Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Race and health wikipedia , lookup
Public health genomics wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Herpes simplex research wikipedia , lookup
Epidemiology of metabolic syndrome wikipedia , lookup
Seven Countries Study wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Infection control wikipedia , lookup
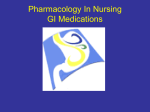
Published by Oxford University Press on behalf of the International Epidemiological Association ß The Author 2013; all rights reserved. International Journal of Epidemiology 2013;42:1873–1881 doi:10.1093/ije/dyt213 Increased incidence of herpes zoster in adult patients with peptic ulcer disease: a population-based cohort study Jen-Yin Chen,1,2,3 Tain-Junn Cheng,4,5,6,7,8 Chia-Yu Chang,4 Kuo-Mao Lan,1 Shih-Feng Weng,9 Ming-Jen Sheu,10 Su-Feng Tseng3 and Miao-Lin Hu2,11* 1 Department of Anesthesiology, Chi Mei Medical Center, Tainan, Taiwan, 2Department of Food Science and Applied Biotechnology, National Chung Hsing University, Taichung, Taiwan, 3Department of the Senior Citizen Service Management, Chia Nan University of Pharmacy and Science, Tainan, Taiwan, 4Department of Neurology, Chi Mei Medical Center, Tainan, Taiwan, 5Department of Occupational Medicine, Chi Mei Medical Center, Tainan, Taiwan, 6Department of Management in Medical Records and Information, Chi Mei Medical Center, Tainan, Taiwan, 7Department of Occupational Safety / Institute of Industrial Safety and Disease Prevention, College of Sustainable Environment, Chia Nan University of Pharmacy and Science, Tainan, Taiwan, 8 Department of Occupational and Environmental Medicine, National Cheng Kung University Hospital, Tainan, Taiwan, 9 Department of Medical Research, Chi Mei Medical Center, Tainan, Taiwan, 10Department of Gastroenterology, Chi Mei Medical Center, Tainan, Taiwan and 11Department of Health and Nutrition Biotechnology, Asia University, Taichung, Taiwan *Corresponding author. Department of Food Science and Applied Biotechnology, National Chung-Hsing University, 250 Kuo-Kuang Road, Taichung, Taiwan 40227. E-mail: [email protected]; [email protected] Accepted 16 September 2013 Background Peptic ulcer disease (PUD) has been linked to immunological dysfunctions and malnutrition—both are predictors of herpes zoster (HZ). We hypothesized that PUD patients might have a greater risk for developing HZ. Methods Using the longitudinal National Health Insurance Research Database, we conducted a retrospective population-based cohort study to evaluate the incidence of HZ in adult PUD patients and controls matched by age and gender. Kaplan-Meier analysis and Cox regression were conducted to compare differences in the development of HZ. The effects of comorbidities on the risk of HZ and the associations between different risk factors of PUD and HZ were assessed by subgroup analyses. Results We identified 41 229 adults PUD patients and 41 229 controls. Over an 8-year follow-up, the cumulative incidence of HZ in PUD patients (11.76/1000 person-years) was significantly higher than controls (6.56/1000 person-years) (P < 0.001, by log-rank test). After adjusting for potential confounders, PUD was an independent predictor for HZ (adjusted hazard ratio: 1.77, 95% confidence interval 1.64–1.91, P < 0.001). Major risk factors of PUD were non-selective nonsteroidal anti-inflammatory drugs (nsNSAID) usage and Helicobacter pylori infection. Subgroup analyses revealed that PUD is an independent predictor of HZ after excluding the potential confounding effects of the comorbidities; PUD associated with the combination of nsNSAID usage and Helicobacter pylori infection leads to greatest risk of HZ. Conclusions Adults with PUD are at increased risk of HZ independently compared with the general population. Further studies are required to clarify the nature of the associations between HZ and PUD. 1873 1874 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY Keywords Retrospective cohort study, peptic ulcer disease, herpes zoster, Helicobacter pylori, non-selective nonsteroidal anti-inflammatory drugs, National Health Insurance Research Database Introduction Herpes zoster (HZ) is a common disease. HZ is caused by a reactivation of latent varicella zoster virus and is characterized by painful rashes. Herpetic pain develops in the acute phase and usually subsides within 2–4 weeks spontaneously. However, approximately 20–25% of HZ patients experience postherpetic neuralgia or other nonpain complications. Any complication substantially increases the cost of HZ-related care. The medical expense of this common disease leads to a substantial burden on the health care system. Diminishing cell-mediated immunity is a well-known risk factor of HZ. Approximately 90% of HZ cases occur among immunocompetent patients.1–5 An HZ vaccine for adults has been available since 2006.6,7 Identifying potentially unfavourable predictors of HZ may help physicians to identify highrisk patients and administer HZ vaccinations to reduce the incidence of HZ. Various diseases linked to impaired immunity such as rheumatic diseases and cancers have been reported to be associated with an increased risk of HZ.8,9 Peptic ulcer disease (PUD) is a gastrointestinal disorder that is common in HZ patients.10 The predominant risk factors of PUD are Helicobacter pylori (H. pylori) infection and the use of non-selective nonsteroidal antiinflammatory drugs (nsNSAIDs), accounting for 48 and 24% of cases, respectively, in the USA.11 In addition to nsNSAIDs, other ulcerogenic medications including aspirin, steroids, chemotherapeutics and cyclooxygenase-2 inhibitors12 are considered risk factors of PUD. H. pylori infection has been linked to extradigestive manifestations including malnutrition and immunological dysregulation.13–16 The usage of nsNSAIDs, aspirin, steroids and chemotherapeutics has been demonstrated to inhibit cell-mediated immunity.17,18 PUD leads to chronic protein/blood loss19 and micronutrients deficiencies,13,16,20 which consequently impair immunity.21,22 Taken together, PUD patients commonly are found to have impaired immunity and nutritional deficiencies. We therefore hypothesized that PUD patients might have a greater risk for developing HZ. However, evidence regarding the association between PUD and the incidence of HZ is limited and worthy of being explored. Methods Data sources We conducted a retrospective cohort study using the longitudinal National Health Insurance Research Database (LNHIRD) containing one million random subjects (about 4% of the enrollees) from 1996–2009 computed by the Taiwan National Health Insurance (NHI) programme. There were no statistical differences in age, gender or income between the sample group and all enrollees. The NHI programme is a nationwide healthcare system in Taiwan, established in 1995. The coverage rate in 2002 was approximately 96% of Taiwan’s entire population.4,9 The NHI electronic data provided encrypted patient identification numbers, gender, date of birth, the ICD-9-CM (International Classification of Diseases, Ninth revision, Clinical Modification), prescription drugs dispensed, medical cost, medical care facilities and specialties. All NHI datasets can be interlinked with each individual personal identification number. Our study was exempted from full review by the Institutional Ethics Committee of Chi Mei Medical Center because we used de-identified secondary data released to the public for research purposes. Study population In the study cohort, we identified adult patients (aged 18 years and older) with PUD by the following criteria: a primary diagnosis with ICD-9-CM code 530-534 concurrent with a claim of gastrointestinal endoscopy (a medical procedure covered by Taiwan’s NHI programme23) and prescriptions for PUD. Based on the reimbursement policy of Taiwan’s NHI, all patients are strictly required to have documented H. pylori infection or endoscopy-confirmed ulcers before receiving H. pylori eradication therapy or antiulcer agents (proton pump inhibitors or histamine2 blockers). Standardized diagnostic methods for detecting H. pylori infection include urea breath test, culture and rapid urease test. Testing and treatments for PUD did not change over time from 2000 to 2008. H. pylori eradication therapy is defined as a triple or quadruple regimen consisting of the following: a proton pump inhibitor or histamine2 blocker, plus clarithromycin or tetracycline, plus amoxicillin or metronidazole, with or without bismuth. Furthermore, patients with a confirmed diagnosis of H. pylori infection are only reimbursed for 2 weeks of antibiotic therapy.23,24 We excluded patients who had diagnostic codes of human immunodeficiency virus infection (ICD-9-CM 042, 043, 044), organ transplants (ICD-9-CM 336, 375, 3751, 116, 1160, 1164, 1169, 505, 5059, 528, 5280, 5283, 556, 5569, 335, 3350–3352), chronic obstructive pulmonary diseases (ICD-9-CM 491, 492, 496), rheumatic diseases (ICD-9-CM 710, 714, 725) PEPTIC ULCER DISEASE INCREASES ZOSTER INCIDENCE and autoimmune diseases (ICD-9-CM 556.9, 555.9, 250.01, 579, 358, 696.1, 696.0, 710.1, 340, 710.2 and 245.2) from the study cohorts and control cohorts because these patients may have been treated with steroids and immunosuppressive medications or suffered from immunosuppressive conditions which are potential confounders of HZ.9,25 Patients were identified by an automatched search12 in either inpatient or outpatient service claims from January 2002 to December 2008. Controls were selected using pair matching by age, gender and year of cohort entry in a ratio of 1:1 through random computerized selection from the remaining subjects in the database who had no diagnostic codes with PUD, and did not take ulcerogenic medications to exclude asymptomatic PUD.26 We collected information from all study subjects including demographic characteristics, treatment modalities, risk factors and comorbidities. Incident HZ cases were identified by an automatch search for codes for HZ and HZ complications (ICD-9 codes 053.0–053.9) present in either an inpatient or outpatient service claim and with treatment modalities for HZ.4 Inpatients and outpatients with primary diagnoses of HZ for the first time between 1 January 2002 and 31 December 2008, were included. We excluded patients with a diagnosis of HZ between 1 January 1996 and 31 December 2001. From the date of cohort entry, all patients were followed until developing HZ or until the end of 2009, whichever was earlier.9 In this study, we used administrative data alone to define cases of HZ for two reasons. First, accuracy of the claims database is routinely monitored by the Bureau of Taiwan’s NHI which performs strict quarterly expert reviews on random samples of every 50–100 ambulatory and inpatient claims for the purpose of reimbursement.1,27,28 Second, a populationbased study in Taiwan reveals that no specific therapy is used for the management of HZ in Taiwan. Common medications used for the treatment of HZ include antiviral agents (23.6%), NSAIDs (61.1%), acetaminophen (49.3%), systemic corticosteroids (14.7%), tricyclic antidepressants (8.9%), anticonvulsants (6.6%) and opiates (3.9%).4 Based on the risk factors of PUD, our study PUD patients were divided into four subgroups for further stratified analyses including: (i) the combination of nsNSAID usage and H. pylori infection; (ii) nsNSAID usage only; (iii) H. pylori infection only; and (iv) Others, where cyclooxygenase-2 inhibitors, aspirin, nonaspirin anticoagulants or other ulcerogenic medications were used.11 H. pylori-associated PUD was identified by the eradication regimens of H. pylori during or after the index PUD.12,23 Potential confounders Comorbidities including diabetes mellitus, cancers and hypertension25 were selected and identified in the 12 months before the index ambulatory care 1875 visits, from inpatient and outpatient diagnoses in both cohorts because these comobidities are potential confounders for HZ. PUD, diabetes mellitus and cancers were not included in the Charlson comorbidity index29 (CCI) scores which included myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, liver disease, hemiplegia, quadriplegia and renal diseases. We assessed the rate of CCI scores greater than 1 in PUD patients by the dichotomized outcome of the Charlson scores. Outcome measures The incidence and hazard ratios (HRs) of HZ over the follow-up period were computed. We performed prespecified subgroup analysis on comorbidities because comorbidities are considered confounders.30 Furthermore, we performed a stratified analysis to assess independent predictors of HZ based on different risk factors of PUD. We also assessed the annual number of HZ patients and the annual incidence for HZ in all adult PUD patients during the follow-up period. Statistical analysis Data processing and statistical analysis were performed using SAS statistical software (Version 9.2; SAS Institute, Cary, NC, USA). Chi-square tests were used to test the differences in categorical data. The differences of the CCI scores and months of followup were considered as continuous variables and were tested by Student’s t-test. Kaplan–Meier analysis was used to calculate the cumulative incidence of HZ between the two groups and the log-rank test was used to test the difference between PUD patients and the controls. The Cox regression model was performed to evaluate the effects of comorbidities to compare the HRs potential. The Cox hazard regressions among different risk factors of PUD were performed to evaluate the effects on HZ in PUD patients. A P value of <0.05 was considered statistically significant. Results We identified 41 229 PUD adults and 41 229 matched controls by age, gender and year of cohort entry from 2002 to 2008. The PUD patients were more likely to suffer from the selected comorbidities and have a higher rate of CCI scores greater than 1 based on the dichotomized outcome of the Charlson scores. Of the total 41 229 PUD patients, 2013 patients experienced HZ during the follow-up period (Table 1). The cumulative incidence of HZ in PUD patients was significantly higher than that of the control cohorts (P < 0.001) over the follow-up period (Figure 1). The incidence of HZ in PUD patients (11.76 per 1000 patient-years) was significantly greater than that in the control cohorts (6.56 per 1876 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY Table 1 Demographic characteristics for adult patients with peptic ulcer disease and control cohorts in Taiwan from 2002 to 2008 Patients with PUD n ¼ 41 229 Number (%) 51.89 (16.28) Variablea Age (years), mean (SD) Control cohorts n ¼ 41 229 Number (%) 51.85 (16.24) P* 0.74 0.99 Age group, years 18-24 1835 (4.45%) 1831 (4.44%) 25-34 4886 (11.85%) 4876 (11.83%) 35-44 8103 (19.65%) 8117 (19.69%) 45-54 9721 (23.58%) 9768 (23.69%) 55-65 6892 (16.72%) 6922 (16.79%) ^65 9792 (23.75%) 9715 (23.56%) Female 19 353 (46.94%) 19 353 (46.94%) Male 21 876 (53.06%) 21 876 (53.06%) Gender Follow-up (months), mean (SD) 50.53 (25.85) 52.88 (25.07) 1.00 <0.001 Comorbidities Diabetes mellitus 5295 (12.84%) Cancers Hypertension 1991 (4.83%) <0.001 1856 (4.50%) 546 (1.32%) <0.001 10 641 (25.81%) 4371 (10.60%) <0.001 32 864 (79.71%) 39 569 (95.97%) <0.001 CCI score 0 ^1 Herpes zoster, number (%) 8365 (20.29%) 1660 (4.03%) 2013 (4.88%) 1174 (2.85%) <0.001 Controls 0.05 PUD Log rank P-value<0.001 0.00 Proportion with herpes zoster 0.10 SD, standard deviation; NTD, New Taiwan Dollars; CCI, Charlson comorbidity index. a Chi-square tests for categorical variables; Student’s t test for continuous variables. *P < 0.001, statistical significance. 0 Number at risk PUD 41229 Controls 41229 2 4 Time (years) 6 8 33202 34506 20710 22135 9880 10728 0 0 Figure 1 Cumulative incidences of herpes zoster for adult patients with peptic ulcer disease and the control cohorts 1000 patient-years). Cox regression revealed that PUD was an independent predictor for HZ after adjusting for potential confounders including age, gender, the selected comorbidities and CCI scores [adjusted HR 1.77, 95% confidence interval (CI): 1.64-1.91; P < 0.001) (Table 2). Adjusted HRs for HZ in PUD patients not suffering from any one of the selected comorbidities were significantly greater compared with those of the controls (no individual comorbidity or PUD). In particular, the adjusted HR of HZ in PUD patients with none of the three selected comorbidities was 1.94 (95% CI: 1.772.12) compared with that of the controls after adjusting for potential confounders (P < 0.001) (Table 3). These results suggest that PUD is associated with an increased risk of developing HZ, independent of other risk factors (selected comorbidities and CCI). Based on the risk factors of PUD, stratified analyses revealed that the adjusted HRs for HZ compared with the control cohorts were ranked from high to low as: the combination of nsNSAID usage and H. pylori infection (2.19, 95% CI: 1.96-2.42); nsNSAID usage only (2.14, 95% CI: 1.95-2.37); H. pylori infection only (1.40, 95% CI: 1.24-1.58); and Others11 (1.34, 95% CI: 1.19-1.50) (Table 4). Our results indicated that any risk factors in the four subgroups of PUD predisposed adult PUD patients to HZ; however, the PEPTIC ULCER DISEASE INCREASES ZOSTER INCIDENCE 1877 Table 2 Incidence and hazard ratios for herpes zoster during the follow-up period for adult patients with peptic ulcer disease versus control cohorts All subjects (n ¼ 90 846) PUD Control HZ 2013 Persons at risk 171 114 Incidence per 1000 person-years 11.76 1174 179 087 6.56 Adjusted HRa (95% CI) 1.77* (1.64–1.91) 1.00 HZ, herpes zoster;HR, hazard ratio. a Adjustments were made for age, gender, and selected comorbidities (diabetes mellitus, cancers, and hypertension) and the Charlson comorbidity index. *P < 0.001 for statistical significance. Table 3 Incidence and hazard ratios for adult patients with peptic ulcer disease and control cohorts concomitant with comorbidities PUD patients Comorbidity Cases Control cohorts (No PUD) HZ Person at risk Incidence per 1000 person-years Cases HZ Person at risk Incidence per 1000 person-years Adjusted HRa (95% CI) P Diabetes mellitus Yes 5295 316 19 555 16.16 1991 98 7963 12.31 1.39 (1.10–1.75) 0.006 No 35 934 1697 151 558 11.20 39 238 1076 171 125 6.29 1.80 (1.67–1.95) <0.001 Cancers Yes 1856 105 5360 19.59 546 25 2031 12.31 1.68 (1.07–2.62) 0.023 No 39 373 1908 165 754 11.51 40 683 1149 177 056 6.49 1.77 (1.64–1.92) <0.001 <0.001 Hypertension Yes 10 641 646 40 560 15.93 4371 209 17 777 11.76 1.42 (1.21–1.67) No 30 588 1367 130 554 10.47 36 858 965 161 311 5.98 1.86 (1.70–2.02) <0.001 27 576 1205 11 9588 10.08 35 541 888 156 022 5.69 1.94 (1.77–2.12) <0.001 None of above PUD, peptic ulcer disease; HR, hazard ratio; HZ, herpes zoster. a Adjusted by age, gender, selected comorbidities and the Charlson comorbidity index. Table 4 Independent predictors of herpes zoster identified by Cox hazard regressions in adult patients with peptic ulcer disease Risk factors of PUD Control cohorts (No PUD) Adjusted HRa (95% CI) 1.00 þ H. pylori þ nsNSAID 2.19* (1.96–2.42) nsNSAID only (- H. pylori; þ nsNSAID) 2.14* (1.95–2.37) H. pylori only (þ H. pylori; - nsNSAID) 1.40* (1.24–1.58) Others (- H. pylori; - nsNSAID) 1.34* (1.19–1.50) PUD, peptic ulcer disease; nsNSAID, non-selective nonsteroidal anti-inflammatory drugs; Others containing usage of cyclooxygenase-2 inhibitors, aspirin, non-aspirin anti-coagulants and other ulcerogenic medications. a Adjusted hazard ratio: adjusted by age group, gender, and three-selected comorbidities. *P < 0.001 for statistical significance. increased incidence of HZ varied with the different risk factors of PUD. PUD associated with the combination of nsNSAID usage and H. pylori infection put patients at the greatest risk of HZ. Over time, a decreased number of patients with HZ among all adult PUD patients annually was noted, from 2002 to 2008. However, the annual incidence of HZ in all PUD patients (ranging from 11.14 to 12.92) did not change during the study periods (Table 5). Discussion To our knowledge, this is the first population-based cohort study to assess the risk of HZ in adult populations with PUD. In this study, adults with PUD were found to be at greater risk for developing HZ than the control cohorts. Annual incidence of HZ in all PUD patients did not change during the study periods. Stratified analyses by risk factors of PUD revealed that PUD including any risk factors of PUD subgroups predisposed adult patients to HZ. PUD associated with the combination of nsNSAID usage and H. pylori infection put patients at the greatest risk of HZ in stratified analyses. 1878 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY Table 5 Numbers of herpes zoster patients and incidence for herpes zoster in all adult patients with peptic ulcer disease (PUD) during the follow-up period from 2002 to 2008 PUD patient numbers 6020 Herpes zoster numbers 475 Persons at risk 42 634 Incidence per 1000 person-years 11.14 2003 5089 384 30 960 12.40 2004 5999 353 30 888 11.43 2005 5611 298 23 071 12.92 2006 5798 217 19 067 11.38 2007 6559 177 15 578 11.36 2008 6153 109 8917 12.22 Calendar year 2002 HZ can cause acute pain and long-term morbidities, causing a negative impact on patients’ quality of life. Medical costs associated with HZ and zoster-related complications place a substantial burden on the healthcare system.1,3 An HZ vaccine for adults has been available since 2006. The present zoster vaccine guidelines, based primarily on age, recommend administering HZ vaccine to immunocompetent individuals aged 60 years or older. However, uptake rates of zoster vaccination are low.6,7 Much research concerning comorbidities has surveyed possible predictors of HZ in order to improve HZ vaccination strategies.8,25 PUD is an important health concern because of its high prevalence (4–17%) in adult populations worldwide.31–33 In this study, adult PUD patients were 1.77 times more likely to develop HZ than the general population. Our results suggest that PUD should be added to the list of risk factors for developing HZ. Furthermore, adult PUD patients were found more likely to suffer from the selected comorbidities and CCI scores greater than 1 than the control cohorts. Pre-specified subgroup analyses on exposure to the selected comorbidities showed that the adjusted HRs of HZ in PUD patients with none of the selected comorbidities was 1.94 (95% CI: 1.77–2.12) as compared with the controls (P < 0.001). The data indicate that PUD is associated with an increased risk for developing HZ after excluding the potential confounding effects of comorbidities. Furthermore, our findings in subgroup analyses concerning comorbidities are consistent with previous studies that have identified diabetes mellitus, cancers and hypertension25 as risk factors of HZ. Our results suggest that the benefits for HZ vaccination need to be evaluated in patients with PUD and other aforementioned comorbidities in future studies. Major risk factors of PUD are nsNSAID usage and/or H. pylori infection.11 Stratified analyses by the risk factors of PUD in PUD patients showed that the adjusted HRs for HZ in the two nsNSAID-related subgroups were higher than those in the other two subgroups including H. pylori infection only and Others. Although adjusted HRs of the fourth subgroup (Others) including usage of cyclooxygenase-2 inhibitors and other ulcerogenic medications increased the risk of HZ significantly, adjusted HRs of the fourth subgroup (Others) ranked the lowest among the four subgroups of PUD. The findings are consistent with previous studies showing that current exposures to NSAIDs, including nsNSAID and cyclooxygenase-2 inhibitors, increase the risk of HZ and zoster-related complications in human observational studies.10,34 However, our data revealed different influences on the risk of HZ between nsNSAID usage and cyclooxygenase-2 inhibitors/other ulcerogenic medications usage. The major morbidity caused by HZ is acute herpetic and chronic pain. NSAIDs, opioids, tricyclic antidepressants and gabapentin are capable of reducing herpetic pain. Prescribing NSAIDs for treating herpetic pain was common in a population-based study.4 Therefore, our data suggest that treating herpetic pain with NSAIDs, especially nsNSAIDs, should be avoided in PUD patients. First, immunity to varicella zoster virus may be decreased by nsNSAIDs exposure.6,10 Second, symptoms and signs of PUD may be worsened by exposure to nsNSAIDs because of their ulcerogenic properties. Based on our study and previous studies, HZ vaccination could be emphasized in PUD patients, especially those using nsNSAIDs. Several potential explanations can be made for the possible underlying mechanisms of the association between HZ and PUD. The risk of HZ is a comprehensive result of cellular immunity that has been linked to the ageing process2,21 and to nutritional status.21,22,35 PUD has been linked to immunological dysfunctions14,15 and nutritional deficiencies13,16,19,20 including proteins, vitamins A and C and zinc. Nutritional deficiencies13,20,36,37 may decrease specific immune responses to varicella zoster virus.38–40 As a consequence, PUD patients could be prone to developing HZ. In addition, nutritional deficiencies of vitamin C and zinc have been identified as predictors for HZ35,41–43 and postherpetic neuralgia (PHN).44,45 Thus, it is reasonable that our results suggest that PUD patients are associated with an increased risk of HZ through the possible common pathways of impaired cellular immunity and/or depressed nutritional status. PEPTIC ULCER DISEASE INCREASES ZOSTER INCIDENCE Strengths The main strength of our study is that our data were obtained from non-biased representative samples from a nationwide population-based database, in which up to 96% of Taiwan’s population was enrolled.9 An additional strength of our study is the relative homogeneity of Taiwan’s population, which reduces potential confounding by race, because racial differences may be a risk factor for developing HZ.46 Furthermore, patients with HZ received their diagnosis either in inpatient or outpatient clinics, which lessened the chance of selection bias arising from including only severely affected patients. Data on death were also obtained and calculated in this analysis. Thus, our data including person-years at risk and incidence per 1000 person-years were less biased than the results in previous studies.9 Limitations First, this study is based on a database. Cases of HZ were defined by diagnostic codes without medical record review.47 Second, H. pylori-associated PUD was defined as the usage of H. pylori eradication therapy in our study. It is impossible to identify those who did not receive H. pylori eradication therapy, in PUD patients and the control cohorts. Third, it is not possible for this study to clarify all of the causal relationships among PUD, HZ and other comorbidities. Fourth, our database did not include nutritional and immunological data of patients such as varicella voster virus (VZV)-specific T cell-mediated immunity. Nevertheless, the negative influence of PUD on the incidence of HZ is validated in the present study. Fifth, all patients in this study were Taiwanese and lived in a tropical region. Racial groups and geographical regions have been found to be independent factors in HZ and postherpetic neuralgia.48 It is possible that our results may not be applicable to the worldwide population. Thus, future large-scale investigations into other racial groups and geographical regions are needed to confirm the findings. In conclusion, to our knowledge, this populationbased cohort study is the first report to assess the risk of HZ in an adult population with PUD. In this 1879 study, PUD is found to be an independent risk factor for HZ. The PUD patients are more in need of vaccination than the general population, to lower incidence of HZ. Further studies are required to clarify the nature of the underlying associations between HZ and PUD.49 Supplementary Data Supplementary data are available at IJE online. Funding The present study was supported by grants (CMNDMC9712 and CMFHR10080) provided by the Chi Mei Medical Center, Tainan, Taiwan. Acknowledgements We appreciate the helpful remarks of Chung-Yi Li, Professor and Chairman of the Department of Public Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan. We appreciate the suggestion of the reviewer to increase the validity of the positive findings in this observational study by using falsification endpoints. These can be found in the supplemental file (available as Supplementary data at IJE online). Specific author contributions Drafting the manuscript: Jen-Yin Chen; performing statistical analysis: Shih-Feng Weng; all authors have been involved in critical study concepts and design, acquisition of data, revisions and editing of the manuscript and have approved the final draft; study supervision: Miao-Lin Hu. Jen-Yin Chen (the first author) will act as guarantor for the paper. Conflict of interest: None declared. KEY MESSAGES In this study, adult PUD patients were 1.77 times more likely to develop herpes zoster than the general population. This suggests that adult PUD patients are more in need of herpes zoster vaccination than the general population. Stratified analyses by the risk factors of PUD showed that any risk factors in the four subgroups of PUD predispose adult PUD patients to herpes zoster. Interestingly, adjusted HRs for herpes zoster in the two nsNSAID-related subgroups were higher than those in the other two subgroups including H. pylori infection only and Others. Our data indicate that the increased incidence of herpes zoster varied with the different risk factors of PUD. 1880 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY References 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 Yawn BP, Itzler RF, Wollan PC, Pellissier JM, Sy LS, Saddier P. Health care utilization and cost burden of herpes zoster in a community population. Mayo Clin Proc 2009;84:787–94. Oxman MN, Levin MJ, Johnson GR et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med 2005;352:2271–84. Yawn BP, Saddier P, Wollan PC, St Sauver JL, Kurland MJ, Sy LS. A population-based study of the incidence and complication rates of herpes zoster before zoster vaccine introduction. Mayo Clin Proc 2007;82: 1341–49. Jih JS, Chen YJ, Lin MW et al. Epidemiological features and costs of herpes zoster in Taiwan: a national study 2000 to 2006. Acta Derm Venereol 2009;89:612–16. Lin YH, Huang LM, Chang IS et al. Disease burden and epidemiology of herpes zoster in pre-vaccine Taiwan. Vaccine 2010;28:1217–20. Rimland D, Moanna A. Increasing incidence of herpes zoster among Veterans. Clin Infect Dis 2010;50:1000–05. Opstelten W, van Essen GA, Hak E. Determinants of noncompliance with herpes zoster vaccination in the community-dwelling elderly. Vaccine 2009;27:192–96. Joesoef RM, Harpaz R, Leung J, Bialek SR. Chronic medical conditions as risk factors for herpes zoster. Mayo Clin Proc 2012;87:961–67. Yang YW, Chen YH, Wang KH, Wang CY, Lin HW. Risk of herpes zoster among patients with chronic obstructive pulmonary disease: a population-based study. Cmaj 2011;183:E275–80. Mikaeloff Y, Kezouh A, Suissa S. Nonsteroidal antiinflammatory drug use and the risk of severe skin and soft tissue complications in patients with varicella or zoster disease. Br J Clin Pharmacol 2008;65:203–09. Ramakrishnan K, Salinas RC. Peptic ulcer disease. Am Fam Physician 2007;76:1005–12. Wu CY, Wu MS, Kuo KN, Wang CB, Chen YJ, Lin JT. Long-term peptic ulcer rebleeding risk estimation in patients undergoing haemodialysis: a 10-year nationwide cohort study. Gut 2011;60:1038–42. Salgueiro J, Zubillaga M, Goldman C et al. Review article: is there a link between micronutrient malnutrition and Helicobacter pylori infection? Aliment Pharmacol Ther 2004;20:1029–34. Gerhard M, Schmees C, Voland P et al. A secreted lowmolecular-weight protein from Helicobacter pylori induces cell-cycle arrest of T cells. Gastroenterology 2005; 128:1327–39. Satoh Y, Ogawara H, Kawamura O, Kusano M, Murakami H. Clinical Significance of Peripheral Blood T Lymphocyte Subsets in Helicobacter pylori-Infected Patients. Gastroenterol Res Pract 2012;2012:819–42. Malfertheiner P, Megraud F, O’Morain C et al. Current concepts in the management of Helicobacter pylori infection: the Maastricht III Consensus Report. Gut 2007;56: 772–81. Cho JY. Immunomodulatory effect of nonsteroidal antiinflammatory drugs (NSAIDs) at the clinically available doses. Arch Pharm Res 2007;30:64–74. Girndt M, Sester U, Kaul H, Hunger F, Kohler H. Glucocorticoids inhibit activation-dependent expression of costimulatory molecule B7-1 in human monocytes. Transplantation 1998;66:370–75. 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 Bjarnason I, Hayllar J, MacPherson AJ, Russell AS. Side effects of nonsteroidal anti-inflammatory drugs on the small and large intestine in humans. Gastroenterology 1993;104:1832–47. Nair S, Norkus EP, Hertan H, Pitchumoni CS. Micronutrient antioxidants in gastric mucosa and serum in patients with gastritis and gastric ulcer: does Helicobacter pylori infection affect the mucosal levels? J Clin Gastroenterol 2000;30:381–85. Lesourd B. Nutritional factors and immunological ageing. Proc Nutr Soc 2006;65:319–25. Maggini S, Wintergerst ES, Beveridge S, Hornig DH. Selected vitamins and trace elements support immune function by strengthening epithelial barriers and cellular and humoral immune responses. Br J Nutr 2007; 98(Suppl 1):S29–35. Hsiao FY, Tsai YW, Wen YW, Kuo KN, Tsai CR, Huang WF. Effect of Helicobacter pylori eradication therapy on risk of hospitalization for a major ulcer event. Pharmacotherapy 2011;31:239–47. Bureau of National Health Insurance in Taiwan. http:// www.nhi.gov.tw/english/index.aspx. Hata A, Kuniyoshi M, Ohkusa Y. Risk of Herpes zoster in patients with underlying diseases: a retrospective hospital-based cohort study. Infection 2011;39:537–44. Wang FW, Tu MS, Mar GY et al. Prevalence and risk factors of asymptomatic peptic ulcer disease in Taiwan. World J Gastroenterol 2011;17:1199–203. Wang YP, Liu CJ, Hu YW, Chen TJ, Lin YT, Fung CP. Risk of cancer among patients with herpes zoster infection: a population-based study. Cmaj 2012;184:E804–09. Kuo CC, Lee CT, Lee IM, Ho SC, Yang CY. Risk of herpes zoster in patients treated with long-term hemodialysis: a matched cohort study. Am J Kidney Dis 2012;59:428–33. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol 1992;45:613–19. Greenland S, Pearl J, Robins JM. Causal diagrams for epidemiologic research. Epidemiology 1999;10:37–48. Bernersen B, Johnsen R, Straume B, Burhol PG, Jenssen TG, Stakkevold PA. Towards a true prevalence of peptic ulcer: the Sorreisa gastrointestinal disorder study. Gut 1990;31:989–92. Aro P, Storskrubb T, Ronkainen J et al. Peptic ulcer disease in a general adult population: the Kalixanda study: a random population-based study. Am J Epidemiol 2006; 163:1025–34. Li Z, Zou D, Ma X et al. Epidemiology of peptic ulcer disease: endoscopic results of the systematic investigation of gastrointestinal disease in China. Am J Gastroenterol 2010;105:2570–77. Wolfe F, Michaud K, Chakravarty EF. Rates and predictors of herpes zoster in patients with rheumatoid arthritis and non-inflammatory musculoskeletal disorders. Rheumatology (Oxford) 2006;45:1370–75. Thomas SL, Wheeler JG, Hall AJ. Micronutrient intake and the risk of herpes zoster: a case-control study. Int J Epidemiol 2006;35:307–14. Milanino R, Frigo A, Bambara LM et al. Copper and zinc status in rheumatoid arthritis: studies of plasma, erythrocytes, and urine, and their relationship to disease activity markers and pharmacological treatment. Clin Exp Rheumatol 1993;11:271–81. Biondi C, Pavan B, Dalpiaz A, Medici S, Lunghi L, Vesce F. Expression and characterization of vitamin C PEPTIC ULCER DISEASE INCREASES ZOSTER INCIDENCE 38 39 40 41 42 43 transporter in the human trophoblast cell line HTR-8/ SVneo: effect of steroids, flavonoids and NSAIDs. Mol Hum Reprod 2007;13:77–83. Smith JG, Levin M, Vessey R et al. Measurement of cellmediated immunity with a Varicella-Zoster Virus-specific interferon-gamma ELISPOT assay: responses in an elderly population receiving a booster immunization. J Med Virol 2003;70(Suppl 1):S38–41. Kuvibidila SR, Gardner R, Velez M, Yu L. Iron deficiency, but not underfeeding reduces the secretion of interferongamma by mitogen-activated murine spleen cells. Cytokine 2010;52:230–37. Sandstead HH, Prasad AS, Penland JG et al. Zinc deficiency in Mexican American children: influence of zinc and other micronutrients on T cells, cytokines, and antiinflammatory plasma proteins. Am J Clin Nutr 2008;88:1067–73. High KP, Legault C, Sinclair JA, Cruz J, Hill K, Hurd DD. Low plasma concentrations of retinol and alpha-tocopherol in hematopoietic stem cell transplant recipients: the effect of mucositis and the risk of infection. Am J Clin Nutr 2002;76:1358–66. Schencking M, Vollbracht C, Weiss G et al. Intravenous vitamin C in the treatment of shingles: results of a multicenter prospective cohort study. Med Sci Monit 2012;18: CR215–24. Chen JY, Chang CY, Lin YS, Hu ML. Nutritional factors in herpes zoster, postherpetic neuralgia, 44 45 46 47 48 49 1881 and zoster vaccination. Popul Health Manag 2012;15: 391–97. Chen JY, Chang CY, Feng PH, Chu CC, So EC, Hu ML. Plasma vitamin C is lower in postherpetic neuralgia patients and administration of vitamin C reduces spontaneous pain but not brush-evoked pain. Clin J Pain 2009;25: 562–69. Chen JY, Chu CC, Lin YS, So EC, Shieh JP, Hu ML. Nutrient deficiencies as a risk factor in Taiwanese patients with postherpetic neuralgia. Br J Nutr 2011;106: 700–07. Schmader K, George LK, Burchett BM, Pieper CF, Hamilton JD. Racial differences in the occurrence of herpes zoster. J Infect Dis 1995;171:701–04. Yawn BP, Wollan P, St Sauver J. Comparing shingles incidence and complication rates from medical record review and administrative database estimates: how close are they? Am J Epidemiol 2011;174: 1054–61. Borkar DS, Tham VM, Esterberg E et al. Incidence of herpes zoster ophthalmicus: results from the pacific ocular inflammation study. Ophthalmology 2013;120: 451–56. Chen JY, Chang CY, Lan KM, Sheu MJ, Lu CL, Hu ML. Is peptic ulcer disease a risk factor of postherpetic neuralgia in patients with herpes zoster? Med Hypotheses 2013; doi: 10.1016/j.mehy.2013.09.007.