Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Academy of Nutrition and Dietetics wikipedia , lookup
Abdominal obesity wikipedia , lookup
Obesity and the environment wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Diet-induced obesity model wikipedia , lookup
Food choice wikipedia , lookup
Human nutrition wikipedia , lookup
Obesity in the Middle East and North Africa wikipedia , lookup
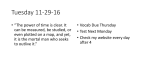
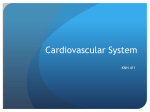
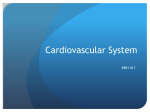
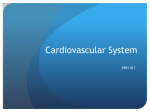
European Journal of Clinical Nutrition (2002) 56, 992–1003 ß 2002 Nature Publishing Group All rights reserved 0954–3007/02 $25.00 www.nature.com/ejcn ORIGINAL COMMUNICATION The nutrition transition in Spain: a European Mediterranean country LA Moreno1, A Sarrı́a2 and BM Popkin3* 1 EU Ciencias de la Salud, Universidad de Zaragoza, Zaragoza, Spain; 2Departamento de Pediatrı́a, Universidad de Zaragoza, Zaragoza, Spain; and 3Carolina Population Center, University of North Carolina, Chapel Hill, North Carolina, USA Background: Mediterranean diets are felt to be healthful diets linked with reduced mortality from diet-related noncommunicable diseases. Objective: To examine trends in diet, activity, obesity and diet-related noncommunicable diseases for Spain and compare these with other European countries, particularly those from the Mediterranean area. Design: A combination of large-scale primary and secondary nationally representative data analysis are used. Data: Nationally representative data on household food consumption, physical activity, adult obesity, and cause of death are combined with regionally representative adolescent obesity data, obtained in the last four decades. Comparative diet and obesity data come from nationally representative comparable data, obtained during the same period. Results: The Spanish diet has shifted toward a very high level of fat intake, high fruit and dairy intake and moderate vegetable intake. Dairy and fruit intakes were the highest in Europe, as was the proportion of energy from fat, when we compared with the available data. Adult overweight and obesity trends show a marked increase in the past decade to levels as high as Italy and far above France. Overweight for children aged 6 – 7 is above that of even the USA, while adolescent overweight levels are among the highest in the world. Cardiovascular disease mortality is low, as with Italy and France, and the cancer mortality rate is lower than Italy and France. Conclusions: We have observed that, in Spain, relatively high obesity prevalences and dairy intake levels are related to much lower levels of cardiovascular disease and cancer mortality than are found in other European countries. This unique Spanish dietary and obesity pattern should be further explored in order to clarify the causal links. Support: The National Institutes of Health (NIH; R01-HD30880 and R01-HD38700). European Journal of Clinical Nutrition (2002) 56, 992 – 1003. doi:10.1038/sj.ejcn.1601414 Keywords: Spain; nutrition transition; the Spanish paradox; obesity; physical activity Introduction The epidemiological transition, particularly the rapid shift in morbidity and mortality patterns towards much higher noncommunicable disease rates, has dominated the health profile of an increasingly large number of people in higher income countries for the last half-century or more. Concurrent shifts in diet, activity and body composition also appear *Correspondence: BM Popkin, Department of Nutrition, Carolina Population Center, University of North Carolina, CB no. 8120 University Square, 123 W Franklin St, Chapel Hill, NC 27516-3997, USA. E-mail: [email protected] Guarantor: BM Popkin. Received 19 July 2001; revised 4 January 2002; accepted 8 January 2002 to be accelerating in many regions of the world (Popkin, 1998). This analysis provides an understanding of the multidimensional phenomenon of the nutrition transition, a sequence of characteristic dietary and nutritional patterns resulting from large shifts in the overall structure of diet, related to changing economic, social, demographic and health factors in Spain, a country that modernized later than most European countries. While Spain was not as deeply affected as other parts of Mediterranean Europe by World War II, it was affected by its own civil war in the period 1936 – 1939 and a subsequent period of isolation with minimal economic development (the 40 y of the Franco era). During this period, Spain suffered an international embargo. After 1975, Spain underwent a rapid transition toward a democratic system, joined the European Union, and has experienced rapid economic change. Nutrition transition in Spain LA Moreno et al 993 This papers builds on previous studies of the dietary and epidemiological changes among the Spanish population and focuses on some unique nutritional issues, including the much higher level of fat intake in the diet, higher obesity levels, along with related socioeconomic and other health factors (Serra-Majem et al, 1993a, 1995; Moreno et al, 2000b). It focuses on the nutrition transition experienced in Spain, a special European Mediterranean country, during the last 30 – 40 y and points out some important distinguishing features. The main purpose of this paper is to explore obesity and dietary intake levels and its relationship with low levels of cardiovascular diseases and cancer mortality found in Spain. Methods A range of primary and secondary economic, dietary intake, physical activity, anthropometric, cause of death and mortality rate data from published reports and articles is used. Economic data Data on urbanization trends were obtained from the Food and Agriculture Organization (FAO) and data on work force structure from the International Labor Office (ILO). For economic trends, we used national income data from the official estimates of gross national product (GNP) per capita (Atlas method) from 1960 to 1998 as established by the World Bank (The International Bank for Reconstruction and Development). GNP per capita was expressed in 1995 US dollars adjusted for inflation on the basis of consumer price indices (Bureau of Labor Statistics), to allow for an easier comparison across the years. Dietary data A series of comparable nationally representative household budget surveys was used to provide a picture of the nutrition transition in Spain. Household dietary information in Spain was obtained from three household budget surveys conducted by the National Institute of Statistics in 1964 – 1965, 1980 – 1981 and the latest in 1990 – 1991 (INE, 1995). While these surveys focus on economic issues, they utilize a systematic sampling and data collection system to collect food consumption and expenditure data which can be used to understand shifts in the structure of food intake in the country. The samples consist of 20 800 – 28 000 households and data collection took place with a record system over a full week. Food consumption in Spain in 1990 – 1991 has been compared with food consumption data obtained in nationally representative household budget surveys, that have been included in the DAFNE (Data Food Networking) databank (Naska et al, 2000). We have also compared these data with those obtained in national dietary surveys conducted in Italy (Turrini et al, 1999) and France (Volatier & Verger, 1999). Energy and macronutrient intakes assessed in the Spanish household budget surveys have been compared with energy and macronutrient intakes assessed in some European national surveys (Becker, 1999; Flynn & Kearney, 1999; Haraldsdottir, 1999; Hermann-Kunz & Thamm, 1999; Ministry of Agriculture Fisheries and Food, 1991; Turrini et al, 1999; Valsta, 1999; Volatier & Verger, 1999). Physical activity data Physical activity data were obtained from the National Health Surveys (Encuesta Nacional de Salud de España 1997, 1999). These surveys started in 1987, but information on physical activity patterns was only obtained in the 1993, 1995 and 1997 surveys. The survey sampled the whole country, but included only the non-institutionalized population. The study sample of those surveys was selected by a multi-stage stratified sampling scheme, and included 26 100 individuals in 1993, 8400 in 1995 and 8400 in 1997. Information on physical activity patterns in the adult population described occupational activity and leisure-time activity. We present leisure-time physical activity data, obtained in the three surveys by the same question: ‘Please, could you tell me what of the following possibilities better describe the majority of your activities during your leisure-time?’ Individuals had four options: (1) I do not perform any exercise, my leisure-time is sedentary; (2) some physical activity or sport performed occasionally; (3) regular physical activity, several times per month; (4) physical training several times per week. Anthropometric data At present, there are no data on anthropometric measurements or the prevalence of obesity in a representative sample of the child or adult Spanish population. We have obtained data on body mass index (BMI) for children aged 6 – 7 y and adolescents aged 13 – 14 y, from the Aragón School Health Examination Surveys, carried out from 1985 to 1995, Aragón being a representative region of the whole country, in terms of socio-economic and health indicators. These surveys began near the start of the school year and lasted 6 – 9 months. Of the 109 916 children aged 6 – 7 y of age (56 741 males and 53 175 females), 90 997 (45 970 males and 45 027 females) were examined in the nine cross-sectional surveys conducted between 1985 and 1995 (this represented 82.79% of the school population in the first school year). Of the 147 251 students (75 478 males and 71 773 females) 13 – 14 y of age, 106 284 (52 772 males and 53 512 females) were also examined in the nine cross-sectional surveys conducted (this represented 72.18% of the school population in the last school year; Moreno et al, 2000a). We chose to use the ‘International Obesity Task Force (IOTF) reference’, since it is appropriate for international use. First, it is developed based on data from multiple nations including Brazil, Britain, Hong Kong, The European Journal of Clinical Nutrition Nutrition transition in Spain LA Moreno et al 994 Netherlands, Singapore, and the US (Cole et al, 2000). Second, the BMI cut-offs are linked to adult cut-offs for overweight and obesity, which are good indicators of risks for adverse health outcomes. They are derived from sexspecific curves that pass through a BMI of 25 and 30 by age 18 for overweight and obesity, respectively. We have compared overweight prevalences in Aragón with those obtained in other countries: Russia, US, Brazil, China, England and Scotland (Chin & Rona, 2001). For adults we use secondary analysis of national surveys from Spain, Italy, France and Germany. In all the cases, to assess BMI values, they use reported height and weight. a major reduction in energy expenditure at work (Popkin, 1998). Cause-of-death data We present cause-of-death trends as percentages of total deaths for four disease categories (Instituto Nacional de Estadı́stica). The four categories chosen to illustrate major shifts in disease patterns were: (1) infectious and parasitic diseases (including tuberculosis); (2) diseases of the respiratory system (eg pneumonia and bronchitis); (3) malignant neoplasms (eg cancers of the stomach, liver, bronchus and lung); and (4) diseases of the circulatory system (eg, rheumatic heart disease, hypertensive disease, ischemic heart disease, cerebrovascular disease and diseases of the pulmonary circulation). All European countries submit annual mortality data to WHO. For the present study, cause-specific mortality rates by year for European Mediterranean countries were obtained from WHO, Geneva (WHO Regional Office for Europe). The starting year of 1970 was chosen aiming to cover the 8th, 9th and 10th revision of the International Classification of Diseases (ICD). No major changes in the classification of the disease groups of interest occurred during the transition from the 8th to the 10th revision of the ICD. Food consumption changes The total amount of food intake per capita per day, calculated from household food intake, fluctuated around 1700 g between 1964 – 1965 and 1990 – 1991 (Table 1). A shift did occur in the sources of food. The percentage of plant-food intake decreased consistently, from 76.1% in 1964 – 1965 to 57.3% in 1990 – 1991. In contrast, the percentage of animal food intake increased almost two-fold from 23.9 to 42.7% of per capita daily grams of food intake. This shift can be clearly seen by examining the intake trends for each food group. Consumption of cereals and grain products decreased to half of its 1964 – 1965 level. In 1964 – 1965, per capita intake of cereals accounted for 24% of total grams of food intake; however, cereals accounted for only 11% of total intake in 1990 – 1991. Other starchy staples, including both legumes and potatoes, were also reduced to half their 1964 – 1965 consumption levels. The intake of vegetables increased slightly between 1964 – 1965 and 1990 – 1991. The major positive shift was a very large increase in fruit consumption from 164.8 to 326.7 g per capita per day in that period. There were also reductions in consumption of vegetable-based oils and fats, added sugar, and wine. Intake of all animal food products increased significantly from 1964 – 1965 to 1990 – 1991. Meat and poultry consumption increased three-fold in that period. Consumption of fish and milk food groups also increased from 1964 – 1965 to 1990 – 1991. While the rate of increase for milk and dairy products did not match that for meat, the absolute increase for these food products represents the dominant element in Results Table 1 Spanish economy Remarkable changes have occurred in the Spanish economy and the structure of its workforce over the past 30 – 40 y. GNP per capita increased dramatically from the early 1960s to the 1990s. The GNP increased in real (deflated) terms approximately four-fold between 1960 and 1997, from 4423 1996 US dollars in 1960 to 14 799 in 1997. With this rapid shift in income, associated changes in the population and occupation distributions occurred. In 1950, the Spanish population was approximately half urban and this increased to 76% urban by 1995. The proportion of the workforce in energyintensive occupations such as the rural primary-product sectors of agriculture, forestry and fisheries has halved during the 1977 – 1993 period, while service sector occupations have increased to over 54% of the workforce and manufacturing has held steady at about 38% of the workforce. The current occupational structure of Spain is similar to that of most Western countries. This transition is linked to European Journal of Clinical Nutrition Changes in intake by food groups, 1964 – 1965 to 1990 – 1991 1964 – 1965 1980 – 1981 1990 – 1991 Plant foods (g=capita=day) Cereals and grain products Legumes and their products Potatoes and starches Vegetables Fruits Vegetable oils and fats Sugar Wine Total Animal foods (g=capita=day) Meat, poultry and their products Eggs Fish and shellfish Milk and dairy products Animal oils and fats Total Total (g=capita=day) Percentage of animal food (%) 402 41 292 156 165 62 39 131 1289 236 26 202 163 272 70 36 114 1120 194 23 138 165 327 56 25 69 995 73 33 62 224 14 407 1695 24 169 38 72 380 3 662 1782 37 229 28 88 396 3 743 1739 43 Nutrition transition in Spain LA Moreno et al 995 the animal food component of the diet. Egg intake increased until 1980 – 1981 and decreased thereafter. Consumption of animal oils and fat fell considerably during this same period. Intake trends for major food groups between 1964 – 1965 and 1990 – 1991 are shown in Figure 1. The figure illustrates a dramatic fall in total cereal intake with a significant rise in Figure 1 Shifts in food consumption of key food groups in Spain, 1964 – 1991. Figure 2 A comparison of food consumption patterns in Spain and other European countries. European Journal of Clinical Nutrition Nutrition transition in Spain LA Moreno et al 996 fruit intake. As noted above, the intake of meat and milk food groups also increased considerably from 1964 – 1965 to 1990 – 1991. The unique features of food intake in Spain are its very high fruit, milk and milk product intake along with a relatively low vegetable intake. We combine several sets of data to compare fruit and vegetable intake across Europe. This comparative analysis explicitly excluded potatoes from the vegetable category. In Figure 2 we see that the fruit intake of Spain is greater than any other country in Western Europe, for example France. Vegetable intake is also high in Spain but below that for Greece. The other unique element of the Spanish diet is the very high milk and dairy intake. Surprisingly, intake of milk and milk products in Spain is even above that for Denmark. No country in Western Europe reports a higher level of dairy consumption than Spain. Nutrients Total energy intake decreased gradually from 1964 – 1965 to 1990 – 1991 (Table 2). Total energy intake was as high as 12.59 MJ (3008 kcal) per capita per day in 1964 – 1965 but, despite the trends to more sedentary activities, total energy intake remained 11.02 MJ (2634 kcal) per capita per day in 1990 – 1991. In terms of individual nutrients, carbohydrates showed the same pattern as did total energy intake. The change in the proportion of energy derived from each nutrient is presented in the first three panels of Figure 3. The decline in the proportion of energy from carbohydrates (from 53 to 42% of energy intake) and the small increase in protein intake (from 12 to 14% of energy intake) are seen. Equally important is the dramatic increase in the proportion of energy from fat. This level was 32% in 1964 – 1965, increased to 40% by 1980 – 1981, and has increased slightly since then to 41.5% in 1990 – 1991. In the 1990 – 1991 period, saturated fat represent 11.9%, monounsaturated fat 18.8% and polyunsaturated fat 6.8% of total energy intake. These are very high levels of fat intake and reasonably high levels of saturated fat intake. The high level of total fat intake is offset in many ways by the very large proportion of monounsaturated fat and the high mono-plus polyunsaturated fat to saturated fat ratio. In Table 2 Changes in macronutrient and energy intakes, 1964 – 1965 to 1990 – 1991 Carbohydrate (g) Fat (g) Protein (g) Alcohol (g) Energy (MJ) (kcal) European Journal of Clinical Nutrition 1964 – 1965 1980 – 1981 1990 – 1991 423 108 87 15 333 131 98 16 294 121 94 10 12.6 3008 12.2 2914 11.0 2634 1964, monounsaturated fat represented 53% of the total fat intake and by 1991, due to a larger increase in other fats in the diet, it was still 45% of total fat. The ratio of (mono þ poly)=saturated fat was 2.34 in 1964 and 2.15 in 1991. Recent surveys of children in Spain from Galicia, Madrid and Zaragoza found about 44 – 45% of total fat from monounsaturated sources, but a much higher saturated fat intake and ratios of (mono þ poly)=saturated fat that varied from 1.39 to 2.25 (unpublished results). In this same figure we compare the macronutrient intake pattern of Spain with that from other European countries (Becker, 1999; Flynn & Kearney, 1999; Haraldsdottir, 1999; Hermann-Kunz & Thamm, 1999; Ministry of Agriculture Fisheries and Food, 1991; Turrini et al, 1999; Valsta, 1999; Volatier & Verger, 1999; De Henauw & De Backer, 1999; Graca, 1999). Comparing the proportion of energy from carbohydrates, often viewed as one element of the traditional Mediterranean diet, Spanish households consume 42% of their energy from carbohydrates compared with only 38% in France and 48 – 49% in Italy and Portugal. In contrast, at the other end of the spectrum, Spain’s 42% of energy from fat is the highest level of consumption of energy from fat in Europe, matched only by England in 1990. Italy and Portugal consume only 29 – 33% of their energy from fat although the Portuguese data are from a much earlier period (1984). Physical activity data Physical activity data shows that more than 45% of the Spanish population is completely sedentary during their leisure-time (Figure 4). However, the proportion of individuals that were completely sedentary during their leisuretime has decreased from 55 to 46% in the 1993 – 1997 period. The proportion of people that made some physical activity per week in their leisure-time increased from 4 to 7% in that period. Obesity For the entire country there is good national data on adult obesity trends and similar data for older children and adolescents is available only for the Aragón region. Using surveys representing large representative samples from each country, we see that adult obesity has risen in Spain and is at levels comparable or even higher than Italy or France (Figure 5). These levels are below those reported for Germany and other European countries (Gutierrez-Fisac et al, 2000; Hoffmeister et al, 1994; Maillard et al, 1999; Pagano et al, 1997). The increase in a decade in Spain from 27% of males to 34.8% and from 22% of females to 25.6% is pronounced for males but not females. These rates of increase in Spain exceed those for Italy. Over a third of Spanish adult males and a quarter of women were obese or overweight in the 1995 – 1997 Nutrition transition in Spain LA Moreno et al 997 survey. The obesity levels are higher than those found in Italy and France but below those of Germany. In the school-age population of Aragón (Spain), BMI has increased in all the age and sex groups studied (16.28 – Figure 3 The proportion of energy from macronutrients: a comparison of European countries. Figure 4 Shifts in leisure-time activities in Spain, 1993 – 1997. European Journal of Clinical Nutrition Nutrition transition in Spain LA Moreno et al 998 Figure 5 A comparison of obesity patterns and trends in Spain with other European countries. 16.96 kg=m2 in males aged 6 y, 16.42 – 17.17 kg=m2 in males aged 7 y, 16.32 – 16.91 kg=m2 in females aged 6 y, and 16.56 – 17.17 kg=m2 in females aged 7 y). The patterns and trends for child and adolescent overweight prevalence are equally significant (Figures 6a and b). By 1995 – 1996, in Aragón over a third of boys and girls aged 6 – 7 were overweight. The levels are somewhat lower for adolescents aged 13 – 14; however, there is a noted increase over the 1985 – 1996 period in adolescent overweight. In Figure 7a and b we utilize the International Obesity Task Force’s (IOTF) proposed standards for overweight (equivalent to a BMI of 25 or greater) discussed earlier. It is important to note that the IOTF standards are based on both several higher-income countries (the US, The Netherlands and England) and a number of middle income ones (Singapore, Brazil, Hong Kong). These results are compared with data for the same age group for Russia, the US, Brazil and China and aged 7 – 8 and 9 – 11 for England and Scotland. For children aged 6 – 7, the Spanish prevalence of overweight ( > 33%) is far greater than that found for any other country. In fact, the increase measured by prevalence points over a 10 y period is greater in Spain than the total found in China, England and Scotland. The rates of increase among adolescents are equally large in Aragón; however, in comparative terms the US has a far higher level of adolescent overweight and Scottish and English adolescents have only slightly lower overweight prevalence levels. European Journal of Clinical Nutrition Spain has a very high ratio of overweight prevalence among older children (34% in males and 36% in females in 1995 – 1996) compared with adolescents (21% in both sexes in 1995 – 1996). Only in the US, England and Scotland are there such marked higher prevalences among teenagers but in Spain, Brazil, and China it is the opposite — adolescent overweight prevalence is higher. Causes of death Diseases of the circulatory system have been the leading cause of death in Spain since 1980. Cancer is the second leading cause of death. After 1980, the proportion of deaths by diseases of the circulatory system has begun to decrease, representing 45.83% of all deaths in Spain in 1979 and 37.58% of all deaths in 1997, while those related to cancer have increased (Figure 7). This shift from cardiovascular to cancer mortality is seen throughout Europe; however, cardiovascular diseases (CVD)-related mortality rates are still higher in all countries. Age-standardized mortality rates from diseases of the circulatory system in European Mediterranean countries are shown in Figure 8. From 1970 to the late 1990s, we can observe a decrease in mortality from diseases of the circulatory system in all the countries, except Greece (despite a decrease after 1987, mortality rates were higher in 1997 than in 1970). The increase in Greece’s CVD mortality is important to note. The decline is relatively Nutrition transition in Spain LA Moreno et al 999 Figure 6 (a) A comparison of children aged 6 – 7: obesity patterns and trends in Aragón, Spain with other countries. Note: data for England and Scotland is for 7 – 8-y-olds. (b) A comparison of adolescent (aged 13 – 14): obesity patterns and trends in Aragón, Spain with other countries. Note: data for England and Scotland is for 9 – 11-y-olds. Source: Chin and Rona, 2001. larger in Spain (from 435=100 000 in 1970 to 239=100 000 in 1996), placing Spain second lowest to France in this mortality rate category. Age-standardized mortality rates from cancer in European Mediterranean countries are shown in Figure 9. In 1996, agestandardized mortality rates from cancer in these countries ranged from 163 to 192=100 000. The countries with the lowest mortality rates from cancer in 1970 (Greece, Portugal and Spain) have tended to increase their mortality rates. In contrast, mortality rates in countries with high rates in 1970 (France and Italy) were relatively unchanged in the late 1990’s from those in the 1970s. European Journal of Clinical Nutrition Nutrition transition in Spain LA Moreno et al 1000 Figure 7 Trends in the causes of death in Spain, 1980 – 1997. Figure 8 Comparison of mortality from cardiovascular diseases, 1970 – 1998. European Journal of Clinical Nutrition Nutrition transition in Spain LA Moreno et al 1001 Figure 9 Comparison of mortality from cancer, 1970 – 1998. Discussion The nutrition transition in the last decades has been described in different developing countries (Popkin, 1998; Kim et al, 2000; Monteiro et al, 1995; Romieu et al, 1997; Vio & Albala, 2000). In this paper, we analyzed the nutrition transition in an industrialized country of the European Mediterranean region. The case of Spain is different from other European countries, due to different political conditions. During this century, Spain has experienced important socioeconomic and consequently food behavior modifications; from the post-war period, without radical changes (1940 – 1960), to a period of expansion and development (1961 – 1975; Serra-Majem et al, 1993a, b). From an economic point of view, Spain has experienced a rapid transition when compared with northern European countries, but a slow transition when compared with lower-income countries. For example, South Korea has increased its GNP 17 times in 34 y (Kim et al, 2000) and Spain has increased it four times in 37 y. Dietary and epidemiologic changes among the Spanish population in the last decades have been previously analyzed (Serra-Majem et al, 1993a,b; Moreno et al, 2000b). What is unique about this paper is the full exploration of not only diet and obesity but also related economic and physical activity and mortality patterns and a comparison with other related countries. From this paper we get a full picture of Spain and its relative position and unique characteristics. For the food intake analysis, we utilize the household food consumption surveys that exist for many European countries but are rarely examined (Trichopoulou, 1992). The data are nationally representative and reliable. Their actual levels most likely overstate nutrient and food intake levels as they do not allow for wastage during the processing and consumption stages. Moreover, these surveys report dietary intake data per capita only; and per capita intakes do not reflect household members’ intakes equally. These limitations prevented us from adjusting on the fact that the Spanish population has aged. That means that we underemphasized trends related to decreased intake and overemphasized trends related to increased intake. There is a possibility reported elsewhere in Europe that higher fat foods and total fat in general are undermeasured more in the 1990s than earlier; however there is no literature on the measurement of other food components (Heitmann et al, 2000; Lafay et al, 1998). The dietary trends found that a very high level of energy from fat, increased meat and especially dairy intake, very high fruit intake, and quite low vegetable intake, define the Spanish diet. The dairy and fruit intake undoubtedly are among the highest found in Europe, far above other Mediterranean countries. Similarly, the high proportion of monounsaturated fat and the high ratio of monounsaturated plus polyunsaturated fat to saturated fat provides an important dimension to the Spanish diet. European Journal of Clinical Nutrition Nutrition transition in Spain LA Moreno et al 1002 On average, in the European Union, nearly three-quarters of the population participate in some kind of physical activity (Vaz de Almeida et al, 1999). In general, the highest proportions of participants were found in the Nordic countries and the lowest in the southern ones. Despite the fact that data on obesity in adults have been obtained from self-reports that lead to underestimation of the true prevalence, adult obesity is very high, as is adult overweight status (34.8% overweight and obesity in males and 25.6% in females; Gutierrez-Fisac et al, 2000). Trends show marked increases in adult male obesity in the past decade or two. The overweight levels for children aged 6 – 7 from the Aragón region of Spain are much higher than in many other countries and adolescent obesity levels are high moreover, it has been observed that the increase in BMI is parallel to an increase in the percentage of body fat assessed by anthropometry (Moreno et al, 2001a) and also parallel to trends towards a central pattern of fat distribution (Moreno et al, 2001b). The overweight problem may relate partly to the energy density of the diet (Bray & Popkin, 1998), but it equally could result from the other component of energy balance, physical activity and inactivity. It has been pointed out that increasing prevalence of obesity may be mostly attributed to reduction of physical activity (Vioque et al, 2000; Martı́nezGonzález et al, 1999). One key component of inactivity is television viewing, which has been associated with obesity in Spanish adults and adolescents (Vioque et al, 2000; Moreno et al, 1998). Moreover, the concepts ‘Controling weight’ and ‘Being fit’ are not perceived to be as important in Spain as elsewhere in the European Union (Holgado et al, 2000). The most noticeable feature of the Spanish nutrition transition is the decrease in mortality from diseases of the circulatory system, parallel to an increase in dietary fat intake and an increase of fruit intake, but we must take into account that mortality data may reflect either a change in the incidence of the disease or a change in medical care that improves survival, lowering the case-fatality rate. The increasing trend in fat consumption is due primarily to a sharp increase in consumption of meat and dairy products. According to the well known relation between dietary fat, serum cholesterol and cardiovascular diseases (Ascherio et al, 1996), a significant increase in incidence and mortality from diseases of the circulatory system should have been detected in Spain. The unexpected trends observed have been termed the ‘Spanish paradox’ (Serra-Majem et al, 1995). This paradox most likely stems from the interaction of multiple synergistic and antagonistic risk and protective factors for CVD. Of much current interest is the role of antioxidants and phytochemicals that may be the keys to understanding the paradoxical trends on mortality from diseases of the circulatory system in Spain as well as in France, Italy and Portugal. The pattern of fruit consumption in Spain reflects a 4.1% annual increase during 1964 – 1980 and 2.0% during 1981 – 1991, which resulted in a net increase of 162 g fruit per capita per day during a 25 y period. There is a puzzling element to this European Journal of Clinical Nutrition ‘Spanish paradox’, namely that the other Mediterranean country with high fruit intake and high total fruit and vegetable intake is Greece. Yet the CVD mortality for Greece is rising while that for Spain is declining. Also it is important to note the high proportion of monounsaturated fat in the diet. Concerning the observed trends on the mortality from cancer, Serra-Majem et al (1993a) analyzed trends in consumption of fat and fat-containing foods in relation to trends in mortality for ovarian, breast, colorectal and prostate cancer in certain European countries and suggested that trends of increased fat consumption appeared to antedate trends of increased rates of ovarian and colorectal cancer, and to a lesser extent, breast cancer. Other authors have also reviewed relations between diet and cancer in Spain (Benito & Cabeza, 1993). Given the low mortality rates from the main causes of death in Spain, identifying the characteristics of the Spanish diet would help us to better understand how to promote a healthier diet. Additional research is needed to explore the full set of determinants of the Spanish dietary pattern and the subsequent health consequences in terms of diet-related chronic diseases. Acknowledgements The study was supported in part by grants from the National Institutes of Health (NIH; R01-HD30880 and R01-HD38700). We are grateful to Samara Nielsen, in particular, and also Youfa Wang for research assistance. We also thank Ms Frances Dancy for her administrative assistance and Mr Tom Swasey for assistance with the graphics. References Ascherio A, Rimm EB, Giovannucci EL, Spiegelman D, Stampfer M & Willet WC (1996): Dietary fat and risk of coronary heart disease in men: cohort follow up study in the United States. Br. Med. J. 313, 84 – 90. Becker W (1999): Dietary guidelines and patterns of food and nutrient intake in Sweden. Br. J. Nutr. 81,(Suppl 2) S113 – S117. Benito E & Cabeza E (1993): Diet and cancer risk: an overview of Spanish studies. Eur. J. Cancer Prev. 2, 215 – 219. Bray GA & Popkin BM (1998): Dietary fat intake does affect obesity! Am. J. Clin. Nutr. 68, 1157 – 1173. Bureau of Labor Statistics, US Department of Labor: www.stats.bls.gov/blshome/datahome/top20.html (accessed 1 September 2000). Chin S & Rona RJ (2001): Prevalence and trends in overweight and obesity in three cross sectional studies of British children, 1974 – 94. Br. Med. J. 322, 24 – 26. Cole TJ, Bellizzi MC, Flegal KM & Dietz WH (2000): Establishing a standard definition for child overweight and obesity worldwide: international survey. Br. Med. J. 320, 1240 – 1243. DAFNE. Data food networking. Databank a tool for monitoring trends in food habits in Europe http:==nut.noa.gr=english (accessed 30 November 2001) De Henauw S & De Backer G (1999): Nutrient and food intakes in selected subgroups of Belgian adults. Br. J. Nutr. 81,(Suppl 2) S37 – S42. Encuesta Nacional de Salud de España 1997 (Spanish National Health Survey 1997) (1999): Madrid: Ministerio de Sanidad y, Consumo. Nutrition transition in Spain LA Moreno et al Flynn MA & Kearney JM (1999): An approach to the development of food-based dietary guidelines for Ireland. Br. J. Nutr. 81,(Suppl 2) S77 – S82. Food and Agriculture Organization: www.apps.fao.org (accessed 1 September 2000). Graca P (1999): Dietary guidelines and food nutrient intakes in Portugal. Br. J. Nutr. 81,(Suppl 2) S99 – S103. Gutierrez-Fisac JL, Banegas JR, Rodriguez F & Regidor E (2000): Increasing prevalence of overweight and obesity among Spanish adults, 1987 – 1997. Int. J. Obes. Relat. Metab. Disord. 24, 1677 – 1682. Haraldsdottir J (1999): Dietary guidelines and patterns of intake in Denmark. Br. J. Nutr. 81,(Suppl 2) S43 – S48. Heitmann BL, Lissner L & Osler M. (2000) Do we eat less fat, or just report so? Int. J. Obes. Relat. Metab. Disord. 24, 435 – 442. Hermann-Kunz E & Thamm M (1999): Dietary recommendations and prevailing food and nutrient intakes in Germany. Br. J. Nutr. 81(Suppl 2), S61 – S69. Hoffmeister H, Mensink GB & Stolzenberg H (1994): National trends in risk factors for cardiovascular disease in Germany. Prev. Med. 23, 197 – 205. Holgado B, de Irala-Estévez J, Martı́nez-González MA, Gibney M, Kearney J & Martı́nez JA (2000): Barriers and benefits of a healthy diet in Spain: comparison with other European member states. Eur. J. Clin. Nutr. 54, 453 – 459. INE (1995): Encuesta de presupuestos familiares 1990 – 91. Estudio nacional de nutrición y alimentación (Household budget survey 1990 – 91. National study of nutrition and diet). Madrid: Instituto Nacional de Estadı́stica. Instituto Nacional de Estadı́stica. Tempus Banco de Datos. Estadı́sticas de causas de muerte (Cause of death statistics): www.ine.es (accessed 1 September 2000). International Labor Office. Foreign Labor Statistics: www.stats.bls.gov (accessed 1 September 2000). Kim S, Moon S & Popkin BM (2000): The nutrition transition in South Korea. Am. J. Clin. Nutr. 71, 44 – 53. Lafay L, Basdevant A, Charles M-A, Vray M, Balkau B, Borys J-M, Eschwège E & Romon M (1998) Determinants and nature of dietary underreporting in a free-living population: the Fleurbaix Laventie Ville Santé (FLVS) study. Int. J. Obes. Relat. Metab. Disord. 46, 567 – 573. Maillard G, Charles MA, Thibult N, Forhan A, Sermet C, Basdevant A & Eschwege E (1999): Trends in the prevalence of obesity in the French adult population between 1980 and 1991. Int. J. Obes. Relat. Metab. Disord. 23, 389 – 394. Martı́nez-González MA, Martı́nez JA, Hu FB, Gibney MJ & Kearney J (1999): Physical activity, sedentary lifestyle and obesity in the European Union. Int. J. Obes. Relat. Metab. Disord. 23, 1192 – 1201. Ministry of Agriculture Fisheries and Food (1991): Household Food Consumption and Expenditure 1990. Annual Report of the National Food Survey Committee. Monteiro CA, Mondini L, Medeiros de Souza AL & Popkin BM (1995) The nutrition transition in Brazil. Eur. J. Clin. Nutr. 49, 105 – 113. Moreno LA, Fleta J & Mur L (1998) Television watching and fatness in children. JAMA 280, 1230 – 1231. Moreno LA, Sarrı́a A, Fleta J, Rodrı́guez G & Bueno M (2000a) Trends in body mass index and overweight prevalence among children and adolescents in the region of Aragón (Spain) from 1985 to 1995. Int. J. Obes. Relat. Metab. Disord. 24, 925 – 931. Moreno LA, Sarría A, Lázaro A & Bueno M (2000b): Dietary fat intake and body mass index in Spanish children. Am. J. Clin. Nutr. 72,(Suppl) 1399S – 1403S. Moreno LA, Fleta J, Sarrı́a A, Rodrı́guez G & Bueno M (2001a): Secular increases in body fat percentage in male children of Zaragoza (Spain), 1980 – 1995. Prev. Med. 33, 357 – 363. Moreno LA, Fleta J, Sarrı́a A, Rodrı́guez G, Gil CM & Bueno M (2001b): Secular changes in body fat patterning in children and adolescents of Zaragoza (Spain), 1980 – 1995. Int. J. Obes. Relat. Metab. Disord. 25, 1656 – 1660. Naska A, Vasdekis VG, Trichopoulou A, Friel S, Leonhauser IU, Moreiras O, Nelson M, Remaut AM, Schmitt A, Sekula W, Trygg KU & Zajkas G (2000): Fruit and vegetable availability among ten European countries: how does it compare with the ‘five-a-day’ recommendation? DAFNE I and II projects of the European Commission. Br. J. Nutr. 84, 549 – 556. Pagano R, La Vecchia C, Decarli A, Negri E & Franceschi S (1997): Trends in overweight and obesity among Italian adults, 1983 through 1994. [Letter]. Am. J. Publ. Health 87, 1869 – 1870. Popkin BM (1998): The nutrition transition and its health implications in lower income countries. Publ. Health Nutr. 1, 5 – 21. Romieu I, Hernandez-Avila M, Rivera JA, Ruel MT & Parra S (1997): Dietary studies in countries experiencing a health transition: Mexico and Central America. Am. J. Clin. Nutr. 65,(Suppl) 1159S – 1165S. Serra-Majem L, La Vecchia C, Ribas L et al (1993a): Changes in diet and mortality from selected cancers in southern Mediterranean countries, 1960 – 1989. Eur. J. Clin. Nutr. 47,(Suppl 1) S25 – S34. Serra-Majem L, Ribas L, Lloveras G & Salleras L (1993b): Changing patterns of fat consumption in Spain. Eur. J. Clin. Nutr. 47,(Suppl 1) S13 – S20. Serra-Majem L, Ribas L, Treserras R, Ngo J & Salleras L (1995): How could changes in diet explain changes in coronary heart disease mortality in Spain? The Spanish paradox. Am. J. Clin. Nutr. 61,(Suppl) 1351S – 1359S. The International Bank for Reconstruction and Development (2000): World development indicators 2000. Washington, DC: World Bank (CD-ROM). Trichopoulou A (1992): Monitoring food intake in Europe: a food data bank based on household budget surveys. Eur. J. Clin. Nutr. 46,(Suppl 5) S3 – S8. Turrini A, Leclercq C & D’Amicis A (1999): Patterns of food and nutrient intakes in Italy and their application to the development of food-based dietary guidelines. Br. J. Nutr. 81,(Suppl 2) S83 – S89. Valsta LM (1999): Food-based dietary guidelines for Finland — a staged approach. Br. J. Nutr. 81,(Suppl 2) S49 – S55. Vaz de Almeida MD, Graca P, Afonso C, D’Amicis A, Lappalainen R & Damkjaer S (1999): Physical activity levels and body weight in a nationally representative sample in the European Union. Publ. Health Nutr. 2, 105 – 113. Vio F & Albala C (2000): Nutrition policy in the Chilean transition. Publ. Health Nutr. 3, 49 – 55. Vioque J, Torres A & Quiles J (2000): Time spent watching television, sleep duration and obesity in adults living in Valencia, Spain. Int. J. Obes. Relat. Metab. Disord. 24, 1683 – 1688. Volatier JL & Verger P (1999): Recent national French food and nutrient intake data. Br. J. Nutr. 81,(Suppl 2) S57 – S59. WHO Regional Office for Europe. Health for all data base: www.who.dk (accessed 1 September 2000). 1003 European Journal of Clinical Nutrition