Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
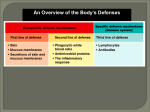
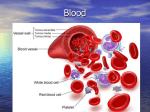
CLINICAL Fig 2. Eosinophil Fig 3. Basophil Fig 4. Monocyte SPL, Mediscan Fig 1. Neutrophil Part three – Granulocytes and monocytes Jonny Zygo Blood cells systems of life Macrophages engulfing Escherichia coli (left) and a microphage with an extended pseudopod, with which it engulfs micro-organisms and cellular debris author Ken Campbell, MSc Clinical Oncology, is clinical information officer, Leukaemia Research Fund (written in a private capacity). This article, the third in a series on blood cells, describes two types of white blood cells: granulocytes and monocytes. These along with lymphocytes, which will be discussed in the next article in this series, are responsible for the immune response. Myeloid lineage white blood cells As described in the first article in this series (Campbell, 2005), all blood cells can be defined as belonging to the lymphoid or myeloid lineage. Apart from lymphocytes and their precursors and derivatives, all white blood cells belong to the myeloid lineage. These myeloid lineage white cells are: l Granulocytes – which encompass neutrophils, eosinophils and basophils; l Monocytes – which migrate to tissues and transform into macrophages; l Dendritic cells – these are tissue cells that are not produced directly within the marrow, but are derived from marrow cells and are key components of the immune system. 26 Granulocytes Neutrophils Neutrophils (Fig 1) are the most numerous type of white blood cell, the normal neutrophil count is 2.5– 7.5 x 109 per litre of blood. Their lifespan in the circulation is about 6–12 hours. At any given time about two-thirds of the neutrophils in the circulation are attached to the walls of the blood vessels – these are known as the marginal pool, which allows a rapid rise in neutrophils in response to an infection or other stimulus. Once they enter the tissues, neutrophils last for 2–4 days. They cross the intact vascular endothelium by an active process called diapedesis. Neutrophils congregate at sites of tissue damage in a reaction called chemotaxis. They respond to signals released by bacteria, damaged white cells and dead or dying tissue cells. Neutrophils are phagocytes – their principal function is to ingest and destroy bacteria and other simple organisms. They are not active against intracellular organisms such as viruses, and are not potent enough to attack more complex organisms such as Mycobacterium tuberculosis. Neutrophils also ingest and break down cellular debris both from necrosis and from apoptotic cells NT 18 October 2005 Vol 101 No 42 www.nursingtimes.net keywords n Blood cells n Monocytes n Granulocytes (normal programmed cell death). Pus is a ‘soup’ of degraded neutrophils with bacteria and damaged cells that have been broken down by the neutrophils. Neutrophils are: l Increased in – bacterial infection, trauma, surgery, burns, haemorrhage, inflammation, infarction, polymalgia, myeloproliferative disorders and with some drugs; l Markedly increased in – leukaemia, disseminated malignancy and severe childhood infections; l Decreased in – viral infections, brucellosis, typhoid, kala-azar, tuberculosis, hypersplenism, bone marrow failure syndromes and also with some drugs, especially cancer chemotherapy. Eosinophils Eosinophils (Fig 2) are less numerous than neutrophils – the normal absolute eosinophil count is 0.04–0.44 x 109/L. They remain in the circulation for longer than neutrophils. The principal targets of eosinophils are persistent antigens on objects too large to be engulfed; whereas a neutrophil will ingest an invader, eosinophils attack using cytolytic enzymes. Eosinophils are enticed to enter the tissues by IgG and IgE antibodies and complement components bound to an invader, typically a multicellular parasite. Their numbers are classically very high in parasitic infestations and allergic responses. Persistent eosinophilia should always trigger a search for evidence of parasitic infection. Eosinophils are: l Increased in – conditions such as asthma and allergic disorders, parasitic infestations, skin disease, malignant disease, and during recovery from infection; l Decreased in – acute stress or infection and steroid therapy/Cushing’s syndrome. Basophils Basophils (Fig 3) are the least common, and probably the least understood type of granulocytes. A normal basophil count is 0.01–0.1 x 109/L. In a healthy blood film one typically sees very few or no basophils. The activity of basophils may facilitate access of lymphocytes and other cellular players in the inflammatory response to tissues. There is a reduction in circulating basophil numbers during flare-ups of chronic urticaria, which is thought to reflect active recruitment into weals (Grattan et al, 2003). There is evidence that basophils may have an immunoregulatory role in some situations (Galli, 2000). Basophils are: l Increased in – viral infections, urticaria, myxoedema, post-splenectomy ulcerative colitis, chronic myeloid leukaemia and other malignancies; l Decreased in – acute stress/infection, steroid therapy/Cushing’s syndrome and chronic urticaria (during flare-ups). NT 18 October 2005 Vol 101 No 42 www.nursingtimes.net Monocytes Monocytes (Fig 4), and their derivatives macrophages and dendritic cells, are antigen-presenting cells (APCs). Lymphocytes can only mount an effective response to an antigen when it is presented on the surface of an APC alongside appropriate costimulatory molecules. This mechanism reduces the risk of harmful autoimmune responses and allows tolerance for commensal organisms (Banchereau, 2002). As well as processing antigens, monocytes ingest and eliminate micro-organisms such as Mycobacterium tuberculosis, which have tough waxy cell coatings that neutrophils cannot break down. Despite their well-deserved reputation as the ‘heavies’ of the immune system, some organisms hide from the immune system within the macrophage population; these include certain mycobacteria, protozoa, Histoplasma capsulatum and HIV (Jandl, 1991). Normal monocyte count is about 0.2–0.8 x 109/L. They spend about 1.5 days in the circulation after leaving the marrow then move into the tissues as macrophages or dendritic cells, where they reside for months, or possibly years (Hoffbrand et al, 2001). Monocytes are: l Increased in – acute and chronic infections (such as tuberculosis, brucellosis, protozoa), malignant disease and myelodysplasia; l Decreased in – steroid therapy and hairy cell leukaemia. Macrophages and dendritic cells On leaving the circulation monocytes are transformed into either tissue macrophages or dendritic cells, both of which migrate through their host tissue ingesting and destroying micro-organisms and cellular debris and presenting antigens (self and non-self) to cells of the immune system. Tissue macrophages have many names because they were independently identified by early anatomists. Modern techniques reveal they belong to the same cell population. Tissue macrophage populations include the following: l Kidney – intraglomerular mesangial cells; l Liver – Kupffer cells; l Lung – alveolar macrophages; l Spleen – sinus macrophages; l Serosal membranes – serosal macrophages; l Bone marrow – bone marrow macrophages; l Lymph nodes – lymph node macrophages. In some cases, monocytes are transformed by developing cytoplasmic processes giving them a starlike appearance and are termed dendritic cells. These principally derive from myeloid or monocytic cells; but at least one type of lymphoid dendritic cell has been reported (Shortman and Caux, 1997). Whether dendritic cells of different origin have different functions is still being debated (Szabolcs et al, 2003). n References Banchereau, J. (2002) The long arm of the immune system: dendritic cells. Scientific American; 287: 5, 34–41. Campbell, K. (2005) Blood cells. Part one – Bone marrow. Nursing Times; 101: 40, 28–29. Galli, S.J. (2000) Mast cells and basophils. Current Opinion in Hematology; 7: 1, 32–39. Grattan, C.E.H. et al (2003) Blood basophil numbers in chronic ordinary urticaria and healthy controls: diurnal variation, influence of loratadine and prednisolone and relationship to disease activity. Clinical and Experimental Allergy; 33: 3, 337–341. Hoffbrand, A.V. et al (2001) The white cells 1: granulocytes, monocytes and their benign disorders. in: Hoffman, A.V. et al (eds) Essential Haematology; Oxford: Blackwell Science. Jandl, J.H. (1991) Monocytes, macrophages and the mononuclear phagocytic system. In: Jandl, J.H. (ed.) Blood: pathophysiology. Oxford: Blackwell Scientific. Shortman, K., Caux, C. (1997) Dendritic cell development: multiple pathways to nature’s adjuvants. Stem Cells; 15: 409–419. This article has been double-blind peer-reviewed. For related articles on this subject and links to relevant websites see www.nursingtimes.net 27