Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
International Journal of Obesity (2003) 27, 693–700
& 2003 Nature Publishing Group All rights reserved 0307-0565/03 $25.00
www.nature.com/ijo
PAPER
TM
Short-term effects of sibutramine (Reductil ) on
appetite and eating behaviour and the long-term
therapeutic outcome
B Barkeling1*, K Elfhag1, P Rooth1,{ and S Rössner1
1
Obesity Unit, Institute of Internal Medicine, Huddinge University Hospital, Stockholm, Sweden
OBJECTIVE: To evaluate the short-term effects of sibutramine on appetite and eating behaviour and whether these effects are
related to the long-term therapeutic outcome.
STUDY DESIGN: Short-term: randomised, double-blind, placebo-controlled, within-subject design. Long-term: prospective
open clinical trial.
SUBJECTS: A total of 36 obese (nine men/27women) with a body mass index of 39.374.3 (mean7s.d.) (range 30.2 – 45.2) kg/
m2 and age 44.4712.1 y.
PROCEDURE AND METHODS: First phaseFshort-term effects: At baseline, the subjects were treated for 14 days with 15 mg
sibutramine/placebo (period 1) followed by a 2 weeks single-blind placebo washout period, the subjects received the alternative
therapy for another 14 days (period 2). At baseline, and at day 14 in each treatment period the subjects arrived fasting to the
laboratory for a standardised breakfast and an ad libitum standardised lunch using the VIKTOR set-up (a universal eating
monitor) to evaluate the microstructure of the eating behaviour (ie amount of food consumed and eating rate). Visual Analogue
Scales were applied before and after the meals as well as every hour between the meals to monitor the appetite. During this first
phase, subjects were encouraged to keep their habitual eating habits. Second phaseFlong-term effects: All subjects received 10
months open treatment with 15 mg sibutramine and dietary advice in monthly group sessions with a dietitian. On the last day of
this treatment period, the subjects returned to repeat the measurements of appetite and eating behaviour using the same test
procedure as during the first phase of the study.
RESULTS: First phase: Sibutramine influenced appetite and eating behaviour that could be registered after only 14 days of
treatment. The amount of food consumed at lunch on VIKTOR was reduced by 16% by sibutramine compared to placebo,
3357123 g vs 3997126 g (Po0.0001). Second phase: Responders and nonresponders were defined as those who ate less vs
more food on VIKTOR when treated with sibutramine compared to the baseline food intake in the first phase of the study. The
weight reduction was greater for responders 11.876.2 (mean7s.d.) kg compared to nonresponders 6.872.7 (mean7s.d.) kg
(Po0.05).
CONCLUSION: Short-term effects of sibutramine on appetite and eating behaviour were identified such as a reduction in food
intake and in ratings of subjective motivation to eat. Short-term sibutramine effects on eating behaviour are to some extent
related to the long-term therapeutic outcome in obese subjects.
International Journal of Obesity (2003) 27, 693–700. doi:10.1038/sj.ijo.0802298
Keywords: appetite; eating behaviour; sibutramine; universal eating monitor
Introduction
Obesity has become a major health problem worldwide.1 An
important task is to prevent this obesity epidemic, and also
*Correspondence: Dr B Barkeling, Obesity Unit M73, Huddinge University
Hospital, SE-141 86 Stockholm, Sweden.
E-mail: [email protected]
{
Deceased.
Received 4 July 2002; revised 16 January 2003;
accepted 28 January 2003
to find efficient long-term treatment programmes for the
already obese.
The development of obesity is determined by genetic,
biological, environmental, social, psychological and ethnical
factors, but the relative contribution and importance of each
such factor varies greatly among individuals. The obese are
not a homogenous group and therefore there is no single
ideal treatment programme available. A range of different
treatment approaches exist: from behavioural modification
and cognitive therapy to surgical therapy and different
pharmacological approaches.
Short-term effects of sibutramine
B Barkeling et al
694
One recent addition to the treatment arsenal is sibutramine, a serotonin and noradrenaline reuptake inhibitor
(SNRI). Sibutramine exerts its weight-reducing effects mainly
by reducing the appetite, but also to some extent by
increasing thermogenesis.2 The long-term weight reducing
effect of sibutramine is well established,3 and the drug is also
effective in sustaining weight maintenance after weight loss.3
In order to offer each patient optimal treatment a common
clinical experience is that there is an urgent need to find
predictors for successful treatment outcome.4
If sibutramine’s appetite-reducing effects are measurable
already after a short term, these appetite measurements
could further be tested in relation to the long-term therapy
outcome. Thus, the aim of the first phase of the study was to
evaluate the short-term effects of sibutramine on appetite,
using objective as well as subjective measurements. The
primary aim of the second part of the study was to evaluate
the relation between the appetite measurements and the
long-term weight reduction.
Subjects and methods
A randomised, double-blind, placebo-controlled, crossover
design was conducted in the first phase of the trial. The
second phase of the trial was open and all subjects received
active medication (15 mg sibutramine) for 10 months.
Male and female patients from 20 to 65 y with a body mass
index (BMI) between 30 and 45 kg/m2 were recruited from
the waiting list to the outpatient Obesity unit at the
Huddinge University Hospital after informed consent had
been obtained. The main exclusion criteria were endocrine
causes of obesity, cardiovascular disorders including hypertension and/or arrythmia, treatment with drugs that might
interfere with the sibutramine action or other conditions
where sibutramine treatment is contraindicated according to
the general clinical routines (eg betablockers and SSRIs).
Participation was stopped if patients became pregnant,
presented with concomitant severe disease, suffered severe
adverse events, withdrew their informed consent or failed
to attend the clinical appointments during the first phase of
the study.
A total of 38 subjects were initially included in the study.
Two subjects were withdrawn from the study within 2 weeks
from study start: one woman because of pregnancy, and
one woman because she failed to attend on the first test
days. Thus, 36 subjects (nine males/27 females) aged
44.1712.1 (mean7s.d.) y with BMI 39.374.3 kg/m2 (range
39.2 – 45.2) were eligible for the evaluation of the first phase
of the study.
All 36 subjects entered the second phase of the study and
27 (20 women/seven men) of them completed the full 10
months period. One patient was excluded because of
hypertension. The remaining eight dropped out because
of the following subjective reasons given: two subjects
because of dry mouth, one because of insomnia and the
other five because of administrative reasons (eg lack of
International Journal of Obesity
time to participate at the monthly group sessions) and/or
insufficient therapeutic response (eg subjects considered
their weight loss progress to be less than they had expected).
Study medication
Sibutramine (15 mg) and placebo were supplied in identical
opaque white capsules in coded bottles. Subjects were
instructed to take their daily dose of medication in the
morning by swallowing the whole capsule with water
before breakfast.
Measurements of appetite and eating behaviour
The main effect variable in this study was the single-meal
intake of food (measured by VIKTOR), which was regarded as
an objective measurement of the effect of appetite of
sibutramine. The VIKTOR equipment consists of a hidden
scale built into a table and connected to a computer. A
plate with a homogenous meal in excess is placed on top
of the scale and the subjects are instructed to eat until
satisfied. After the meal is finished the computer calculates
the microstructure of the eating behaviour, that is the total
food intake in grams, meal duration in minutes and
eating rate as grams per minute. The stability of these eating
variables has been tested previously and over five eating
occasions both relative (test–retest) and absolute (F-test)
stability has been found in both obese and normal weight
men and women.5,6 The intraindividual coefficient of
variation (CV) calculated on the same population (76
subjects) is 14% for the variable food intake and 14% for
eating rate.
The eating curve is also fitted to a polynomial. Twice the
quadratic coefficient represents the rate of deceleration.7 A
negative coefficient illustrates a decelerating eating curve, an
eating curve where the eating rate slows down towards the
end of the meal. The decelerating eating curve is the most
common type of eating curve and has also been called the
biological satiating curve.8 A positive coefficient represents
an accelerating eating curve.
Assessments of subjective feelings of appetite that is desire
to eat, hunger, satiety and how much they could eat
(prospective consumption) were made by Visual Analogue
Scales (VAS).6,9 For example, the question ‘How strong is
your desire to eat now?’ was rated along a 100 mm scale
anchored with ‘Not strong at all’ on the left and ‘Very, very
strong’ on the right.
Meals
The standardised breakfast, which had to be entirely
consumed by the subjects, consisted of two slices of wholemeal bread (90 g), low-fat margarine (10 g), cheese 28% fat
(30 g), a glass of orange juice (200 g) and a cup of coffee or
tea. The breakfast energy content was 1837 kJ (protein 16.9 g
(16 E%), fat 15 g (30 E%), carbohydrate 58.5 g (54 E%)). The
Short-term effects of sibutramine
B Barkeling et al
695
ad libitum lunch meal served was an industrially produced
Swedish hash with a standard energy content of 650 kJ/100 g
(protein 6 g (15 E%), fat 8 g (45 E%), carbohydrate 16 g
(40 E%)) consisting of diced meat, onions and potatoes
mixed and fried, which is a common Swedish lunch dish.
Procedure
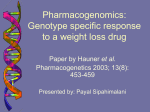
First phaseFshort-term effects of sibutramine vs placebo. At
baseline, subjects were randomly assigned to sibutramine
(15 mg) or placebo for 14 days (period 1), and after a 2 week
single-blind placebo washout period, the subjects switched
to the alternative therapy for another 14 days (period 2) (see
Figure 1). At baseline, and on the 14th day of each treatment
period, the subjects arrived fasting to the laboratory in the
morning for a test day (at the same hour each test day). Body
weight, blood pressure, pulse rate and any adverse events
were assessed, and a pregnancy test performed. A fasting
blood sample was collected for subsequent analysis of
glucose, insulin and lipids (triglycerides, HDL and LDL)
before the standardised breakfast was served. At 4 h after the
start of the breakfast, an ad libitum standardised lunch meal
was served on VIKTOR with a glass of water (200 ml). Patients
were asked to eat until satisfied and to drink the glass of
water. VAS to monitor the appetite were applied immediately
before and after the meals, as well as every hour between the
meals. The subjects were informed that they were participating in a 6 week long double-blind study with within-subject
design, to examine the effect of the drug on appetite, but
that neither we nor they would know when they received the
different study medications. No mention that food intake
was measured by VIKTOR was made until the end of the
study. Subjects were asked to keep their habitual eating
habits and physical activity level during the whole 6 weeks
long trial and not to change anything during this time
period. We also asked them to keep the same habits
according to working hours, physical habits and eating
pattern prior to test days.
Figure 1 Study design for the first phase of the study, measuring the shortterm effects of 15 mg sibutramine vs placebo.
Second phaseFlong-term effects of sibutramine treatment.
Immediately after the second test day during the first phase
of the study all subjects received 10 months of open
treatment with 15 mg of sibutramine. During this 10 months
period, all subjects participated monthly in group sessions
with a dietitian relating to nutritional education, food
choices, cooking methods as well as behavioural modification methods in order to improve weight reduction
and weight maintenance. If subjects are compliant with
the recommendations given at these sessions, they will
obtain about 15–20% of their daily energy from protein,
not more than 30 E% from fat and 50–55% of their daily
energy intake from carbohydrates, all according to the
Nordic Nutrition Recommendations (1996).10 In conjunction
with these monthly sessions, a nurse assessed body weight,
blood pressure, pulse rate, recorded any adverse event as
well as handled study medication and performed pregnancy
tests.
On the last day of the 10-month period of open treatment
with sibutramine, the subjects came for a test day for
measurements of appetite and eating behaviour, where the
procedure from the first phase of the study (see above) was
repeated.
The staff and the subjects were blinded to the results
from the first phase and also during the second phase of the
study.
Adverse events
All adverse events were recorded, including type, severity,
dates of onset and resolution as well as the relation of the
adverse event to study medication.
Statistics
First phase: The statistical package Statistica 5.5 and SAS
(Statistical Analysis Systems Inc., Cary, NC, USA) was used
for the statistical analysis. Repeated measures two-way
analysis of variance (ANOVA) was used to analyse experimental and laboratory data with treatment (placebo/
active) and time period (baseline/period 1/period 2) as
main factors. Two-way ANOVA was also used to analyse
the VAS ratings (Visual Analogue rating Scales) in the
two different periods separately with treatment and time as
main factors. Student’s t-test was used to test individual
means. w2 test was used to test the number of decelerated
eating curves.
Second phase: Student’s t-test was used to compare longterm treatment effects of sibutramine with baseline data. For
evaluating the relation between short-term effects on food
intake on long-term outcome on weight, correlations
(Pearson’s R) were used for continuous data and the Mann–
Whitney test was used for comparing weight loss for
responders and nonresponders. A nonparametric test was
chosen because of skewness in the number of subjects in
each of the groups.
International Journal of Obesity
Short-term effects of sibutramine
B Barkeling et al
696
Results
First phaseFshort-term effects of sibutramine vs
placebo
Eating behaviour. The intake of food at baseline, and on
the test days during the first and the second period, with the
different study medications are shown in Figure 2 and in
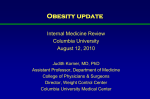
Table 1. The subjects receiving sibutramine during period 1
decreased their intake of food by 19% compared to baseline
measurements and when this group received placebo, their
intake of food returned to baseline level. The subjects
receiving placebo during the first period also reduced their
intake of food by 8% compared to baseline. When this group
received sibutramine during period 2, their intake was
reduced by 16% compared to baseline. The statistical
analysis with ANOVA, including baseline and the two test
days, showed a significant difference in intake between the
different time periods as well as for different treatments
(Po0.001). When baseline measurements were excluded and
analyses performed between sibutramine and placebo, the
active drug reduced food intake by 16% (Po0.0001, paired
Student’s t-test). The eating rate and the occurrence of
decelerated vs accelerated eating curves were unaffected by
the treatment (see Table 1).
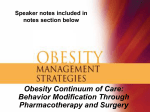
VAS ratings of appetite. Using Visual Analogue rating
Scales measuring motivation to eat (appetite), there was no
significant difference in ratings between sibutramine and
placebo for any of the following scales: desire to eat
(P ¼ 0.62), hunger (P ¼ 0.35), fullness (P ¼ 0.89) and prospective consumption (P ¼ 0.75) during period 1. During period 2
when the initial placebo effect was not present, there was an
obvious reduction in appetite when sibutramine was compared to placebo for the rating scale measuring the desire to
eat (Po0.05). The same trend towards a reduction was seen
for prospective consumption (P ¼ 0.057) and the scale
measuring hunger (P ¼ 0.079). The ratings for the scales
measuring desire to eat during periods 1 and 2 are shown in
Figure 3a and b, respectively.
Anthropometric data. Anthropometric data at baseline
and after 14 days with sibutramine and placebo are
presented in Table 1. The statistical analysis with ANOVA
showed a significant difference in weight between different
time periods as well as in relation to treatment (Po0.01).
When baseline measurements were excluded in the analyses
there was a significant reduction in weight when sibutramine was compared to placebo (Po0.01; paired Student’s ttest).
Figure 2 The intake of food at lunch (mean7s.d.) measured by VIKTOR at
baseline, and on test days during periods 1 and 2, with the different study
medications. The reduction of food is given as a percentage.
Adverse events. The most frequently reported adverse
event during the short-term period of the study was dry
Table 1 Selected anthropometrics and eating behaviour at baseline, and after 14 days with sibutramine and placebo (n ¼ 36), statistically tested with ANOVA and
paired t-test when appropriate (if nothing else are given)
Weight (kg)
Waist (cm)
Intake of food (g)
Eating rate (g/min)
Number of decelerated eating curves
Mean7s.d. are given.
International Journal of Obesity
Baseline
Sibutramine 15 mg
Placebo
ANOVA
113.3717.3
117714
408713
42713
55%
112.3716.9
116714
3357123
44717
66%
113.1716.6
116713
3997126
47717
65%
Po0.05
NS
Po0.0001
NS
NS (w2 test)
Paired t-test (excluding baseline)
Po0.01
Po0.0001
Short-term effects of sibutramine
B Barkeling et al
697
measurements, that is 300787 vs 4087146 g (Po0.01). The
smaller food intake after treatment was because of a shorter
duration of consumption, 7.972.5 min vs 10.273.0 min
(Po0.001) as the eating rate was the same after 10 months
of treatment compared to baseline, 42716 vs 42713 g/min
(NS). The number of subjects with decelerated and accelerated eating curves was also the same.
VAS ratings of appetite
Statistical analyses for the Visual Analogue rating Scales
measuring appetite were performed for the time points
immediately after the standardised breakfast and immediately before lunch. After breakfast, there was a clear decrease
in appetite ratings for fullness (Po0.05) and increase in
ratings of prospective consumption (Po0.05) and hunger
(P ¼ 0.052) after 10 months with sibutramine treatment
compared with baseline values. The ratings immediately
before lunch also showed the same trend towards a
reduction in appetite when on sibutramine but with no
statistical significant differences compared to baseline.
Figure 3
Subjective ratings of motivation to eat, that is appetite on Visual
Analogue rating scales (100 mm) at different time points of the test day for the
scales measuring desire to eat during period 1 (a) and period 2 (b).
mouth, reported by 12 subjects on sibutramine, but also by
four subjects on placebo. Insomnia was reported by six
subjects on sibutramine, and by one subject on placebo.
Anxiety was reported by two subjects when on sibutramine,
headache by two subjects on sibutramine and by three
subjects on placebo. Constipation was only reported by one
subject while taking placebo. Palpitations were reported by
one subject during the sibutramine period and by one during
placebo.
Second phaseFlong-term effects of sibutramine
treatment
Eating behaviour. After 10 months of treatment with
sibutramine the intake of food measured by the VIKTOR
equipment was reduced by 27% compared to baseline
Weight, waist and metabolic changes. In Table 2, data on
anthropometric data at baseline and after 10 months of
treatment with sibutramine are presented for the 27
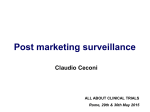
completers. After 10 months, a mean weight loss of 10%
(10.9 kg) had been achieved as well as significant reduction
in BMI and waist circumference compared to baseline. When
the same analysis was performed for all 36 patients initially
included using the principal of ‘last observation carried
forward’ the mean weight reduction was 8.2 kg or 7.2%.
There were substantial decreases in fasting levels of glucose
(from 6.172.3 to 5.470.9 mmol/l, Po0.05), insulin (from
95737 to 73728 mU/l, Po0.01) and triglycerides (from
1.670.7 to 1.270.5 mmol/l, Po0.001), but not in concentrations of LDL or HDL cholesterol. The blood pressure
recordings tended to decrease over the 10-month period, but
the observed differences were not significant (5 mmHg,
P ¼ 0.054).
The sequential mean weight changes during the 10 months
of open treatment with sibutramine are shown in Figure 4.
Short-term effects and long-term therapeutic outcome. In
order to evaluate if the short-term effects of sibutramine on
eating behaviour and appetite are related to the long-term
Table 2 Changes in anthropometrics at baseline and after 10 months of
open treatment with sibutramine (n ¼ 27), statistically tested with paired t-test
Weight (kg)
BMI (kg/m2)
Waist (cm)
Baseline
After 10 months with
sibutramine 15 mg
Paired t-test
112.7717.3
39.274.1
116713
101.8718.4
35.474.6
107715
Po0.001
Po0.0001
Po0.0001
Mean7s.d. are given.
International Journal of Obesity
Short-term effects of sibutramine
B Barkeling et al
698
Figure 4 The changes in weight (mean7s.d.) compared to baseline, month
per month, during the 10 months of open treatment with sibutramine.
therapeutic outcome, that is weight loss, groups of ‘responders’ and ‘nonresponders’ were defined. Responders regarding eating behaviour were defined as those who ate less food
on VIKTOR, when on sibutramine compared to their baseline food intake. Accordingly, nonresponders were defined as
the opposite. When the mean weight reduction at 10
months was compared between the two groups, responders
(n ¼ 22) had lost 11.876.2 (mean7s.d.) kg (median 12.0 kg)
and nonresponders (n ¼ 5) 6.872.7 (mean7s.d.) kg (median
8.1 kg), (Po0.05, Mann–Whitney test). Of the eight subjects
who dropped out during the second phase of the study, six
were responders (see definition above) and two were
nonresponders. Of these six responders, three had lost
weight and three had gained weight at their last attendance
(ranging from month one to seven) in the study. Of the two
nonresponders who dropped out, one had lost weight and
one had gained weight at their last attendance (at month 6
and 1, respectively).
A scattergram showing the correlation between the
reduction in food intake on VIKTOR when on sibutramine
vs baseline during the first phase and the long-term weight
loss is shown in Figure 5. If all 27 subjects are included in the
statistical analysis the r-value is 0.09 (NS). In this scatterplot,
two statistical outliers were suggested by visual estimations,
that is the subject who lost the most weight and the subject
who gained the most weight. Further, box plot analyses
revealed that these cases were the highest and lowest
extreme outliers on the weight reduction variable. If these
outliers are excluded in the statistical analyses, the r-value
would be 0.53 (Po0.01).
In order to obtain an ‘appetite index’ the ratings for each
of the different types of appetite scales (eg desire to eat,
hunger, satiety and prospective consumption) from all the
seven time points were added and divided by seven.
Responders were defined as those who had lower appetite
index when on sibutramine compared to baseline (less desire
to eat, less hunger, felt more full or thought they could eat
less), and nonresponders defined as those with higher scores
International Journal of Obesity
Figure 5 A scattergram showing the correlation between the reduction in
single-meal food intake (g) when on sibutramine vs baseline during the first
phase, and the long-term weight loss (kg).
when on sibutramine compared to baseline. For all four
different scales the weight reduction was greater for
responders compared to nonresponders (Mann–Whitney
tests), although not statistically different.
Discussion
In this study, sibutramine reduced the intake of food and
subjective motivation to eat. The short-term changes in the
intake of food are to some extent related to the long-term
weight reduction results in obese subjects.
The VIKTOR equipment, as an objective measurement of
appetite, together with rating scales measuring subjective
motivation to eat, has previously been used in a number of
studies with within-subject design to test and document
effects of drugs, dietary manipulations or other treatments
on appetite and satiety.5,6,11–17 The explanation for the
decreased food intake during treatment with sibutramine is
not likely to be a normal variability of the eating behaviour.
Data on the reproducibility of the VIKTOR measurements
have shown that variables such as eating rate and amount of
food eaten are stable over time, if physical habits and eating
patterns are controlled before test meal.6
The short-term effects of sibutramine on food intake in
obese subjects have been studied previously and our findings
are in accordance with these results. Rolls and collaborators
used a test meal of ‘smorgasboard type’ consisting of a
variety of standardised dishes. They also compared two
different doses of sibutramine 10 and 30 mg with placebo,
and found that the intake of food was reduced by 19 and
26%, respectively, after 14 days of treatment.18
A placebo effect was detected in the present study during
the first 14 days of the study. The reduction in intake and
appetite ratings compared to placebo would probably have
been greater if this placebo effect, probably because of high
Short-term effects of sibutramine
B Barkeling et al
699
expectations on treatment, had not been present. We believe
it was interesting to document such an effect. A run-in
period with placebo prior to the actual start of the study
could possibly have been one way to eliminate such an
effect.
When analysing the long-term effects of sibutramine
treatment on subjective motivation to eat measured repeatedly with VAS on test days, ANOVA (repeated measures)
cannot be applied, nor multiple comparisons with t-tests,
because of the likelihood of mass significances. Thus, we
had to choose a maximum of two time points of interest
to compare over time: one time point prior to a meal and
one time point after a meal. We chose the time point
after breakfast and not before lunch, since the size of the
breakfast meal was equal for all subjects but not the size
of the lunch meal intake. We chose ‘before lunch’
since the trial conditions up to that time point were
standardised for all subjects and the possible effects of
biological rhythm (morning vs night traits) would also be
wiped out.
When the subjective VAS ratings for appetite from the first
phase of the study were used to compare groups of
‘responders’ and ‘nonresponders’, there was a trend towards
a greater long-term weight reduction in the former. The
number of nonresponders was however very small and a
larger sample may have resulted in a statistically significant
difference.
Most clinical trials on weight-reducing drugs combine
drug administration with dietary advice prescribing a
reduced energy intake. Thus, in the present study monthly
group sessions with a dietitian was also included in the
second open phase of the study. How much of the
achieved weight loss on sibutramine could be attributed to
the drug and the dietary intervention, respectively? The
placebo-controlled trials with sibutramine including energy
restriction have after 6 months resulted in almost no
changes in weight when on placebo þ dietary intervention
compared to a weight reduction of 4–12% when on
sibutramine+dietary intervention.2 Thus, it seems like the
major part of the weight loss could be attributed to the
actual drug.
There are several comorbid conditions associated with
obesity including type II diabetes, coronary heart disease
(CHD), dyslipidaemia and hypertension. Weight reduction
improves blood glucose dramatically in diabetes and also
reduces several risk factors for CHD3,19 and should therefore
be considered a first-line therapy.
In this study, long-term treatment with sibutramine was
associated with a significant reduction not only in weight
and BMI but also in waist circumference, which is a marker
for increased risk for metabolic comorbid conditions not
only in the obese, but also in overweight people. Despite our
patients being primarily selected to the study for obesity
treatment, rather than for associated complications, we
found significant reductions in fasting plasma glucose
(11%), insulin (23%) and triglyceride levels (25%).
These findings indicate a lowered risk for the development
of CHD and diabetes. In contrast to other studies,3,20 no
significant changes in total cholesterol, LDL-cholesterol or
HDL-cholesterol levels were seen when baseline values were
compared with 10 months data. This discrepancy can be
explained by the selection of patients with baseline values
being within the normal range for these parameters. An
alternative explanation could be that our treatment period
was shorter than in other studies.3,20
Interestingly, we found that weight loss continued
throughout the 10 months treatment period with only a
slight tendency to attenuate during the last month. This is
also in accordance with data from the STORM study,3 but in
contrast to many other obesity treatment programmes where
most of the weight loss is achieved during the first 6 months
of treatment.21
In conclusion, the short-term effects of sibutramine on
appetite and eating behaviour can be identified by means of
the VIKTOR equipment and Visual Analogue rating Scales.
The short-term reduction in food intake when on sibutramine are to some extent related to the long-term therapeutic
outcome, that is weight reduction, in obese subjects.
Sibutramine is a well-tolerated and effective treatment in
promoting weight loss in obese patients. Sibutramine also
improves several risk markers such as waist circumference,
insulin levels, glucose levels and triglycerides associated with
obesity.
Acknowledgements
Our thanks are particularly to Birgitta Spetz and Karin
Östling and also to Birgit Hännikäinen, Lena Mannström,
Viveka Petre Larsson, Jonas Ramsten and Josefine Jonasson
for always taking good care of the patients in the study. This
study was supported by grants from Abbott Pharmaceutical
(former Knoll Pharmaceutical).
References
1 WHO. Obesity, preventing and managing the global epidemic. World
Health Organisation: Geneva; 1997.
2 McNeely W, Goa KL. SibutramineFa review of its contribution to
the management of obesity. Drugs 1998; 56: 1093–1124.
3 James WP, Astrup A, Finer N, Hilsted J, Kopelman P, Rössner S,
Saris WHM, Van Gaal LF. Effect of sibutramine on weight
maintenance after weight loss: a randomised trial. Lancet 2000;
356: 2119–2125.
4 Lissner L, Barker DJP, Blundell JE, Dietz WH, Epstein LH, Jeffery
RW, Remschmidt H, Rolls BJ, Rössner S, Saris WHM. Group
report: what are the bio-behavioral determinants of body weight
regulation? In: Bouchard C, Bray GA (eds.). Regulation of body weight:
biological and behavioral mechanisms, John Wiley & Sons; Chichester,
New York, Brisbane, Toronto, Singapore; 1996. pp 159–177.
5 Barkeling B, Rössner S, Björvell H. Effects of a high-protein meal
(meat) and a high-carbohydrate meal (vegetarian) on satiety
measured by automated computerized monitoring of subsequent
food intake, motivation to eat and food preferences. Int J Obes
Relat Metab Disord 1990; 14: 743–751.
6 Barkeling B, Rössner S, Sjöberg A. Methodological studies on
single meal food intake characteristics in normal weight and
obese men and women. Int J Obes Relat Metab Disord 1995; 19:
284–290.
International Journal of Obesity
Short-term effects of sibutramine
B Barkeling et al
700
7 Lindgren AC, Barkeling B, Hägg A, Ritzén M, Marcus C, Rössner S.
Eating behaviour in Prader–Willi syndrome, normal weight and
obese control groups. J Pediatr 2000; 137: 50–55.
8 Meyer J-E, Pudel V. Experimental studies on food intake in
obese and normal weight subjects. J Psychosom Res 1972; 16:
305–308.
9 Blundell JE, Rogers PJ, Hill AJ. Evaluating the satiating power of
foods: implications for acceptance and consumption. In: Solms J
(ed). Chemical composition and sensory properties of food and their
influence on nutrition. Academic Press; London; 1988. pp 205–219.
10 Nordic Nutrition Recommendations. Scand J Nutr 1996; 40: 161–165.
11 Linné Y, Barkeling B, Rössner S, Rooth P. Vision and eating
behavior. Obes Res 2002; 10: 92–95.
12 Barkeling B, Granfelt Y, Björck I, Rössner S. Effects of carbohydrates in the form of pasta and bread on food intake and satiety
in man. Nutr Res 1995; 15: 467–476.
13 Hylander B, Barkeling B, Rössner S. Eating behaviour in
continuous ambulatory peritoneal dialysis and hemodialysis
patients. Am J Kidney Dis 1992; 6: 592–597.
14 Hylander B, Barkeling B, Rössner S. Changes in patients’ eating
behavior: in the uremic state, on continuous ambulatory
peritoneal dialysis treatment, and after transplantation. Am J
Kidney Dis 1997; 29: 691–698.
International Journal of Obesity
15 Näslund E, Barkeling B, King N, Gutniak M, Blundell J, Holst J,
Rössner S, Hellström P. Energy intake and appetite are suppressed
by glucagon-like peptide-1 (GLP-1) in obese men. Int J Obes Relat
Metab Disord 1999; 23: 304–311.
16 Rössner S, Barkeling B, Asp A, Flaten H, Fuglerud P. Effects of
weight loss on single meal eating behaviour in obese subjects. Int
J Obes Relat Metab Disord 1996; 20: 287–289.
17 Rössner S, Barkeling B, Erlanson-Albertsson C, Larsson P, WåhlinBoll E. Intravenous enterostatin does not affect single meal food
intake in man. Appetite 1995; 24: 37–42.
18 Rolls BJ, Shide DJ, Thorwart ML, Ulbrecht JS. Sibutramine reduces
food intake in non-dieting women with obesity. Obes Res 1998; 6:
1–11.
19 Andersson JW, Konz EC. Obesity and disease management:
effect of weight loss on comorbid conditions. Obes Res 2001; 9:
326S–334S.
20 McMahon FG, Fujioka K, Singh BN, Mendel CM, Rowe E, Rolston
K, Johnson F, Mooradian AD. Efficacy and safety of sibutramine
in obese White and African American patients with hypertension.
Arch Intern Med 2000; 160: 2185–2191.
21 Bray GA. Drug treatment of overweight. Contemporary diagnosis
and management of obesity. Handbooks in Health Care Co.:
Newtown, PN; 1998. pp 246–273.