Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
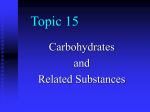
CARBOHYDRATES Table 5.6 67 Major polysaccharide food additives Type Variants Features Properties Usage Cellulose Carboxy methyl p(1->4)-D-Glucans Water-insoluble Thickening agent Pectins High methoxy, low methoxy, modified Galacturonans with few side-chains Methoxyl varies with source High methoxy pectins gel in sugar solutions at low pH Low methoxy forms gel with Ca in dilute solution Very widely used as stabilizer and emulsifier, and as the setting agent in jams Gums Guar Locust bean Tragacanth Arabic Polymers of glucose, galactose, mannose, arabinose, rhamnose and uronic acids May be methoxylated or acetylated Form viscous solutions Wide use in foods as emulsifiers, stabilizers and thickeners Algal Alginates Copolymers of D-mannuronic and L-guluronic acids Insoluble in cold water; Na, K, NH4 salts and propylene glycol esters very soluble Widespread use in many foods; milk, puddings, dairy products, ice cream, beer, confectionery, etc. Carrageenans Mixed galactose and sulphated galactose polymers One type gels strongly with potassium ions to give a brittle gel One type gels strongly with calcium ions to give an elastic gel One type is non-gelling Very widely used in a large number of types of foods Exhibit synergic effects (on physical properties) with proteins Xanthans Glucose, mannose and glucuronic acid in a linear chain with mannose side-chains with pyruvate as a side-chain Non-gelling; soluble in hot and cold water giving viscous solutions Used as a stabilizing agent Often used in combination with plant gums Polydextrose Highly branched, synthetic, glucose polymer Water-soluble Used as a low-calorie filler Neosugar Short chains of fructose Water-soluble Used as a low-calorie fat substitute In the plant, NSP are responsible for the rigidity of cell walls. Plant cell-wall NSP may be isolated and fractionated into more or less purified preparations. Table 5.6 lists these and some other polysaccharides used as food additives. CARBOHYDRATE CONTENT OF FOODS Table 5.7 gives values for the sugar, starch and NSP content of a selection of plant foodstuffs. A good source of further values is the McCance & Widdowson food tables and supplements (e.g. Holland et al 1988, 1991). INTAKES OF DIETARY CARBOHYDRATES Table 5.8 shows fibre intakes estimated on the basis of household food surveys in European countries. There is a wide range, from 11.8 g per person per day in the UK to 24.7 g per person per day in Italy. The average intake value for the countries using mostly enzymic-chemical methods to measure fibre is 16.6 g per person per day, and it is 20.3 g per person per day for those countries using mainly enzymic-gravimetric methods (Cummings 1993). Urban populations from Denmark, Finland and Japan have NSP intakes similar to those in Britain, although rural communities in these countries tend to consume more. Present-day intakes of dietary fibre in affluent countries are generally lower than they have been in the past, when there was a greater dependence on lightly processed carbohydrate foods. Data for intakes of other carbohydrate fractions are less plentiful but daily intakes per capita of about 90 g of sugars and 130 g of total starch per day are given for the UK National Food Survey, and rather consistent intakes per capita of about 3 g of resistant starch per day have been calculated for adults in several European countries. Carbohydrate intakes in the developing world are not well documented but there are some data from The Gambia, West Africa: estimated daily intakes per person of 375 g of starch and 25 g of NSP for adult males have been reported, with lower value for women and children, reflecting their lower body weights (Hudson & Englyst 1995). There are also some data from Latin America; when adjusted for estimates of energy intakes, the NSP intakes of rural Mexican men and women were similar to those in Africa (Sanchez-Castillo et al 1997). DIGESTION AND ABSORPTION OF CARBOHYDRATES The small intestine The digestive process begins in the mouth, where chewing breaks up the structure of compact food and mixes it 68 NUTRITIONAL SCIENCE Table 5.7 The carbohydrate content (g/100 g as eaten) of foods (NSP, non-starch polysaccharide) Food Sugars Starch NSP Cereals All-Bran Barley, pearled Bran, wheat Brown bread Brown rice Buckwheat Corn flakes Cornflour Crispbread Croissants Digestive biscuit Gingernut biscuit Granary bread Hot cross bun Macaroni Mince pie Naan bread Noodles, egg Oat & wheat bran Oat bran flakes Pitta bread, white Porridge Puffed Wheat Rice Krispies Rye bread Scones, plain Scones, wholemeal Shortbread Shredded Wheat Spaghetti, white Spaghetti, w/meal Sweetcorn, kernels Water biscuit Weetabix Wheat flour, brown Wheat flour, white Wheat flour, w/meal Wheatgerm White bread White rice 19.0 0 3.8 3.0 0.5 0.4 7.2 0 3.2 1.0 13.6 35.8 2.2 23.4 0.3 28.1 5.5 0.2 16.7 16.8 2.4 0 0.3 10.6 1.8 5.9 5.9 17.1 0.8 0.5 1.3 9.6 2.3 5.2 1.7 1.5 2.1 16.0 2.6 0 27.6 27.6 23.0 41.3 31.6 84.5 77.7 92.0 67.4 37.2 55.0 43.3 44.1 35.1 18.2 30.9 44.6 12.8 51.0 57.2 55.5 9.0 67.0 79.1 44.0 47.9 37.1 46.9 67.5 21.7 21.9 16.6 73.5 70.5 66.8 76.2 61.8 28.7 46.7 30.9 24.5 1.6 36.8 3.5 0.8 2.1 0.9 0.1 11.7 1.6 2.2 1.4 4.3 1.8 0.9 2.1 1.9 0.7 17.9 10.0 1.6 0.8 5.6 0.7 4.4 1.9 5.2 1.9 9.8 1.2 3.5 1.4 3.1 9.7 6.4 3.1 9.0 15.6 1.5 0.1 1.4 2.6 5.8 8.8 0.9 0.9 3.0 1.5 2.0 4.6 1.0 0.6 1.9 0 0.2 9.3 0.7 4.3 0 0.3 15.6 0.1 0.2 16.6 29.5 0.1 1.4 2.3 3.5 1.9 5.4 2.3 3.1 5.2 1.8 2.5 4.3 2.2 1.2 Vegetables Asparagus Aubergine Baked bean Beetroot Broad bean Broccoli, green Brussels sprouts Butter bean Cabbage Carrot Chickpea Chips, fried Courgette with saliva containing an amylase (ptyalin), but this phase is relatively short, the amylase being inactivated by the gastric acid when the food bolus is swallowed and broken up in the stomach. Digestion occurs mainly in the small intestine through the action of pancreatic aamylase, which hydrolyses starch to dextrins and maltose. In the brush border of the intestinal epithelium there are glucosidases that further reduce the dextrin, and Food Sugars Starch Cucumber Kidney bean, red Lentil, red Lettuce Marrow Mushroom, fried Okra Old potato Onion, fried Parsnip Plantain, fried Potato crisps Radish, red Runner bean Tomato Turnip Watercress Yam 1.4 3.6 0.8 1.7 1.4 0.1 2.3 1.0 10.0 5.9 11.5 0.7 1.9 2.0 3.1 1.9 0.4 0.7 0.1 12.8 16.2 0 0.2 0.2 0.5 14.5 0.1 6.4 36.0 52.6 0 0.3 0 0.1 0 32.3 0.6 6.2 1.9 0.9 0.6 1.5 3.6 1.1 3.1 4.7 2.3 5.3 0.9 1.9 1.0 1.9 1.5 1.4 4.2 11.8 7.2 0.5 5.1 7.6 2.4 5.6 11.5 8.6 48.6 18.5 6.8 15.4 4.0 10.3 14.3 13.8 4.2 9.0 0 8.5 5.8 8.8 6.2 10.0 10.1 8.3 19.7 4.6 7.6 6.0 1.7 8.0 2.6 2.7 0 0 0 0 0 0.7 13.2 0 0 0 0 0 0 2.0 0.3 0 0.3 0 0 0 0 0 0 6.3 0 0 0 0 0 0 0 16.3 0 0.7 7.4 1.8 1.7 3.4 3.1 3.1 4.3 3.2 0.9 1.6 6.9 1.7 1.3 0.7 6.5 1.9 0.7 2.6 1.0 1.2 2.9 1.7 3.3 2.2 6.2 2.2 1.2 1.5 2.4 2.5 0.8 1.1 6.0 1.3 3.5 Fruits and nuts Almond Apple Apricot Avocado Blackberry Blackcurrant Brazil nut Cashew nut Cherry Damson Fig Gooseberry Grapefruit Grape Hazelnut Kiwi fruit Lychee Mango Melon, Cantaloupe Nectarine Olive Orange Passion fruit Paw-paw Peanut Pear Pineapple Plum Prune, canned Raspberry Rhubarb, canned Strawberry Sunflower seed Tangerine Walnut NSP specific disaccharidases that hydrolyse maltose, sucrose and lactose into their constituent monosaccharides (glucose, fructose and galactose); these are transported across the epithelial cells and enter the portal vein (see Figure 5.1). Free concentrations in the intestine or at the mucosal surface are likely to be high enough for passive or facilitated absorption, but as concentrations fall, active transport against a concentration gradient becomes CARBOHYDRATES Table 5.8 Fibre intakes in Europe (after Cummings 1993) Country Amount (g per person/day) Year(s) Analytical method(s) Croatia Yugoslavia Denmark France Germany (GDR) 19.0 20.6 19.1 15.9-17.5 17.3 (female) 20.7 (male) 24.7 18 22.4 15.1 11.8 1990 1990 1987 1972-1989 1988 1988 1980-1984 1990 1991 1991 1989 a a a, b a, d c c b +d d d a a Italy Norway Spain UK Methods: a, NSP, Englyst; b, Association of Official Analytical Chemists (AOAC), Prosky; c, other gravimetric; d, Southgate or mixed. necessary, which requires energy. The active transport system is similar to that responsible for the absorption of glucose from the renal tubules, and involves the breakdown of ATP and the presence of Na + . Different sugars compete for transport, and galactose and glucose are absorbed faster than fructose. Surprisingly, glucose, dextrins and some forms of starch are digested and absorbed at equal rates (Wahlqvist et al 1978), indicating that luminal digestion of these soluble glucans per se is not a limiting factor in glucose absorption. The rate of digestion and absorption of carbohydrate from the small intestine plays a major role in determining the metabolic effects of dietary carbohydrate. Factors that reduce this rate include the presence of intact plant cell walls, the dense physical structure of starchy foods (see later), and the presence of proteins and fats. The slowing of small intestinal absorption by increased meal frequency (nibbling or grazing) results in reduced insulin secretion and lower low-density lipoprotein (LDL) cholesterol concentrations (Jenkins et al 1995). lactose-intolerant individuals, SCC, and synthetic carbohydrates such as Polydextrose and Neosugar. Together these provide about 5 g of carbohydrate per day in a UK diet. In addition, an unknown amount of substrate is available in the form of mucin secretions into the large gut. All the carbohydrates that reach the large intestine (sugars, SCC, RS and NSP) may be fermented by the colonic microflora, with the production of short-chain fatty acids (SCFAs) and gases (Figure 5.2). The rate and extent of fermentation depends on the form and solubility of the substrate. Soluble carbohydrates such as pectin are degraded almost completely, whereas insoluble polysaccharides, especially in lignified material such as wheat bran, are more resistant. Initially, polymers are enzymatically hydrolysed into their constituent monomers (mainly glucose, galactose, arabinose, xylose and uronic acids). The sugars are converted to pyruvate via the glycolytic pathway. Various routes may be followed, depending on the microbial species present and the identity of the substrate. The principal SCFAs produced from all substrates are acetate, propionate and butyrate; other organic acids such as isobutyrate, valerate, isovalerate, lactate and succinate may be produced in small amounts. The SCFAs are the predominant anions in the large intestine and contribute to the relatively low pH (5.6-6.6) of the colon contents. The efficiency of SCFA production and the molar ratios of acetate, propionate and butyrate generated from carbohydrate differ according to the identity of the substrate (Table 5.5). For example, the fermentation of starch yields SCFA with about 29% as butyrate. In contrast, only 2% of the SCFA generated from the fermentation of pectin is in the form of butyrate. Acetate and propionate are rapidly absorbed from the colon and carried in the portal vein to the liver. In experiments with healthy human subjects, it was shown that acetate and propionate enhanced the absorption of calcium from the distal colon The large intestine A variety of potentially fermentable organic molecular species, including carbohydrates, fats and proteins, escape digestion in the small intestine. Studies using ileostomy subjects (people who have had the large intestine removed for medical reasons) have shown that dietary NSP are virtually completely recovered in the ileostomy effluent (Englyst & Cummings 1985) and will therefore be available as substrates for fermentation in the large intestine of intact subjects. With normal epithelial turnover in adults on a Western diet, endogenous carbohydrates from mucin and glycoproteins that line the small intestine contribute 3-5 g of fermentable substrate per day. Other potential substrates for colonic fermentation include fructose and other poorly absorbed monomers, sugar alcohols, lactose in 69 Carbohydrates reaching the large intestine Carbon dioxide Hydrogen Methane Microbial metabolism Energy •* I Acetate *" Butyrate Propionate Ammonia Microbial growth Breath & flatus Fig. 5.2 Faeces Blood Fermentation of carbohydrates in the large intestine. 70 NUTRITIONAL SCIENCE (Trinidad et al 1996) and there is some evidence that absorption of acetate in the rectum and colon is influenced by the presence of calcium and propionate (Wolever et al 1995). SCFAs play an important role in the regulation of the absorption of water and sodium from the colon. Butyrate is the preferred fuel for human colonocytes, particularly in the distal colon (AfonsoRodriguez et al 1995), and it is actively metabolized to ketone bodies (acetoacetate and P-hydroxybutyrate), carbon dioxide and water. The use of butyrate rather than glucose or glutamine by the colonic epithelium is thought to have beneficial effects; an antitumour action has been demonstrated in vitro (Kim et al 1982, Krupitza et al 1996). Most SCFAs are cleared by the liver, with only acetate released (Pomare et al 1985) to be used as a fuel by peripheral tissues (Skutches et al 1979). Propionate is utilized within the liver, where it may modify carbohydrate and lipid metabolism. The main gases produced during fermentation are hydrogen and carbon dioxide. Some individuals have the capacity to produce methane (CH4) from C 0 2 and H 2 , thus diminishing the total volume of gas accumulating in the colon (C0 2 + 4H 2 CH 4 + 2H 2 0). In others, sulphate-reducing bacteria incorporate hydrogen into hydrogen sulphide, particularly after a high intake of dietary sulphate (Christl et al 1992). Excretion of gases per rectum occurs when production of gas exceeds the absorptive capacity of the colon, but at low levels the gases are largely absorbed and excreted through the lungs. Measurement of the hydrogen expired in breath is used as a marker for carbohydrate fermentation (Anderson et al 1981) and maybe useful in a clinical setting to detect pancreatic insufficiency. However, this technique cannot be used for reproducible assessment of the quantity of carbohydrate entering the colon (Cummings & Englyst 1991). All dietary fats, proteins and carbohydrates escaping digestion and absorption in the small intestine contribute directly or indirectly to faecal bulk. However, dietary fibre (NSP) is the only food fraction that has been shown to have a universal effect on stool weight. Two factors are involved in the faecal bulking effect of dietary fibre. Soluble fibre is readily fermented and leads to increased faecal weight through proliferation of the bacterial population. Insoluble fibre, especially in lignified material like wheat bran, partially survives the fermentation process and acts directly as a bulking and water-holding agent. Stool weight is closely associated with transit time. Faecal weights below 150 g/day are associated with increasing transit time, and constipation commonly occurs if the faecal output falls below 100 g/day. Transit time is the time taken for a meal to pass from the mouth to the anus, which may be measured by administering a marker by mouth and measuring the time taken for this to appear in the faeces. The marker may be a dye such as carmine red, or a capsule of tiny radioopaque plastic shapes that can be detected by X-rays. It is convenient to divide whole-gut transit time into two phases, mouth-to-caecum transit, and colonic transit, which takes approximately 10 times as long. Mouth-to-caecum transit is affected by the rate of gastric emptying and by small-intestinal transit, both of which may be altered by the consumption of viscous polysaccharides such as guar gum and gum tragacanth, and by the soluble (3-glucans in oat bran. The viscosity of these polysaccharides delays gastric emptying, resulting in greater satiety and a slow delivery of nutrients to the small intestine (Holt et al 1979). Viscous polysaccharides delay the absorption of nutrients such as sugars within the small intestine, particularly in the distal regions where the viscosity is increased by the absorption of water from the gut contents. Colonic transit is influenced less by the viscosity of polysaccharides, which is rapidly reduced as fermentation proceeds. Insoluble polysaccharides and largely intact cereal products like wheat bran decrease colonic transit time, resulting in larger, softer stools. It is probable that a number of different factors, including the retention of fluid in the fibre matrix, the presence of poorly absorbed SCFA such as lactic acid, a low pH, which inhibits salt and water absorption, an increase in bacterial cell mass and distension due to gas production, all contribute to the decrease in intestinal transit time. THE IMPACT OF MODERN DIETARY CARBOHYDRATES ON PUBLIC HEALTH The world's most abundant staples are rich in carbohydrates, and the site and rate of digestion of these carbohydrates, both highly dependent on processing, have significant implications for health. The human digestive system is evolutionarily adapted to the diet that prevailed until the Agricultural Revolution about 10 000 years ago. In comparison with the modern 'Western' diet, the pre-agriculture diet contained less fat and far more dietary fibre (plant cell walls). Carbohydrates in the pre-agriculture diet were derived mainly from roots, seeds, fruits and tubers; cereal grains were not a major component of this diet. The natural encapsulation of starch and sugars within undamaged plant cell walls (dietary fibre) in the raw or only lightly processed foods typical of that diet slows the rate of digestion, resulting in a sustained release of glucose. In a classic study, using apples, apple pulp and apple juice, Heaton and colleagues (Haber et al 1977) demonstrated that the rate and extent of increases in blood glucose (the glycaemic response) and insulin levels were correlated with the extent of destruction of plant cells by processing. The same effect has since been shown for a range of foods, CARBOHYDRATES including wheat, rice and potato (Heaton et al 1988). Modern starchy food products are mainly cereal-based and often finely milled, which disrupts the plant cell walls, and the starch is often fully gelatinized during processing. The release of sugars and starch from within the cell walls, which may be removed during refining, and the gelatinization of the starch lead to rapid digestion and absorption of the starch in the small intestine, in contrast to the fate of the starch in the pre-agriculture diet. There are strong indications that the large amounts of rapidly available glucose derived from starch and free sugars in the modern diet, in combination with the consumption of discrete meals, lead to periodic increases in plasma glucose and insulin levels that are detrimental to health in many contexts, including diabetes, coronary heart disease, cancer and ageing. The evolutionary timescale is too long to expect that there has been any significant adaptation of the human gut to the cerealbased diets introduced during the Agricultural Revolution and certainly not to the highly processed foods in the modern diet. Current knowledge of the fate of dietary carbohydrates means that the potentially undesirable properties of many modern foods could be altered by using processing techniques that yield foods with more intact plant cellwall structures. Such products would more closely resemble the foods in the pre-agriculture diet with respect to the rate of digestion and absorption of carbohydrate in the small intestine, which would be of great benefit to public health. Dietary fibre National dietary guidelines recommend consumption of a naturally high-fibre diet. This diet is low in free sugars, salt and fat, and is a good source of a range of naturally occurring nutrients, including vitamins, minerals and antioxidants. Any definition or measurement of dietary fibre must lead to values that guide the consumer in the choice of the naturally high-fibre diet recommended in the guidelines. The common characteristic of the plant foods that comprise this largely unrefined high-fibre diet is the presence of naturally occurring plant cell walls. This is what prompted Trowell (1972) to offer the following definition of dietary fibre material: '... the skeletal remains of plant cells that are resistant to hydrolysis by the enzymes of man'. This specific focus on the skeletal remains of plant cells deliberately excluded starch and other non-cell-wall material, and provided the source definition of dietary fibre as endogenous plant cell-wall material (Trowell 1972, Trowell et al 1985). Any analytical procedure capable of measurements reflecting this material would provide meaningful values in terms of the dietary fibre hypothesis (Englyst & Hudson 1996). 71 The argument put forward by some of the food industry (Bar 1994), that all the carbohydrates that reach the large intestine have 'fibre-like' properties and should be included as dietary fibre, is not supportable. In effect, this is proposing a new hypothesis: namely, that all carbohydrates that reach the large intestine, irrespective of origin or composition, are beneficial to health. There is no evidence to support this (Johnson & Southgate 1993). There is no justification for the inclusion of retrograded starch, or indeed any carbohydrate other than the plant cell-wall NSP in the definition and measurement of dietary fibre. Only the plant cell-wall NSP are characteristic of the plant foods that constitute a true high-fibre diet for which health benefits are known. It is important to recognize that the beneficial effects associated with unrefined plant foods cannot be restored by adding 'fibre supplements' to fibre-depleted foods. The structural integrity of the naturally occurring plant cell wall must be retained. Starch digestion and absorption The gross physical form of food, the susceptibility of starch granules to enzymatic hydrolysis and to retrogradation after cooking have a major effect on the rate and extent of starch digestion and absorption in the small intestine. Thus the way food is processed and prepared in the factory and/or at home is of great importance. Starch contained within discrete structures such as whole grains and seeds is physically inaccessible to pancreatic amylase. Crushing, chopping and milling all increase the accessibility of the starch, i.e. the rate of digestion is influenced by the final particle size (Crapo & Henry 1988, Heaton et al 1988, O'Donnel et al 1989). In foods such as pasta, starch hydrolysis is retarded by the density of the product (Bornet et al 1990, Hermansen et al 1986), which decreases enzyme access. Physical inaccessibility may cause the rate of starch hydrolysis to be so slow that some starch enters the large intestine. In extreme cases, starch contained within discrete structures may be excreted in the faeces. Cooking facilitates the hydrolysis of starch through gelatinization and dispersion of the starch granules. However, foods eaten raw retain their starch as granules, which show varying degrees of resistance to digestion. Raw starch from cereals is digested slowly within the small intestine, giving a modest glycaemic response. Raw starch from banana and potato shows a greater degree of resistance, up to 90% passing undigested through the small intestine (Englyst & Cummings 1986, Silvester et al 1995). Retrogradation also retards digestion, and retrograded starch (mainly amylose) from processed cereal and potato products has been shown to pass through the small intestine (Englyst & Cummings 1985). Table 5.9 shows how the digestibility of starchy foods 72 NUTRITIONAL SCIENCE Table 5.9 The effects of food processing on the in vitro digestibility of wheat starch. The values are expressed as a percentage of total starch White flour Shortbread White bread White spaghetti RDS SDS 49 56 94 52 48 43 4 43 RS, RS2 RS3 3 — — — — 3 — trace 1 2 3 RDS, rapidly digestible starch; SDS, slowly digestible starch; RS, resistant starch; RS,, physically inaccessible; RS2, resistant granules; RS3, retrograded amylose. varies with the type of food processing. Raw white wheat flour, which consists mainly of ungelatinized starch granules, is digested relatively slowly, 48% of the starch measuring as slowly digestible starch (SDS). Baking the flour into shortbread, which involves cooking in the presence of very little water, results in limited disruption of the granular structure and gives a product that is also digested slowly. On the other hand, baking the flour into bread, a process that requires a long cooking time in the presence of water, leads to extensive gelatinization of the starch granules and results in a rapidly digestible product. A small amount of retrograded amylose (RS3) is produced during cooling. The starch in wheat flour made into spaghetti is digested more slowly than that in bread, despite being cooked by moist heat. This is because the dense structure of the pasta impedes enzymic hydrolysis of the starch; 3% of the starch is measured as RSj (physically inaccessible). Other examples of foods in which some of the starch may be physically inaccessible are haricot beans and pearl barley. Normal food processing results in only small amounts of RS. The UK diet provides an average of about 3 g of RS per capita per day and there is no evidence that these modest amounts of RS are detrimental to health. However, certain types of processing and the addition of, for example, high-amylose corn starch may result in substantial amounts of RS in foods. Fermentation of RS in the human large intestine has been shown to reduce faecal ammonia, which is potentially beneficial to health. The SCFAs produced by fermentation of carbohydrates, including RS, have been implicated as a protective factor against colon cancer. However, recent studies have shown that RS can enhance tumour formation in rats (Young et al 1996), and in a mouse model (Burn et al 1996). Although detrimental effects have been shown only in animal studies, the desirability of increasing levels of RS in foods requires further evaluation. hydrate-containing foods, and allows foods to be ranked on the basis of the rate of digestion and absorption of the carbohydrates that they contain (Frost et al 1993). Because GI values are normalized to a reference amount of carbohydrate, they do not take into account the amounts of carbohydrate present in foods; e.g. a food with a low content of carbohydrates may nevertheless have a high GI value if that carbohydrate is digested and absorbed rapidly in the human small intestine. This is potentially confusing for a person wishing to control his or her blood glucose levels by the choice of foods. Rapidly available glucose (RAG) is the sum of free glucose, glucose from sucrose and glucose from RDS. RAG values are determined in vitro as the glucose released under strictly controlled conditions of extraction and hydrolysis with pancreatin, amyloglucosidase and invertase (Englyst et al 1992). The values are expressed as grams of glucose per 100 grams of food as eaten. The measurement of RAG provides values that reflect the amount of glucose likely to be rapidly absorbed, and thus to influence blood glucose and insulin levels. These values can be used to compare foods on an equal weight basis, and are important indicators for the consumer, as food table RAG values can be used for simple calculation of the total amount of rapidly available glucose likely to be provided by single foods, by whole meals and by whole diets. When the values for 39 foods (Englyst et al 1996a) were expressed on the basis of the available carbohydrate content of these foods, highly significant (P < 0.001) positive correlations were observed between GI and both RDS and RAG. This correlation between RAG intake and glycaemic response has been confirmed with a small number of carbohydrate-rich foods over a range of RAG intakes (Englyst et al 1999). There has been some controversy over the application of the glycaemic index to mixed meals (Wolever & Bolognesi 1996). This has led to recommendations from the American Diabetes Association (1994) that focus on the total amount of carbohydrate consumed rather than the source of the carbohydrate. Part of the problem may be the complexity of using the glycaemic index in a mixed diet, as it gives no information on the amount of carbohydrate consumed. This may be overcome by the comparatively simple use of RAG intakes, which clearly indicate the amount of glucose likely to be rapidly absorbed in the small intestine. Meals with a high RAG value will result in elevated levels of blood glucose, i.e. a large glycaemic response, and subsequently raised levels of circulating insulin. The glycaemic response to dietary carbohydrates Non-enzymatic protein glycation The glycaemic index (GI; Jenkins et al 1981) is an in vivo measurement based on the glycaemic response to carbo- Elevated levels of blood glucose are responsible for increased non-enzymatic protein glycation, which is CARBOHYDRATES implicated in the development of diabetes complications and the ageing process (Dyer et al 1993, Vlassara & Bucala 1996). The importance of the reaction of reducing sugars with amino acids in living organisms has been appreciated only recently. Initial studies of this process were centred on the biochemical abnormalities that occur in diabetes, an illness characterized by high levels of blood glucose (Koenig & Cerami 1975). The reaction products that form in vivo have been termed advanced glycosylation end-products or AGEs (Bucala et al 1992). The amount of carbohydrates linked to haemoglobin and other proteins is increased in diabetes, and has proved to be a useful marker for glycaemic control of diabetic patients (Jovanovic & Peterson 1981). In a large trial (Shamoon et al 1993), levels of the glycated haemoglobin HbAlc (Koenig et al 1977) were 9% in normally controlled diabetics but were only 7.5% in those whose blood glucose was measured many times a day. This lowering was associated with a dramatic decrease (75-90%) in the number of patients who developed complications of diabetes over a period of 9 years, demonstrating the long-term detrimental effect of high levels of blood glucose. Yellow-brown pigments accumulate in the lens with age and do so at an accelerated rate in diabetics. These pigments are capable of cross-linking proteins, a hallmark of cataract formation (Monnier & Cerami 1981). Protein cross-linking has been observed also for collagen, and again the levels are higher in diabetics (Dyer et al 1993). Macrophages have been shown to possess specific AGE receptors that could mediate the uptake and eventual breakdown of AGEs (Vlassara & Bucala 1996). The net accumulation of AGEs reflects the balance of the reaction of glucose with the matrix proteins and their removal by the macrophages. The amino groups of the bases of DNA react with reducing sugars. Although DNA is not exposed to the high levels of glucose circulating in the blood, DNA is very long-lived and might be expected to accumulate AGEs. The DNA in older animals has been shown to be cross-linked both to itself and to proteins (Bojanovic et al 1970). The incidence of birth defects in children born to diabetic mothers is increased many-fold, and animal studies have shown an increased rate of mutations in embryos that were exposed to hyperglycaemia in utero (Lee et al 1995). Increased levels of glycation on proteins with modest half-lives reflect recent increases in glucose levels. On more stable proteins, the initial glycation products become irreversibly fixed and the accumulation of AGEs represents a measure of exposure to glucose over time. The cross-linking of AGEs with a second protein has been proposed as the pathway of collagen cross-linking that increases tissue stiffness, which may lead directly or indirectly to kidney failure (Drickamer 1996). 73 Causes and consequences of elevated insulin levels The rise in plasma glucose that follows a carbohydratecontaining meal (the glycaemic response) is accompanied by the production of insulin from the beta cells of the pancreas. Insulin is required to facilitate the transport of glucose across cell membranes. Insulin homeostasis is restored by the production of insulin antagonists (e.g. adrenaline and Cortisol) within 1-2 hours in normal individuals. If the sensitivity of cells to insulin becomes impaired, the body will respond by producing more insulin and circulating levels may remain high (hyperinsulinaemia). Basal levels of circulating insulin tend to increase with age, and hyperinsulinaemia is strongly associated with adiposity (Eckel 1997, Mayer-Davis et al 1997), especially central fatness in men, and with lack of fitness due to inactivity (Helmrich et al 1991, Manson et al 1991). The amount of insulin produced in response to a meal is related to a number of factors, including the rate at which sugars are absorbed in the small intestine. Elevated levels of insulin are associated with dyslipidaemia (Despres et al 1996), atherosclerosis (Stout 1996) and the formation of tumours and increased tumour growth in a number of cancers (Giovannucci 1995; McKeown-Eyssen 1994). Rapidly absorbed sugars tend to enter the lipogenic pathway and hence predispose to the obesity that is so common in the modern Western world. It has been hypothesized that insulin promotes the growth of colon tumours, and this has been demonstrated in animal models (Tran et al 1996). Breast cancer is associated with an elevated number of insulin receptors, and there is some evidence that hyperinsulinaemia or its determinants, such as waist-to-hip ratio, increases the incidence of breast cancer. If the hypothesis is correct, the determinants of serum insulin levels should influence the risk of both colon and breast cancer. Fasting serum levels are affected by insulin sensitivity, and postprandial levels depend on how quickly glucose is absorbed in the small intestine. Most modern people are relatively sedentary, and the combination of inactivity, ready access to energy-rich foods and consumption of considerable amounts of food at discrete meals often leads to obesity and tissue resistance to insulin. This insulin resistance results in the inability to cope with the increased blood glucose caused by rapid absorption of the carbohydrates in modern sugary and starchy foods. The highest levels of circulating insulin occur after a meal, with the level depending on (1) the amount of carbohydrates in the meal, (2) their form, and (3) the degree of insulin sensitivity. The rate at which starch is hydrolysed depends on a number of factors (see above). In general, the starch and sugars in modern processed 74 NUTRITIONAL SCIENCE foods are digested and absorbed more rapidly than those in raw or traditionally cooked foods. Encapsulation of nutrients by plant cell-wall material is an important factor in moderating the glycaemic response. It must be emphasised that this and most other beneficial effects of a naturally high-fibre diet cannot be achieved by the addition of 'fibre supplements' to fibre-depleted foods (as discussed above). The range of factors considered as risks for non-insulindependent diabetes mellitus (high body mass index, central obesity, high energy intakes, high sugar intakes, high saturated fat intakes, low fibre intakes) have all been identified as risk factors for colon cancer. There are strong indications that elevated plasma glucose and insulin responses are the common factors. Support for the promotion of colon cancer by insulin has come from animal studies (e.g. see Tran et al 1996). CONCLUSIONS National dietary guidelines recommend an increase in intake of dietary fibre and starch. The recommendations for fibre intakes are based on the proven health benefits of a naturally high-fibre diet (see above) and are made in terms of obtaining fibre in the form of a balanced mixture of fruits, vegetables and whole grains. The guidelines discourage the use of 'fibre supplements' as a source of dietary fibre, and there is some evidence to suggest that these supplements may be detrimental to health (Jacobs 1983, Jacobs & Lupton 1986, Wasan & Goodlad 1996). The recommendations to eat more starch are related to the recommendations to eat less fat, with starch being a cheap and readily obtainable alternative energy source. However, recent advances in our knowledge of the physiological consequences of eating sugars and starch that are rapidly digested and absorbed in the small intestine suggest that, as for fibre, the form as well as the amount of starch should be considered. Carbohydrates that are digested and absorbed rapidly are potentially detrimental to health in many areas, as discussed above. It is pertinent to ask whether food labels provide values that aid consumers in selecting a healthy diet. The entry 'carbohydrate' is required in most countries, and the value is usually obtained 'by difference' and used in the calculation of energy content, but the value provides no nutritional information per se. Many processed foods carry second-level entries, preceded by 'of which', and here one might expect to find values for sugars, starch and fibre. High values for sugars correctly serve as a warning to the consumer. Since the starch may be in the form of RDS, SDS or RS, or any mixture of these in any proportions, a single value for starch is impossible to interpret in nutritional terms. High levels of RDS result in elevated plasma glucose and insulin levels known to be detrimental to health (McKeown-Eyssen 1994). As discussed in this chapter, the benefits or otherwise of RS are unknown. The small amounts of RS in the Western diet may prove to be beneficial, but large supplements of RS are potentially detrimental to health. There is a bona fide case for considering how best to indicate the likely rate and extent of digestion and absorption of starch on the food label; a third-level entry under starch 'of which rapidly digestible' or perhaps a new entry of RAG under carbohydrate would go some way to addressing the problem. Whatever decision is taken by the legislators, there must be public education concerning the potential dangers of consuming large amounts of carbohydrates that will be rapidly digested and absorbed in the small intestine. In countries where food label values for fibre are measured as naturally occurring plant cell-wall NSP, the labelling for fibre provides the consumer with accurate information. In countries where fibre values are obtained by non-specific gravimetric procedures, however, the values are not confined to naturally occurring plant cell-wall NSP. Indeed, these values may represent solely material such as retrograded starch, formed as the result of food processing, or substances added to foods. Such labelling cannot guide the consumer in the choice of naturally fibre-rich foods and may mistakenly encourage the choice of foods with added 'fibre supplements', in contradiction to the advice given in the guidelines. The recent advances in our knowledge of the importance of dietary carbohydrates represents an opportunity for the food industry to make a significant contribution to public health by restricting the use of the term 'fibre' to naturally occurring plant cell walls, by preserving the natural structure of plant foods as far as possible, and by the development and marketing of starchy foods that are more compatible with human physiology. This, together with nutritionally sound food labelling for dietary carbohydrates, would be of great benefit to public health. CARBOHYDRATES 75 KEY POINTS • Dietary carbohydrates are classified into four major groups: (1) free sugars; (2) short-chain carbohydrates; (3) starch; and (4) non-starch polysaccharides (NSP). • The in vitro measurement of rapidly available glucose (RAG; RDS and free-sugar glucose) provides information about the likely glycaemic response to plant foods. • The site, rate and extent of digestion of carbohydrates, which are highly dependent on food processing, have significant implications for health. • The measurement of dietary fibre as NSP provides a good marker of the unrefined plant foods for which benefits to health are known. • Starch is subdivided into rapidly digestible starch (RDS), slowly digestible starch (SDS) and resistant starch (RS). • Most of the carbohydrate that reaches the large intestine is fermented by the colonic microflora, with the production of short-chain fatty acids and gases. REFERENCES Afonso-Rodriguez J J, Medina-Arana V, Alvarez-Arguelles H, Hernandez-Calzadilla C, Gonzalez-Hermoso F 1995 Cytometric study of colonic tumors in a model of experimental cancer. Impact of the diet. Hospital Nutrition 10:279-285 American Diabetes Association 1994 Position statement: nutrition recommendations and principles for people with diabetes mellitus. Diabetes Care 17:519-522 Anderson I H, Levine A S, Levitt M D 1981 Incomplete absorption of the carbohydrate in all-purpose wheat flour. New England Journal of Medicine 15:891-892 Association of Official Analytical Chemists (AOAC) Official Methods of Analysis 1990 15th edn, vol II, section 985.29. AOAC, Arlington, Virginia, 1105-1106 Bar A 1994 Defining dietary fibre for nutrition labelling purposes: a nutritional/physiological approach. In: Food Ingredients Europe: Conference Proceedings (1993). Expoconsult, Maarssen, The Netherlands Bojanovic J J, Jevtovic A D, Pantic V S, Dugandzic S M, Javanovic D S 1970 Thymus histones in young and old rats. Gerontologia 16:304-312 Bornet F R J, Cloarec D, Barry J-L et al 1990 Pasta cooking time: influence on starch digestion and plasma glucose and insulin responses in healthy subjects. American Journal of Clinical Nutrition 51:421-427 Bucala R, Vlassara H, Cerami A 1992 Advanced glycosylation endproducts. In: Harding J J, James M, Crabbe C (eds) Posttranslational modifications of proteins. CRC Press, Boca Raton, Florida Burn J, Katheuser A, Fodde R, Coaker J, Chapman P D, Mathers J C 1996 Intestinal tumours in the Ape mouse: aspirin not protective and resistant starch increases small bowel tumours. European Journal of Human Genetics 4 (suppl 1):13 Christl S U, Gibson G R, Cummings J H 1992 The role of dietary sulphate in the regulation of methanogenesis in the human large intestine. Gut 33:1234-1238 Crapo P A, Henry R R 1988 Postprandial metabolic responses to the influence of food form. American Journal of Clinical Nutrition 48:560-564 Cummings J 1993 Dietary fibre intakes in Europe: an overview. In: Cummings J, Frolich W (eds) Dietary fibre intakes in Europe. Commission of the European Communities, Directorate-General Science, Research and Development, Office for Official Publications of the European Communities, Luxembourg, pp 11-19 Cummings J H, Englyst H N 1991 Measurement of starch fermentation in the human large intestine. Canadian Journal of Physiology and Pharmacology 69:121-129 Despres J P, Lamarche B, Mauriege P, Cantin B, Lupien P J, Dagenais G R 1996 Risk factors for ischaemic heart disease: is it time to measure insulin? European Heart Journal 17:1453-1454 Drickamer K 1996 Breaking the curse of the AGEs. Nature 382:211-212 Dyer D G, Dunn J A, Thorpe S R, Bailie K E, McCance D R, Baynes J W 1993 Accumulation of Maillard reaction products in skin collagen in diabetes and aging. Journal of Clinical Investigation 91:2463-2469 Eckel R H 1997 Insulin resistance in atherosclerosis. American Journal of Clinical Nutrition 65:164-165 Englyst H N, Cummings J H 1985 Digestion of the polysaccharides of some cereal foods in the human small intestine. American Journal of Clinical Nutrition 42:778-787 Englyst H N, Cummings J H 1986 Digestion of the carbohydrates of banana (Musa paradisiaca sapientum) in the human small intestine. American Journal of Clinical Nutrition 44:42-50 Englyst K N, Englyst H N, Hudson G J, Cole T J, Cummings J H 1999 Rapidly available glucose in foods: an in vitro measurement that reflects the glycemic response. American Journal of Clinical Nutrition 69: 448-454 Englyst H N, Cummings J H 1990 Dietary fibre and starch: definition, classification and measurement. In: Leeds A R (ed) Dietary fibre perspectives: reviews and bibliography. John Libbey, London, pp 3-26 Englyst H N, Hudson G J 1996 The classification and measurement of dietary carbohydrates. Food Chemistry 1:15-21 Englyst H N, Hay S, Macfarlane G Y 1987 Polysaccharide breakdown by mixed populations of human faecal bacteria. FEMS Microbiology and Ecology 95:163-171 Englyst H N, Kingman S M, Cummings J H 1992 Classification and measurement of nutritionally important starch fractions. European Journal of Clinical Nutrition 46(suppl 2):S33-S50 Englyst H N, Kingman S M, Cummings J H 1993 Resistant starch: measurement in foods and physiological role in man. In: Meuser F, Manners D J, Seibel W (eds) Plant polymeric carbohydrates. Royal Society of Chemistry, Cambridge, 137-146 Englyst H N, Quigley M E, Hudson G J, Cummings J H 1994 Determination of dietary fibre as non-starch polysaccharides with gas-liquid chromatographic, high-performance liquid chromatographic or spectrophotometric measurement of constituent sugars. Analyst 119:1497-1509 Englyst H N, Veenstra J, Hudson G J 1996a Measurement of rapidly available glucose (RAG) in plant foods: a potential in vitro predictor of the glycaemic response. British Journal of Nutrition 75:327-337 Englyst H N, Kingman S M, Hudson G J, Cummings J H 1996b Measurement of resistant starch in vitro and in vivo. British Journal of Nutrition 75:749-755