Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
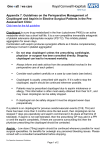
Clinical Investigation and Reports Effects of Aspirin Dose When Used Alone or in Combination With Clopidogrel in Patients With Acute Coronary Syndromes Observations From the Clopidogrel in Unstable angina to prevent Recurrent Events (CURE) Study Ron J.G. Peters, MD; Shamir R. Mehta, MD; Keith A.A. Fox, MD; Feng Zhao, MSc; Basil S. Lewis, MD; Steven L. Kopecky, MD; Rafael Diaz, MD; Patrick J. Commerford, MD; Vicent Valentin, MD; Salim Yusuf, DPhil; for the Clopidogrel in Unstable angina to prevent Recurrent Events (CURE) Trial Investigators Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Background—We studied the benefits and risks of adding clopidogrel to different doses of aspirin in the treatment of patients with acute coronary syndrome (ACS). Methods and Results—In the Clopidogrel in Unstable angina to prevent Recurrent Events (CURE) trial, 12 562 patients with ACS using aspirin, 75 to 325 mg daily, were randomized to clopidogrel or placebo for up to 1 year. In this analysis, patients were divided into the following 3 aspirin dose groups: ⱕ100 mg, 101 through 199 mg, and ⱖ200 mg. The combined incidence of cardiovascular death, myocardial infarction, or stroke was reduced by clopidogrel regardless of aspirin dose, as follows: ⱕ100 mg, 10.5% versus 8.6% (relative risk [RR], 0.81 [95% CI, 0.68 to 0.97]); 101 to 199 mg, 9.8% versus 9.5% (RR, 0.97 [95% CI 0.77 to 1.22]); and ⱖ200 mg, 13.6% versus 9.8% (RR, 0.71 [95% CI, 0.59 to 0.85]). The incidence of major bleeding increased with increasing aspirin dose both in the placebo group (1.9%, 2.8%, and 3.7%, respectively; P⫽0.0001) and the clopidogrel group (3.0%, 3.4%, and 4.9%, respectively; P⫽0.0009); thus, the excess risk with clopidogrel was 1.1%, 1.2%, and 1.2%, respectively. The adjusted hazard ratio for major bleeding for the highest versus the lowest dose of aspirin was 1.9 (95% CI 1.29 to 2.72) in the placebo group, 1.6 (95% CI 1.19 to 2.23) in the clopidogrel group, and 1.7 (95% CI 1.36 to 2.20) in the combined group. Conclusions—In patients with ACS, adding clopidogrel to aspirin is beneficial regardless of aspirin dose. Bleeding risks increase with increasing aspirin dose, with or without clopidogrel, without any increase in efficacy. Our findings suggest that the optimal daily dose of aspirin may be between 75 and 100 mg, with or without clopidogrel. (Circulation. 2003; 108:1682-1687.) Key Words: aspirin 䡲 coronary disease 䡲 angina 䡲 platelets 䡲 thrombosis A ntiplatelet therapy is effective in preventing serious vascular events both during short-term and long-term treatment in patients with atherosclerotic arterial disease.1 Aspirin is the most widely studied antiplatelet drug, with ⬎60 000 patients included in randomized trials against placebo. However, there is no uniformity in the doses used in clinical practice.2 Experimentally, a single oral 100-mg dose of aspirin is sufficient to completely block the synthesis of thromboxane A2 in healthy individuals, the predominant pathway by which aspirin inhibits platelet aggregation. Lower doses may require several days to reach complete blockade of thromboxane A2 production or fail to do so.3 At higher doses, the synthesis of prostacyclin is also inhibited, mainly in the endothelium. This could paradoxically lead to thrombosis and vasoconstriction. In addition, the incidence of other adverse effects increases, particularly the risk of gastrointestinal bleeding.3 Thus, careful selection of dose is important to balance efficacy against safety. Received November 22, 2002; de novo received March 6, 2003; revision received July 11, 2003; accepted July 11, 2003. From the Department of Cardiology (P.J.G.P.), Academic Medical Center, Amsterdam, the Netherlands; Canadian Cardiovascular Collaboration Project Office (S.R.M., F.Z., S.Y.), McMaster University, Hamilton, Ontario, Canada; Royal Infirmary of Edinburgh (K.A.A.F.), Edinburgh, UK; Lady Davis Carmel Medical Center (B.S.L.), Haifa, Israel; Division of Cardiovascular Diseases (S.L.K.), Mayo Clinic and Foundation, Rochester, Minn; Estudios Cardiologicos Latinoamerica (R.D.), Instituto Cardiovascular de Rosario, Argentina; Department of Medicine (P.J.C.), University of Cape Town, South Africa; and Unidad Coronaria (V.V.), Hospital Universitario Dr Peset, Valencia, Spain. All authors, except Dr Zhao, have received honoraria and travel expenses for speaking at scientific meetings from Sanofi-Synthelabo and Bristol Myers Squibb. All centers received a grant for the conduct of the CURE trial. Correspondence to Salim Yusuf, Canadian Cardiovascular Collaboration Project Office, Population Health Research Institute, McMaster University, Hamilton General Hospital, 237 Barton Street East, Hamilton, ON L8L 2X2, Canada. E-mail [email protected] © 2003 American Heart Association, Inc. Circulation is available at http://www.circulationaha.org DOI: 10.1161/01.CIR.0000091201.39590.CB 1682 Peters et al Compared with the original trials of aspirin in acute coronary syndrome (ACS), additional antithrombotic therapy (such as heparin) or invasive strategies are now commonly used. Furthermore, recent guidelines recommend the use of clopidogrel4 and glycoprotein (GP) IIb/IIIa receptor inhibitors. When all these drugs and interventions are used together, the risk of a major bleeding complications increases and optimal dosing of each drug, including aspirin, is even more important.5 Therefore, we performed an analysis of the Clopidogrel in Unstable angina to prevent Recurrent Events (CURE) study to explore the relationship between the dose of aspirin and risks of bleeding when used alone or in combination with clopidogrel in the context of current treatment strategies. Methods Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 The CURE study compared aspirin alone with aspirin plus clopidogrel in 12 562 patients with ACS without ST-segment elevation.6 Doses in the range of 75 to 325 mg daily were recommended by the study protocol. Almost all patients (99.8%) used aspirin. The dose of aspirin was chosen by the patient’s physician and in general was the same within a center. The design of the CURE study has been published previously7 and is summarized briefly. Patients Patients were eligible for inclusion if they had had symptoms indicative of ACS within the past 24 hours and if they did not have ST-segment elevation ⬎1 mm on their ECG. Other electrocardiographic evidence of new ischemia or concentrations of cardiac enzymes (including troponin) at least twice the upper limit of normal was required. Patients were excluded if they had New York Heart Association class IV heart failure, if they had undergone percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) in the previous 3 months, if they had contraindications to antithrombotic or antiplatelet therapy, if they had previous disabling or hemorrhagic stroke or intracranial hemorrhage, if they had clinically severe thrombocytopenia, if they used or required oral anticoagulants or nonstudy antiplatelet agents, or if they had received a GP IIb/IIIa inhibitor fewer than 3 days before randomization. Study Treatments Patients were randomly assigned clopidogrel or placebo. A loading dose of clopidogrel 300 mg orally or matching placebo was given immediately on a double-blind basis, followed by clopidogrel (75 mg per day) or matching placebo for 3 to 12 months. Aspirin was started or continued simultaneously with clopidogrel or placebo. The dose was left to the discretion of the local investigator; the study protocol recommended a dose of 75 to 325 mg. The dose and compliance with aspirin therapy was recorded on the case report forms and at each visit. Outcomes Efficacy The first coprimary outcome of the study was the composite of cardiovascular (CV) death, myocardial infarction (MI), or stroke. The second coprimary outcome was the composite of the first coprimary outcome or refractory ischemia. Detailed definitions of study outcomes have been previously published.6 Safety Major bleeding was defined as being significantly disabling, intraocular bleeding leading to significant loss of vision, or bleeding requiring transfusion of 2 or 3 units of red blood cells or equivalent whole blood. Major bleeding was subclassified as life-threatening or other major bleeding. Life-threatening bleeding complications were defined as fatal or leading to a drop in hemoglobin of ⱖ5 g/dL or significant hypotension with the need for inotropes, requiring sur- Aspirin Dose and Clopidogrel in Unstable Angina 1683 gery (other than vascular site repair) or symptomatic intracranial hemorrhage, or requiring transfusion of 4 or more units of red blood cells or equivalent whole blood. Minor bleeding was defined as any other bleeding requiring modification of the drug regimen. Analyses Patients were divided into the following 3 groups based on daily aspirin dose at the time of randomization: ⱕ100 mg, 101 through 199 mg, or ⱖ200 mg. An intention-to-treat analysis approach was used. The difference in proportions was tested by 2 test, and for the difference in means, the Student t test was used. The CochranArmitage trend test was used to test the trend in rates in aspirin dose groups. All hazard ratios (HRs) and 95% CIs for primary and secondary outcomes comparing the clopidogrel and placebo groups were derived by use of the Cox proportional hazards model. Efficacy HRs were adjusted for gender, weight, hypertension, components of the TIMI risk score, and rates of angiography, PCI, and CABG. For bleeding outcomes, a logistic regression model was used. HRs for bleeding events were adjusted for gender, weight, hypertension, components of the TIMI risk score, rates of angiography, PCI, and CABG, and the use of nonsteroidal anti-inflammatory drugs, heparin, GPIIb/IIIa inhibitors, oral anticoagulants, open-label ticlopidine, or clopidogrel at any time during the study period. In addition, a stratified analysis of the risk of bleeding at various doses of aspirin was performed in selected subgroups of patients. Tests for heterogeneity among various subgroups were also carried out. Results The main findings of the CURE study have been published previously.4 The first coprimary outcome of CV death, MI, or stroke occurred in 9.3% of the patients in the clopidogrel group and in 11.4% of the patients in the placebo group (relative risk [RR], 0.80; 95% CI, 0.72 to 0.90; P⬍0.001). The second coprimary outcome occurred in 16.5% of the patients in the clopidogrel group and 18.8% of the patients in the placebo group (RR, 0.86; 95% CI, 0.79 to 0.94; P⬍0.001). The overall risk of major bleeding was 3.7% in the clopidogrel group compared with 2.7% in the placebo group (RR 1.4; 95% CI, 1.1 to 1.7; P⫽0.001). Life-threatening bleeding occurred in 2.2% compared with 1.8%, respectively (RR 1.2; 95% CI, 1.0 to 1.6; P⫽0.13). The baseline characteristics of the patients in the 3 groups based on aspirin dose are presented in Table 1. There were 5320 patients receiving low-dose (ⱕ100 mg), 3109 receiving medium-dose (101 to 199 mg), and 4110 receiving high-dose (ⱖ200 mg) aspirin. Aspirin dosing varied among regions (Table 1). The use of the highest dose was most common in North and South America, the medium dose was common in Australia and New Zealand, and the lowest dose was common in Eastern and Western Europe. The median dose of aspirin used in the study was 150 mg. Within each center, the variation in aspirin dose was small; an average of 89% of all patients per center used a dose of aspirin within 50 mg of the most frequently used dose. Aspirin dose per patient varied little during the course of the study. Only 14% of patients used a dose that differed at least 50 mg from the initial dose for ⬎50% of the duration of follow-up. In general, the high-dose group included a greater proportion of men and patients with a prior history of diabetes, PCI, and CABG surgery. 1684 Circulation October 7, 2003 TABLE 1. Regional Distribution and Baseline Characteristics by Aspirin Dose Group Aspirin Dose ⱕ100 mg 101 to 199 mg ⱖ200 mg 5320 (42.4) 3109 (24.8) 4110 (32.8) Canada/United States, n (%) 232 (10.5) 78 (3.5) 1906 (86.0) Latin America, n (%) 187 (13.8) 144 (10.7) 1019 (75.5) Australia/New Zealand/South Africa, n (%) 209 (18.4) 832 (73.4) 93 (8.2) Western Europe, n (%) 3096 (61.6) 954 (19.0) 979 (19.5) Eastern Europe, n (%) 1596 (56.8) 1101 (39.2) 113 (4.0) Weight, kg, mean 77.3 77.3 78.2 Male, % 58.8 61.1 65.4 Body mass index, mean 27.3 27.4 27.6 Current smokers, % 20.8 24.2 25.1 Previous MI, % 32.0 31.1 33.2 Diabetes, % 21.0 19.8 26.8 Hypertension, % 58.8 56.6 60.5 History of PCI, % 9.2 7.1 12.8 10.0 8.9 13.8 3.3 3.1 3.5 N, % Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 History of CABG, % TIMI risk score, mean Additional Medication and Revascularization Procedures Table 2 presents the frequencies of the use of other antithrombotic medication and of revascularization procedures in the various aspirin dose groups. These additional treatments, except the use of nonsteroidal anti-inflammatory drugs and oral anticoagulants, were significantly more frequent in the highest aspirin dose group, reflecting practice patterns in the regions where higher doses are routinely used. Efficacy The impact of clopidogrel in preventing CV death, MI, or stroke was not significantly heterogeneous by aspirin dose (high-dose group, 9.8% versus 13.6%; RR, 0.71; 95% CI, 0.59 to 0.85; medium-dose group, 9.5% versus 9.8%; RR, 0.97; 95% CI, 0.77 to 1.22; low-dose group, 8.6% versus 10.5%; RR, 0.81; 95% CI, 0.68 to 0.97) (Figure 1). Similar results were observed with the composite of CV death, MI, stroke, and refractory ischemia (Figure 2). The results were not heterogeneous in patients receiving aspirin alone when examined by dose (highest and medium aspirin dose groups compared with the low-dose group: adjusted OR, 1.0 (95% CI, 0.82 to 1.23) and 1.2 (95% CI, 1.08 to 1.51), respectively (Table 3). In the aspirin plus clopidogrel group, event rates appeared to be similar across various doses (adjusted OR, 1.2 [95% CI, 0.98 to 1.48] and 1.2 [95% CI, 0.95 to 1.40] for medium- and high-dose groups compared with the low-dose group, respectively). Bleeding Clopidogrel increased the risk of bleeding at each dose of aspirin. However, the incidence of major bleeding complications increased significantly with increasing aspirin dose both TABLE 2. Additional Medications and Procedures During the Entire Study Period Aspirin Dose ⱕ100 mg N 5320 101 to 199 mg ⱖ200 mg 3109 4110 P Value Heparin, % 89.7 93.6 95.1 䡠䡠䡠 ⬍0.0001 NSAIDs, % 14.1 14.9 13.2 0.13 GP IIb/IIIa inhibitors, % 5.6 3.7 10.0 ⬍0.0001 Other antiplatelet agents* combined, % 19.0 17.5 25.4 ⬍0.0001 Oral anticoagulants, % 5.0 5.1 5.2 0.95 PCI, % 19.9 17.3 25.9 ⬍0.0001 CABG, % 15.6 16.5 17.7 0.02 *Open-label ticlopidine or clopidogrel. NSAIDs indicates nonsteroid anti-inflammatory drugs. Figure 1. Aspirin dose and incidence of first coprimary outcome (CV death, nonfatal MI, and stroke). Peters et al Aspirin Dose and Clopidogrel in Unstable Angina Figure 2. Aspirin dose and the incidence of the second coprimary outcome (CV death, nonfatal MI, stroke, and refractory angina). Figure 3. Aspirin dose and the incidence of major bleeding. Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 in the placebo (1.9%, 2.8%, 3.7%; P⫽0.0001) and the clopidogrel (3.0%, 3.4%, 4.9%; P⫽0.0009) groups (Figure 3). The risk of bleeding at the highest dose of aspirin given with placebo was higher than the risk of bleeding with the combination of clopidogrel and aspirin in the lowest-dose group (Figure 3). HRs for major bleeding for the 2 higherdose groups compared with the lowest-dose group are presented in Table 4. The risk of bleeding is lower at the lowest dose of aspirin. A similar pattern is observed in the subgroup of major bleeding complications defined as life-threatening (Table 4). Table 5 presents the results of a stratified analysis of the risk of major bleeding in selected subgroups of patients. In support of the multivariate analysis, a trend of a higher risk of bleeding with increasing doses of aspirin is observed consistently in patients undergoing PCI, CABG, or no revascularization. In patients who were not treated with heparin, no such trend is apparent. However, these numbers are small. In patients who were treated with GP IIb/IIIa inhibitors, no trend is observed. Again, the numbers are small and the use of these agents may increase the risk of bleeding to a rate where the impact of aspirin dose is masked. Regarding the site of bleeding, the rates of surgical, gastrointestinal, and puncture site bleeding increased significantly with increasing aspirin dose both in the placebo and the clopidogrel groups (data not shown). Minor bleeding compliTABLE 3. cations were not clearly related to aspirin dose (data not shown). Discussion Our study demonstrates 3 important observations. First, the benefits of clopidogrel, when added to aspirin, in reducing major ischemic events do not vary significantly by the aspirin dose used. Second, higher doses of aspirin are not associated with lower clinical event rates and may in fact be associated with higher event rates. Third, with increasing doses of aspirin, the risk of major bleeding increases, irrespective of whether it is used alone or in combination with clopidogrel. The ideal dose of aspirin for the prevention of vascular events has been the subject of much debate.3 This is best evaluated by comparing patients randomized to different doses; however, observational data may also be useful. Trials in patients with a cerebral transient ischemic attack have demonstrated increased bleeding complications with higher doses while observing no differences in efficacy.8,9 Other observations suggest that a low dose may be associated with a lower risk of vascular complications compared with higher doses.10,11 The latest report of the AntiThrombotic Triallists Collaboration (ATTC) identifies 10 trials that have directly compared 2 doses of aspirin across a variety of indications; 7 compared 500 to 1500 mg with 75 to 325 mg daily. Overall, there was no difference in the rates of vascular events (high- Incidence of the First Coprimary End Point by Various Doses of Aspirin Aspirin Alone ASA ⱕ100 mg ASA 101–199 mg ASA ⱖ200 mg P value for trend 1685 Aspirin⫹Clopidogrel All Patients HR Aspirin Plus Clopidogrel vs Aspirin Alone* 95% CI 10.5% 8.6% 9.6% 0.81 0.68–0.97 9.8% 9.5% 9.7% 0.97 0.77–1.22 13.6% 9.8% 11.7% 0.71 0.59–0.85 0.0016 0.17 0.0011 䡠䡠䡠 䡠䡠䡠 Adjusted† HR for 101 to 199 vs ⱕ100 1.0 (0.82–1.23) 1.2 (0.98–1.48) 1.09 (0.95–1.26) 䡠䡠䡠 䡠䡠䡠 Adjusted† HR for ⱖ200 vs ⱕ100 1.3 (1.08–1.52) 1.2 (0.95–1.40) 1.23 (1.08–1.39) 䡠䡠䡠 䡠䡠䡠 *Test for heterogeneity, P⫽NS. †Adjustment for gender, weight, hypertension, components of the TIMI risk score, and rates of angiography, PCI, and CABG. 1686 Circulation October 7, 2003 TABLE 4. Major and Life-Threatening Bleeding by Various Doses of Aspirin Aspirin Alone Aspirin⫹Clopidogrel All Patients Major bleeding complications ASA ⱕ100 mg, % 1.86 2.97 2.41 ASA 101–199 mg, % 2.82 3.41 3.12 ASA ⱖ200 mg, % 3.67 4.86 4.26 P value for trend ⬍0.0001 ⬍0.001 ⬍0.0001 Adjusted* OR for 101–199 vs ⱕ100 1.52 (1.00–2.31) 1.20 (0.84–1.73) 1.33 (1.01–1.74) Adjusted* OR for ⱖ200 vs ⱕ100 1.7 (1.22–2.59) 1.63 (1.19–2.23) 1.70 (1.33–2.16) ASA ⱕ100 mg, % 1.26 1.75 1.50 ASA 101–199 mg, % 1.90 1.39 1.64 ASA ⱖ200 mg, % 2.37 3.29 P value for trend 0.004 0.0006 Life-threatening bleeding complications 2.82 ⬍0.0001 Adjusted* OR for 101–199 vs ⱕ100 1.48 (0.89–2.46) 0.79 (0.47–1.32) 1.06 (0.74–1.52) Adjusted* OR for ⱖ200 vs ⱕ100 1.64 (1.04–2.59) 1.82 (1.22–2.71) 1.72 (1.27–2.32) Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 *Adjusted for gender, weight, hypertension, components of the TIMI risk score, rates of angiography, PCI and CABG, and the use of NSAIDs, heparin, GP2B3A inhibitors, oral anticoagulants, open-label ticlopidine, or clopidogrel at any time during the study period. versus low-dose RR, 1.03; SE⫽10, P⫽NS).1 Three trials compared doses ⬍75 mg daily with 75 mg or more daily. Again, there was no difference in event rates (high versus low RR, 0.92; SE⫽10).1 Taken together, these 10 trials demonstrated no significant difference in efficacy between different doses ranging from 75 to 1500 mg/d. Recently, a randomeffects model was used to analyze the same data. After adjustment for temporal trends, higher doses of aspirin were associated with less benefit.12 Indirect comparisons between the results of trials comparing different doses of aspirin versus placebo are also available. The ATTC report divided the trials into 4 subgroups based on daily aspirin dose, as follows: ⬍75, 75 to 150, 160 to 325, and ⬎500 mg, each compared with placebo. The odds reductions were 13%, 32%, 26%, and 19%, respectively. Thus, consistent with our findings, there is no evidence that the benefit of aspirin increases at dose ⬎75 mg/d. Furthermore, 4 studies have compared aspirin with placebo in patients with unstable angina using doses of 75,13 325,14 650,15 and 1300 mg.16 All studies showed a similar degree of risk reduction, consistent with our findings. In the pooled analysis by the ATTC in trials comparing aspirin with control, the proportional increase in the risk of a major extracranial bleed was similar with all daily aspirin doses ⬍325 mg. However, their analysis included smaller TABLE 5. patient numbers and patients at a lower overall risk of bleeding. Two trials that compared 75 to 325 mg aspirin daily with ⬍75 mg daily found a nonsignificant trend toward an increase in major extracranial bleeds at the higher dose of aspirin (39 of 1576 [2.5%] with 75 to 325 mg versus 28 of 1555 [1.8%] with ⬍75 mg). The mechanism underlying the differences in bleeding rates is not clear. Consistent with the literature,17 higher doses of aspirin were associated with higher rates of gastrointestinal bleeding, particularly in the placebo group, although the rates were low in the CURE study. This dose-response relationship may reflect at least 2 cyclo-oxygenase (COX)-1– dependent mechanisms, dose-dependent inhibition of COX-1 in the gastric mucosa and (relatively) dose-independent inhibition of COX-1 in platelets.18 Whereas platelet thromboxane synthesis is blocked completely at a daily dose of 100 mg, higher (or repeated) doses would be expected to inhibit COX-2– dependent thromboxane synthesis in vascular endothelium, monocytes, and macrophages. This could contribute to the impairment of hemostasis in patients using higher doses of aspirin. Despite the important benefits of clopidogrel in preventing major ischemic events in the CURE trial, there was an excess in (mostly reversible) major bleeding. However, our present analysis clearly demonstrates that the increase in bleeding Risk of Major Bleeding by Aspirin Dose in Various Patient Subgroups ⱕ100 mg, % (n) 101 to 199 mg, % (n) ⱖ200 mg, % (n) PCI alone 1.9 (997) 2.4 (508) 3.9 (1000) 11.1 (728) P Value for Trend 0.0068 CABG 6.9 (829) 7.6 (514) No revascularization 1.5 (3494) 2.2 (2087) 2.3 (2382) 0.0030 0.019 Heparin 2.6 (4774) 3.2 (2909) 4.4 (3910) ⬍0.0001 No heparin 0.9 (546) 2.0 (200) 1.5 (200) 0.39 GP IIb/IIIa 5.4 (298) 1.7 (115) 5.1 (410) 0.96 No GP IIb/IIIa 2.2 (5022) 3.2 (2994) 4.2 (3700) ⬍0.0001 Peters et al Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 was largely dependent on the dose of aspirin used. By lowering the dose of aspirin, the risk of major bleeding may be substantially attenuated without loss of efficacy. Indeed, the major bleeding rates for combined use of low-dose aspirin plus clopidogrel are lower than for using aspirin alone at higher doses. Similarly, the risk of surgical bleeding with the combination of aspirin and clopidogrel seems also to be dependent on the dose of aspirin used. Consequently, surgical bleeding risks may also be reduced by using lower aspirin doses than presently used in several regions of the world, including North and South America. Balancing risk and benefit is particularly important when patients are at increased risk of bleeding, based on the presence of multiple risk factors such as age, weight, and female sex.18,19 Furthermore, combinations of antithrombotic medications are used in high-risk patients, which are likely to increase the risk of bleeding (clopidogrel, heparin, aspirin, and GP IIb/IIIA inhibitors). In addition, the risk of bleeding increases additionally when interventions, especially coronary bypass surgery, are performed in the presence of these drugs. Therefore, approaches to maintaining the benefits of the various treatments while reducing the risk of bleeding would be useful. Because the use of clopidogrel in patients with unstable coronary syndromes is now recommended (class IA recommendation in the United States guidelines), it is important that clinicians consider the dose of aspirin that is to be used in ACS. Based on our findings and on the observations in the ATTC, a dose between 75 and 100 mg may be optimal, either alone or in combination with clopidogrel. Limitations Our findings are based on a post hoc observational analysis and should be considered exploratory. The dose of aspirin was not prescribed by the study protocol, nor was it randomized. However, the data with respect to both efficacy and bleeding are internally consistent in both the placebo and the clopidogrel groups and externally consistent with data from the ATTC meta-analysis. Second, the main determinant of the dose used in patients in CURE was the routine approach of centers and specific countries (Table 1). This argues against the possibility that the selection of dose may be related to the risk profile of patients, thus confounding the differences in efficacy or safety between dose groups. Third, regional differences in patient populations and practice patterns are reflected by significant differences in the baseline characteristics of the patients (Table 1) and in additional treatments. However, after adjustment for these differences, including the use of other antithrombotics, a dose response between aspirin and bleeding complications is still observed. Conclusions Our findings demonstrate that clopidogrel, when added to aspirin and other standard therapies, is beneficial in patients with ACS irrespective of the dose of aspirin used. Compared with a daily dose of 75 to 100 mg with or without concomitant use of clopidogrel, higher doses of aspirin lead to higher Aspirin Dose and Clopidogrel in Unstable Angina 1687 rates of bleeding complications without increasing efficacy. The available data suggest that in patients treated for unstable coronary syndromes, a daily dose of aspirin in the range of 75 to 100 mg may be optimal. Acknowledgments The CURE study was funded by Sanofi-Synthelabo and Bristol Meyers Squibb. However, the study was conducted independently under the supervision of the CURE Steering Committee and coordinated by the Population Health Research Institute at McMaster University and Hamilton Health Sciences. Dr Yusuf is a Senior Scientist of the Canadian Institutes of Health Research and holds a Heart and Stroke Foundation of Ontario Research Chair. References 1. Antithrombotic Triallists Collaboration. BMJ. 2002;324:71– 86. 2. Patrono C, Coller B, Dalen JE, et al. Platelet-active drugs: the relationships among dose, effectiveness, and side effects. Chest. 2001;119: 39S– 63S. 3. Awtry EH, Loscalzo J. Aspirin. Circulation. 2000;101:1206 –1218. 4. Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA Guideline Update for the Management of Patients With Unstable Angina and Non–ST-Segment Elevation Myocardial Infarction, 2002: Summary Article. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Unstable Angina). Circulation. 2002;106: 1893–1900. 5. Gilchrist IC, Berkowitz SD, Thompson TD, et al. Heparin dosing and outcome in acute coronary syndromes: the GUSTO-IIb experience. Am Heart J. 2002;144:73– 80. 6. The Clopidogrel in Unstable Angina to Prevent Recurrent Events Trial Investigators. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345:494 –502. 7. CURE study investigators. The Clopidogrel in Unstable Angina to Prevent Recurrent Events (CURE) Trial programme: rationale, design and baseline characteristics including a meta-analysis of the effects of thyenopyridines in vascular disease. Eur Heart J. 2000;21:2033–2041. 8. UK-TIA Study Group. United Kingdom Transient Ischaemic Attack (UK-TIA) aspirin trial: interim results. BMJ. 1988;296:316 –320. 9. The Dutch TIA Trial Study Group. A comparison of two doses of aspirin (30 mg vs 283 mg a day) in patients after a transient ischemic attack or minor stroke. N Engl J Med. 1991;325:1261–1266. 10. Taylor DW, Barnett HJM, Haynes RB, et al. Low-dose and high-dose acetylsalicylic acid for patients undergoing carotid endarterectomy: a randomised controlled trial. Lancet. 1999;353:2179 –2184. 11. van Gijn J. Low doses of aspirin in stroke prevention. Lancet. 1999;353: 2172–2173. 12. Kong DF, Hasselblad V, Kandzari DE, et al. Seeking the optimal aspirin dose in acute coronary syndromes. Am J Cardiol. 2002;90:622– 625. 13. The RISC Group. Risk of myocardial infarction and death during treatment with low dose aspirin and intravenous heparin in men with unstable coronary artery disease. Lancet. 1990;336, 827– 830. 14. Lewis HD, Davis JW, Archibald DG, et al. Protective effects of aspirin against acute myocardial infarction and death in men with unstable angina: results of a Veterans Administration cooperative study. N Engl J Med. 1983;309:396 – 403. 15. Theroux P, Ouimet H, McCans J, et al. Aspirin, heparin, or both to treat acute unstable angina. N Engl J Med. 1988;319:1105–1111. 16. Cairns JA, Gent M, Singer J, et al. Aspirin, sulfinpyrazone, or both in unstable angina. N Engl J Med. 1985;313:1369 –1375. 17. Roderick PJ, Wilkes HC, Meade TW. The gastrointestinal toxicity of aspirin: an overview of randomized controlled trials. Br J Clin Pharmacol. 1993;35:219 –226. 18. Blankenship JC. Bleeding complication of glycoprotein IIb-IIIa receptor inhibitors. Am Heart J. 1999;138:S87–S296. 19. Aguirre FV, Topol EJ, Ferguson JJ, et al for the EPIC investigators. Bleeding complications with the chimeric antibody to platelet glycoprotein IIb/IIIa integrin in patients undergoing percutaneous coronary intervention. Circulation. 1995;91:2882–2890. Effects of Aspirin Dose When Used Alone or in Combination With Clopidogrel in Patients With Acute Coronary Syndromes: Observations From the Clopidogrel in Unstable angina to prevent Recurrent Events (CURE) Study Ron J.G. Peters, Shamir R. Mehta, Keith A.A. Fox, Feng Zhao, Basil S. Lewis, Steven L. Kopecky, Rafael Diaz, Patrick J. Commerford, Vicent Valentin and Salim Yusuf for the Clopidogrel in Unstable angina to prevent Recurrent Events (CURE) Trial Investigators Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Circulation. 2003;108:1682-1687; originally published online September 22, 2003; doi: 10.1161/01.CIR.0000091201.39590.CB Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2003 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/108/14/1682 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/