Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
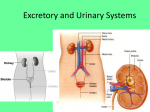
ADDITIONAL ARTICLES SIMPLIFIED NEUROPHYSIOLOGY OF THE LOWER URINARY TRACT Lars Viktrup, MD, PhD, and Richard C. Bump, MD Urinary incontinence is an important health problem with a significant effect on the quality of life of its sufferers. Despite the prevalence and impact of the condition, incontinent patients seem to accept their symptoms for years before they consult their physician. When they do finally consult their physician, an unnecessarily high proportion is referred to a specialist. However, though the pathophysiology is complex, urinary incontinence can be effectively treated in primary care practice with a basic knowledge of the anatomy and function of the lower urinary tract. This review presents updated findings on the neurophysiology of the lower urinary tract (LUT), focusing on the role of the central and peripheral autonomic and somatic nervous systems during urinary storage and voiding. (Prim Care Update Ob/ Gyns 2003;10:261–264. © 2003 Elsevier Inc. All rights reserved.) Lower urinary tract symptoms (LUTS) and urinary incontinence in particular affect the quality of life of many men and women. Nevertheless, incontinent patients seem to accept their symptoms for years before they consult their physician.1 Furthermore, for those who do consult their physician, an unnecessarily high proportion is referred to a specialist for assessment and treatment.2 This is unfortunate, since urinary incontinence may be manFrom Eli Lilly Research Laboratories, Indianapolis, Indiana. Volume 10, Number 5, 2003 aged in a primary care practice setting with reference to a basic description of the LUT. To maintain urinary continence, intact anatomical structures in and around the urethra together with a correct position of the bladder neck are a necessity, while the comprehensive innervation of the LUT needs to be intact. The central and peripheral autonomic and somatic nervous systems synchronize urinary storage and voiding via inhibitory and facilitatory activity. Certain neurotransmitters play an important role in this function and new pharmacological opportunities to treat both urge urinary incontinence (UUI) and stress urinary incontinence (SUI) are currently being investigated.3,4 A knowledge of the basic anatomy and function of the LUT is important in understanding how these medications can be effective. The aim of this article is to provide an updated simple review of the neurophysiology of the LUT. The Bladder and the Urethral Muscles The urinary bladder is a hollow, muscular organ with smooth muscle fibers (detrusor muscle) extending in many directions, allowing it to expand during urine storage and contract during voiding. UUI is a result of overactivity in this muscle. The smooth muscle layer runs as a continuum from the detrusor in the bladder via the bladder neck and ends in the proximal part of the urethra. The urethral muscles may © 2003 Elsevier Inc., all rights reserved. 1068-607X/03/$30.00 ● be divided into an inner layer of smooth muscle fibers and an outer layer of striated muscle fibers forming the rhabdosphincter (Figure 1). The urethral smooth muscles are primarily longitudinal and may shorten and widen the urethral lumen during voluntary voiding, while a thinner circular outer sheath provides some resting tone during storage. 5 The urethral smooth muscle extends down most of the length of the urethra. The striated rhabdosphincter is thickest in the middle two-thirds of the urethra, while the muscle proximally and distally is horseshoe-shaped and intermingled posterior with connective tissue in the anterior wall of the vagina.6 In addition to the muscular structures, the urethral lumen lining, the urethral vascular plexus, and the collagen and elastin connective tissue of the urethra contribute to continence. Another important factor affecting SUI is the pelvic floor with its levator ani and coccygeus muscle. The pelvic floor muscles are suspended like a hammock between the pubic bone in the front and the coccyx bone behind. The pelvic floor supports and maintains the position of the pelvic organs and attaches to the anterior vaginal wall, allowing compression of the urethra against the vaginal wall. These muscles help resist the tendency of the bladder neck to thrust downward when physical activities such as running, jumping, coughing or sneezing produce a sudden increase in abdominal pressure. Conscious tightening of these muscles helps doi:10.1016/S1068-607X(03)00043-X 261 VIKTRUP AND BUMP well as nociceptors. Injury to the proprioceptive fibers of the pelvic floor may account for some women’s decreased ability to perform correct pelvic floor muscle training.8 Bladder Filling Figure 1. The muscle types in the bladder, urethra, and the pelvic floor. elevate and stabilize the anterior vaginal wall and urethra. The Central Nervous System Different centers in the brain and the spinal cord have various roles for the urinary function. The cerebral cortex permits conscious control over micturition by allowing voluntary contraction of the striated rhabdosphincter and of the levator ani muscle to resist micturition and stress incontinence. It also provides input to the pontine micturition center in the brainstem to allow voluntary suppression of detrusor activity after early childhood. The pontine micturition center coordinates the contraction of the detrusor muscle and relaxation of the striated urethral rhabdosphincter during voiding. In the spinal cord, all impulses reaching the bladder and the urethra are mediated via nerves originating in the thoracic-lumbar sympathetic division and the sacral parasympathetic and somatic divisions (Figure 2). The spinal cord 262 also serves as a relay station for sensory information from the bladder, urethra, and the pelvic floor. The Peripheral Nervous System The peripheral nervous system innervates the bladder and the urethra with autonomic efferent sympathetic fibers via the hypogastric nerve and the bladder with parasympathetic fibers to the bladder via the pelvic nerve (Figure 2). The somatic efferent motor innervation to the striated rhabdosphincter runs in the pudendal nerve, while direct sacral fibers innervate the levator ani muscle (Figure 2).7 The somatic and sympathetic divisions promote storage while the parasympathetic division promotes voiding. Sensory impulses from the bladder or the urethra travel back to the spinal cord via the same sympathetic, parasympathetic, or somatic nerves that supply the area with efferent fibers. The sensory stimuli include stretch-, tension-, friction-, and proprioceptive receptors as When the bladder begins to fill with urine, stretch receptors in the bladder wall generate nerve impulses that are transmitted along sensory fibers to the central nervous system (CNS). These afferent impulses cause reflex activation of the sympathetic nucleus, a cluster of neurons located in the upper lumbar spinal cord. The sympathetic nucleus responds by firing impulses along the hypogastric nerve back to the bladder and urethra, with subsequent release of the neurotransmitter norepinephrine. In the bladder the beta-adrenergic receptors on the detrusor muscle respond to norepinephrine by causing relaxation and allowing the bladder to fill without an increase in pressure or change in tone. At the same time alpha1-adrenergic receptors in the urethral smooth muscles respond to norepinephrine by bringing about contraction of the urethral smooth muscles. During filling, there is also tonic activity of the striated urethral rhabdosphincter. This activity can be augmented with voluntary contraction of the rhabdosphincter. As the detrusor muscle relaxes and the urethral smooth and striated muscles contract, the urethral pressure remains greater than the bladder pressure, facilitating urine storage without urine loss. Bladder Emptying Normal voiding involves both voluntary and involuntary neural regulation. When the bladder reaches capacity, stimuli from the bladder are transmitted to the pontine micturition center. If voiding is initiPrim Care Update Ob/Gyns LOWER URINARY TRACT ing UUI by blocking the effect of acetylcholine on muscarinie receptors on the detrusor muscle. CONTRACTION OF THE RHABDOSPHINCTER Figure 2. The innervation of the bladder, urethra, and the pelvic floor. ated, the pontine micturition center stimulates output from the parasympathetic nucleus in the spinal cord, which results in detrusor contractions via release of acetylcholine and stimulation of the muscarinic bladder receptors. The pontine micturition center also sends impulses to the pudendal motor nucleus, which inhibits the activity of the pudendal nerve and the rhabdosphincter. This combined activity allows the rhabdosphincter to relax in coordination with the contraction of the bladder. Pontine impulses also suppress sympathetic activity to the bladder and urethra. The net effect is that bladder pressure increases due to contraction of the detrusor muscle, while urethral pressure decreases due to relaxation of the rhabdosphincter, permitting voiding to occur. Volume 10, Number 5, 2003 Conscious Inhibition of the Micturition Reflex The cerebral cortex is the area of the brain that mediates awareness and conscious thought. Thus, the cerebral cortex is involved in the conscious perception of the need to urinate and the decision to initiate voiding. When the decision is made to postpone bladder emptying, the cerebral cortex: 1) sends signals to the lower urinary tract to contract the rhabdosphincter and levator ani, to resist urination and urine loss, and 2) suppresses parasympathetic impulses from the pontine micturition center that normally mediate micturition. New and old pharmaceutical agents have proved to alleviate premature detrusor contractions caus- The rhabdosphincter and external anal sphincter are innervated by the pudendal nerve. The pudendal nerve stimulates contraction of these muscles via the neurotransmitter acetylcholine acting on nicotinic receptors. Nerve tracts from higher centers in the central nervous system (the medulla and locus ceruleus) terminate in Onuf’s nucleus in the spinal cord. These nerves use serotonin and norepinephrine as their neurotransmitters. At Onuf’s nucleus they synapse with pudendal motor neurons. The neurotransmitter glutamate plays an important role for initiating the pudendal activity in Onuf’s nucleus. Thus, there are three sets of neurotransmitters involved— serotonin, norepinephrine and glutamate, which are released in Onuf’s nucleus, and acetylcholine, which is released by pudendal neurons and which stimulates receptors on the rhabdosphincter and external anal sphincter. In effect, 1) glutamate starts the pudendal message, 2) serotonin and norepinephrine working at the proximal end of the pudendal nerve by stimulating its motor neuron cell bodies to amplify the message, while 3) acetylcholine works at the distal end of the pudendal nerve where its release causes the rhabdosphincter to contract. Increasing the pudendal activity in Onuf’s nucleus causing the rhabdosphincter to contract more forcefully may avoid SUI if a sudden increase in abdominal pressure occurs. Increasing the availability of norepinephrine and serotonin in Onuf’s nucleus is believed to intensify this pudendal activity and new pharmaceutical agents to treat women with SUI are therefore 263 VIKTRUP AND BUMP currently being tested for this purpose.9 CONTRACTION OF THE PELVIC FLOOR Direct sacral nerves carry impulses mediated by acetylcholine to the levator ani stimulating contraction via nicotinic receptors.4 INHIBITION OF PARASYMPATHETIC ACTIVITY At the same time that the rhabdosphincter and levator ani are stimulated to contract, inhibitory impulses are transmitted along the hypogastric nerve to inhibit contraction of the detrusor muscle. The net effect of this neural activity is that urethral pressure increases with the contraction of the rhabdosphincter and the levator ani, while vesical pressure decreases with the relaxation of the detrusor muscle. This keeps urine contained in the bladder. After additional urine accumulates, the micturition reflex occurs again. Al- 264 though the urge to urinate can usually be temporarily suppressed again as more urine accumulates, the urge sensations ultimately become irresistible and micturition occurs. 6. 7. References 1. Toozs-Hobson P, Cardozo L. Family Doctor Guide to Urinary Incontinence in Women. London: Dorling Kindersley Limited, 1999. 2. Lose G, Jacobsen AT, Madsen H, Thorsen P, Tibæk S, Johansen B. Alment praktiserende lægers viden om og holdninger til undersøgelse og behandling af kvinder med urininkontinens [General practitioners’ knowledge about and attitudes towards assessment and treatment of women with urinary incontinence]. Ugeskr Læger 2001;163:5183–8. 3. De Groat WC, Yoshimura N. Pharmacology of the lower urinary tract. Annu Rev Pharmacol Toxicol 2001; 41:691–721. 4. Yoshimura N, De Groat WC. Neural control of the lower urinary tract. Int J Urol 1997;4:111–25. 5. Lose G. Simultaneous recording of pressure and cross-sectional area in the female urethra: a study of urethral closure function in healthy and 8. 9. stress incontinent women. Neurourol Urodyn 1992;11:55–89. Thind P. The significance of smooth and striated muscles in the sphincter function of the urethra in healthy women. Neurourol Urodyn 1995;14: 585–618. Barber MD, Bremer RE, Thor KB, Dolber PC, Kuehl TJ, Coates KW. Innervation of the female levator ani muscles. Am J Obstet Gynecol 2002; 187:64 –71. Viktrup L. The risk of lower urinary tract symptoms 5 years after the first delivery. Neurourol Urodyn 2002;21: 2–29. Thor KB, Katofiasc MA. Effects of duloxetine, a combined seretonin and norepenephrine reuptake inhibitor on central neural control of lower urinary tract function in the chloralose-anesthetized female cat. J Pharmacol Exp Ther 1995;274:1014 –24. We are grateful to Plexus Learning Design, LLC for the illustrations used in Figures 1 and 2. Address correspondence and reprint requests to: Lars Viktrup, MD, PhD, Eli Lilly and Company, Faris II, Drop Code 6112, Indianapolis, IN 46285. Prim Care Update Ob/Gyns