Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
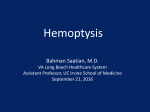
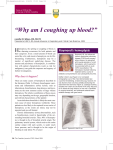
of tuberculosis appeared to be unlikely, and oral corticosteroid therapy was begun, leading to a rapid normalization of the symptoms and to a resolution of the radiographic abnormalities. Corticosteroids were discontinued after a 12-month treatment period, and regular clinical, radiologic, and sonographic controls failed to detect a recurrence of the disease for ⬎ 1 year. Multiple primary disorders have been associated with pulmonary reactions and pathologic features of BOOP, including respiratory infections with various bacterial and viral agents, toxic inhalants, adverse drug reactions, or collagen vascular disease. In a large proportion of cases, however, no etiology may be apparent (idiopathic BOOP). On the basis of the available serologic data, the patient may have had a respiratory infection, presumably caused by C pneumoniae, as has previously been observed.5 The present case represents an unusual radiographic manifestation of BOOP, with an almost symmetrical involvement of the two apical lung segments. Comparable abnormalities affecting both upper lobes associated with BOOP have not been reported previously. Differential diagnosis of bilateral apical consolidations is primarily suggestive of tuberculosis, which could be excluded in the patient. The case presented herein demonstrates that BOOP can both clinically and radiographically mimic tuberculosis. the left pulmonary artery. Following this procedure, he developed recurrent episodes of hemoptysis, cough, and left upper lobe consolidation. Treatment resulted in clinical but no radiologic resolution. At age 6, a new right systemic-to-pulmonary anastomosis was needed, as the left one was no longer functioning. After placement of the second shunt, the hemoptysis disappeared. At age 14, flexible bronchoscopy revealed a foreign body granuloma at the left secondary carina. Rigid bronchoscopy and laser photoresection showed it to be the left vascular prosthesis, placed 10 years before. Surgery failed to remove it. (CHEST 2000; 118:865– 867) References A 14-year-old boy with history of single ventricle, left type, left pulmonary artery stenosis, and left great vessels transposition, diagnosed by cardiac catheterization during the postnatal period, was sent to the Pulmonary Department for chest radiograph abnormalities. At age 4, the patient developed worsening cyanosis and decreased exercise tolerance. A cardiac catheterization was performed, confirming the previous diagnosis and showing the development of collateral circulation, in the form of a great number of vessels branching from the descending aorta toward both lungs, particularly the left one. Bronchial circulation was poor bilaterally, particularly in the left lung where it was almost absent. A left systemic-to-pulmonary anastomosis was performed (from the left subclavian artery to the left pulmonary artery; Fig 1), using a tubular 6-mm polytetrafluoroethylene prosthesis (Gore-Tex; W.L. Gore; Flagstaff, AZ). In the immediate postoperative period, a new catheterization showed increase in blood flow to the left lung. Nine months after the surgery, the patient presented an episode of cough and hemoptysis, and chest radiography showed consolidation and atelectasis on the left upper lobe (LUL). The patient was treated with antibiotics, and aspirin was discontinued. The picture improved both clinically and radiologically, although a small opacity persisted in the LUL in the following chest radiographs. This abnormality was further investigated by CT of the chest, which only showed lung consolidation. Similar clinical 1 Epler GR, Colby TV, McLoud TC, et al. Bronchiolitis obliterans organizing pneumonia. N Engl J Med 1985; 312: 152–158 2 Davidson AG, Heard BE, McAllister WAC, et al. Cryptogenic organizing pneumonia. Q J Med 1983; 52:382–393 3 Bartter T, Irwin RS, Nash G, et al. Idiopathic bronchiolitis obliterans organizing pneumonia with peripheral infiltrates on chest roentgenogram. Arch Intern Med 1989; 149:273– 279 4 Izumi T, Kitaichi M, Nishimura K, et al. Bronchiolitis obliterans organizing pneumonia: clinical features and differential diagnosis. Chest 1992; 102:715–719 5 Diehl JL, Gisselbrecht M, Meyer G, et al. Bronchiolitis obliterans organizing pneumonia associated with chlamydial infection. Eur Respir J 1996; 9:1320 –1322 Recurrent Hemoptysis Following a Systemic-toPulmonary Anastomosis in a Child With a Complex Congenital Cardiomyopathy* Jose Pablo Diaz-Jimenez, MD, PhD; Alicia N. Rodriguez, MD; and Martin Anselmo Andres, MD A 14-year-old boy with a history of congenital cardiopathy is presented. At age 4, a left systemic-topulmonary fistula was performed, using a tubular prosthesis to anastomose the left subclavian artery to Key words: foreign body; hemoptysis; laser photoresection; vascular prosthesis Abbreviation: LUL ⫽ left upper lobe is a frequent complication in children with H emoptysis congenital cardiopathies undergoing surgery. We present an unusual case of hemoptysis in a 4-year-old child after the performance of a systemic-to-pulmonary anastomosis secondary to a severe congenital cardiopathy. The possible cause of the hemoptysis was found 10 years later, after a flexible bronchoscopy. Case Presentation *From the Endoscopy and Laser Unit (Drs. Diaz-Jimenez and Rodriguez), Hospital Duran i Reynals, L’Hospitalet de Llobregat, Barcelona; and Pulmonary Pediatric Section (Dr. Andres), Hospital Infantil Universitario Virgen del Rocio de Sevilla, Spain. Manuscript received June 28, 1999; revision accepted March 1, 2000. Correspondence to: Jose Pablo Diaz-Jimenez, Endoscopy and Laser Unit, Pulmonary Department, Ciutat Sanitària de Bellvitge, Feixa Llarga s/n, E-08907 L’Hospitalet de Llobregat, Barcelona, Spain; e-mail: [email protected] CHEST / 118 / 3 / SEPTEMBER, 2000 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21952/ on 06/17/2017 865 Figure 3. Endobronchial image showing sutures, granulation tissue, and part of the vascular prosthesis. Figure 1. Location of the left systemic-to-pulmonary anastomosis. episodes recurred occasionally, with the same characteristics of cough, hemoptysis, and worsening of the LUL radiologic abnormalities. Two years after the surgery, at age 6, a new systemic-topulmonary anastomosis was performed, this time to the right pulmonary artery, since the previous one had stopped working. After the second operation, the episodes of hemoptysis diminished progressively and finally disappeared, but the consolidation-like image was persistent in the LUL. At age 14, the patient was scheduled for cardiac surgery; as a part of the presurgical evaluation, he underwent a flexible bronchoscopy in order to clarify the persistent chest radiograph image (Fig 2). Flexible bronchoscopy showed a tracheal bronchus as an incidental finding, a normal right tracheobronchial tree, and a granulomatous-type lesion located at the level of the left secondary carina. Since some sutures were visible, a presumptive diagnosis of foreign body granuloma was made, and the patient was transferred to us for laser bronchoscopy evaluation. The patient underwent rigid bronchoscopy under general anesthesia. After removal of the granulation tissue, we found a mesh-like foreign body emerging from the lateral wall of the left upper bronchus, which appeared to be the endovascular prosthesis (Fig 3). No attempt was made to remove it, and the patient was referred to thoracic surgery for evaluation. A left thoracotomy was performed and was complicated by excessive fibrous adhesions and a cardiac arrest. It was not possible to remove the prosthesis. Since then, the patient has remained clinically stable. The episodes of hemoptysis have not recurred, and the LUL chest radiograph abnormalities have not resolved. Discussion Figure 2. Chest radiograph at age 14, showing the persistent consolidation image at the LUL, and atelectasis. A single ventricle is a rare and complex congenital cardiopathy, characterized by the presence of one ventricle, which receives two atrioventricular valves and empties into both the aorta and the pulmonary artery.1 Transposition of the great arteries and pulmonary stenosis are common accompanying malformations. Hemodynamically, there is bidirectional shunting at the ventricular level. Surgical correction is very difficult, but palliation of the cyanosis can be achieved by the creation of a systemicto-pulmonary anastomosis by means of a tube graft, or without using vascular prosthesis. This will increase the pulmonary blood flow, bypassing the pulmonary stenosis.2 Causes of hemoptysis in children with congenital cardiopathies, whether they undergo surgery or not, are many: extracorporeal circulation, pulmonary infections, coagulopathies, vascular disorders. A vascular prosthesis as a cause of bronchial obstruction and hemoptysis is very unusual, and reports in the literature are scant. Some cases 866 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21952/ on 06/17/2017 Selected Reports of chronic hemoptysis are associated with the development of aortobronchial fistulas involving prosthetic aortic grafts.3 Artery bands can migrate and produce bronchial obstruction. A case of a 4.5-kg boy was presented by Parry et al.4 This patient developed cough after placement of a pulmonary band, and episodes of consolidation were seen on the chest radiographs. Two bronchoscopies failed to reveal any abnormality other than purulent drainage coming from the right middle and lower lobes. The intact Silastic band (Dow Corning; Auburn, MI) used for the pulmonary banding was recovered from the right lung at age 5. Some other reports involving pulmonary band migrations through the vascular wall have been published, most of them associated with infections at the site of the prosthesis followed by vascular erosion.5–7 To our knowledge, this is the first report of a vascular prosthesis migrating and eroding the bronchial wall. We presume that the mechanism is the same as the one involved in the aortobronchial fistula formation: chronic inflammation secondary to foreign body reaction, and/or direct pressure necrosis of the wall. Unfortunately, it is not possible at present to know the exact situation of the prosthesis. After the attempted prosthesis removal and the cardiac arrest, the patient had a complicated postoperative period, and the family decided not to perform any additional studies or procedures. We speculate that the prosthesis may be still connected to the anastomosis. It is possible that the erosion of the bronchial wall and kinking of the vessels was the reason why the systemic-to-pulmonary bypass stopped working 2 years after the surgery. The graft most probably caused endobronchial obstruction and episodes of postobstructive infections. It is important to consider prosthesis migration in any patient with a thoracic vascular prosthesis who develops recurrent hemoptysis and/or recurrence of other respiratory symptoms and nonresolving radiologic abnormalities. ACKNOWLEDGMENT: The authors thank Dr. Mark Mercurio for reviewing and correcting the manuscript. References 1 Ionescu MI, Macartney FJ, Wooler GH. Intracardiac repair of single ventricle with pulmonary stenosis. J Thorac Cardiovasc Surg 1973; 65:602– 607 2 Holden MP, Macartney FJ, Ionescu MI. Surgical palliation of single ventricle with pulmonary stenosis. Ann Thorac Surg 1973; 15:578 –587 3 Wheeler AP, Loyd JE. Fatal hemoptysis: aortobronchial fistula as a preventable cause of death. Crit Care Med 1989; 17:1228 –1230 4 Parry RL, Gordon LS, Sherman NJ. Pulmonary artery band migration producing endobronchial obstruction. J Pediatr Surg 1997; 32:48 – 49 5 Albus RA, Trusler GA, Izukawa T, et al. Pulmonary artery banding. J Thorac Cardiovasc Surg 1984; 88:645– 653 6 Romer J, Brom AG, Nauta J. Bands inside the pulmonary artery: a complication of the Damman-Muller procedure. Ann Thorac Surg 1967; 3:449 – 454 7 Kumar RV, Roughneen PT, deLeval MR. Mycotic pulmonary artery aneurism following pulmonary artery binding. Eur J Cardiothorac Surg 1994; 8:665– 666 Normal Diffusing Capacity in Patients With PiZ ␣1Antitrypsin Deficiency, Severe Airflow Obstruction, and Significant Radiographic Emphysema* Jeffrey S. Wilson, MD; and Jeffrey R. Galvin, MD, FCCP ␣1-Antitrypsin deficiency is usually suspected clinically in young adults with irreversible airflow obstruction that is out of proportion to their smoking history. Many patients with ␣1-antitrypsin deficiency receive an initial diagnosis of asthma or chronic bronchitis. Measurement of the diffusing capacity of the lung for carbon monoxide (DLCO) has been recommended as a way to help distinguish emphysema from asthma and chronic bronchitis. In this article, we describe four patients with severe ␣1antitrypsin deficiency, each of whom had a repeatedly normal DLCO despite having a significant component of fixed airway obstruction and prominent panacinar emphysema on high-resolution CT scan (HRCT). Each patient also demonstrated significant bronchodilator responsiveness, and two patients received an initial diagnosis of asthma. Potential explanations for these findings are discussed. We report these findings to illustrate the limitations of DLCO in this setting. ␣1-Antitrypsin deficiency should be considered in patients with fixed airway obstruction that is out of proportion to their age and smoking history, regardless of their diffusing capacity and response to bronchodilators. (CHEST 2000; 118:867– 871) Key words: ␣1-antitrypsin deficiency; chronic obstructive lung disease; CT; diffusing capacity; emphysema Abbreviations: ␣1-AT ⫽ ␣1-antitrypsin; Dlco ⫽ diffusing capacity of the lung for carbon monoxide; HRCT ⫽ high-resolution CT evere ␣ -antitrypsin (␣ -AT) deficiency may result in S the development of premature emphysema. It is usu1 1 ally suspected clinically in young adults with irreversible airflow obstruction that is out of proportion to their smoking history.1–3 Early diagnosis is important to prevent disease progression, through implementation of smoking cessation.4 –5 The data supporting the efficacy of ␣1-AT *From the Departments of Internal Medicine and Radiology, University of Iowa, Iowa City, IA. Manuscript received June 26, 1997; revision accepted March 13, 2000. Correspondence to: Jeff Wilson, MD, University of Iowa, Department of Internal Medicine, C33 GH, 200 Hawkins Dr, Iowa City, IA 52242-1081; e-mail: [email protected] CHEST / 118 / 3 / SEPTEMBER, 2000 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21952/ on 06/17/2017 867