Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
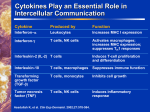
/vWlDJNf~OGY AND EL.SEVIER FEZMSImmunology and Medical Microbiology 12 (1995) 17-28 MICROBIOLOGY The ability of peripheral blood mononuclear cells ( PBMC) of syphilitic patients to produce IL-2 J. Podwiiiska a**, R. iaba b, M. Chomik a, J. Bowszyc b a Institute of Immunology and Experimental Therapy, Polish Academy of Sciences, Czerska 12, 53-l 14 Wroctaw. Poland b Department of Dermatology, School of Medicine, Poznari. Poland Received 13 February 1995; revised 15 May 1995: accepted 15 May 1995 Abstract The cell-mediated immune response of importance in protection against Treponema pallidum, is distinctly suppressed in some stages of the disease. This may be a result of decreased ability of cells to produce IL-2, or IL-2 absorption by different factors. The experiments were designed to evaluate the ability of peripheral blood mononuclear cells (PBMC) of patients with different stages of syphilis to produce IL-2, and to investigate the causes which could possibly limit its activity. The ability of the PBMC of syphilitic patients to produce IL-2 develops at the beginning of the disease, reaching a maximum in primary seropositive syphilis. In the next stages of the disease this capability is distinctly lowered. The lowest was in malignant syphilis and tabes dorsalis, i.e. during severe disease. Absorption of adherent cells from PBMC increased the ability of lymphocytes to produce IL-2. The highest level of this interleukin was observed at the stages of the disease where suppression was the deepest. Sera of both control and syphilitic patients contained IL-2 inhibitor. Its level was the highest in early and late latent syphilis where no symptoms of disease were present. In all syphilitic sera a distinctly elevated level of soluble IL-2 receptors (sIL-2R) was also found. Its high level was noted in sera of patients in which PBMC had the weakest ability to produce IL-2. These findings suggest that sIL-2R may be bound to IL-2 and in this way would lead to weakening of T cell function and of resistance against Treponemu pallidurn infection. Keywords: Treponema pallidum; Interleukin-2; Serum IL-2 inhibitor; Soluble IL-2 receptor; Lymphocyte marker 1:Introduction In syphilis, as in other infectious diseases where bacteria are intracellular, the cell-mediated immune response plays a pivotal role in host defence against infectious agent [I]. This form of immunological response, as is known from studies on experimen- Corresponding author. Tel: +48 (71) 73 22 74; Fax: +48 (71) 67 91 Il. l tally induced syphilis in rabbits, is, in some periods of the disease duration, distinctly inhibited [l-3]. This was found as diminished ability of lymphocytes to produce migration inhibition factor (MIF), which affects various antimicrobial functions [4]. and weakening the ability to mount delayed type hypersensitivity (DTH) [5]. R ecent data have also indicated that spleen cells of syphilitic rabbits are not able to produce antitreponemal lymphotoxin (ATJL)[6] which kills treponemes both in vitro [7,8] and in vivo [9]. In some periods in the course of syphilis in rabbits IL-2 0928-8244/95/.%X9.50 0 1995 Federation of European Microbiological Societies. All rights reserved SSDI 0928-8244(95)00043-7 18 J, Podwibka et al. / FEMS Immunology and Medical Microbiology production is also markedly decreased [ 10,l l]. IL-2 is known to play a key role in development of various forms of cellular immunity by activation of T lymphocytes into cell division and differentiation into effector cells by means of receptor mediated IL-2 binding [ 121. Deficiencies in the synthesis of and/or response to IL-2 have been implicated in impaired cell-mediated immune reactions and immunity in some infectious diseases [13-161 for which efficient cell-mediated immunity is very important for host resistance. The aim of the present study was to investigate if human lymphocytes are able to produce this interleukin at different stages of syphilis, in both the mild and acute course of disease. In addition, the association between production and ability to absorb IL-2, by serum IL-2 inhibitor or serum soluble interleukin 2 receptor (sIL-2R), was examined. As far as we know, no reports have been published on IL-2 production by PBMC of syphilitic patients and no information is available on serum IL-2 inhibitor and soluble serum IL-2R in this disease. 2. Materials and methods 2.1. Cell separation and culture medium The PBMC were separated from heparinized blood of 55 patients with different stages of syphilis, and 12 (I 995) 17-28 from 32 healthy people used as a control (Table 1). The cells were obtained by centrifugation of heparinized blood on a Ficol (Pharmacia, Uppsala, Sweden) Uropoline (Polfa, Poland) density gradient. Uropoline was used instead of Hypaque M as originally recommended [171. They were washed and suspended in RPM1 1640 (Gibco, Grand Island, NY) supplemented with 2 mM glutamine, 0.1 mM sodium pyruvate, 100 IU ml-’ penicillin, 100 pg ml-’ streptomycin, 5 X 10m5 M 2ME, 15 mM Hepes and 10% foetal calf serum (FCS) at final concentration for interleukin stimulation and 2% for IL-2 determination. All reagents were from Gibco (Grand Island, NY). 2.2. Cell culture and IL-2 stimulation The peripheral blood mononuclear cells (PBMC) (density 1 X lo6 ml-‘) were cultured in flat-bottomed 96-well microtitre plates (Greiner). Cells from every patient were cultured in 36 wells (12 with ConA, 12 with PHA and 12 with medium without mitogen). Each well contained 100 11-1of cell suspension, 100 ~1 ConA at final concentration of 7.8 pg ml-‘, and PHA at concentration 10 +g ml-’ as determined from titration or 100 ~1 medium. Cells were incubated for 24 and 48 h at 37°C in a humidified atmosphere containing 5% CO,. Cells cultured only in culture medium were used as non-stimulated controls. At the end of incubation, culture supernates Table 1 Patients examined with different stages of syphilis Stages of syphilis Shortening No. of patients Women Men Primary seronegative syphilis Primary seropositive syphilis Secondary early syphilis Secondary relapse of syphilis Early latent syphilis Late latent syphilis Malignant syphilis Asymptomatic neurosyphilis Paralysis progressive Cerebrospinahs syphilis Tabes dorsalis prim. seroneg. syph. prim. seropos. syph. second. early syph. second. tel. syph. early lat. syph. late lat. syph. malignant syph. asympt. neurosyph. paralysis progr. cembrospin. syph. tabes dors. 3 2 5 I 7 I 1 15 3 4 3 I 0 I 3 2 3 3 0 9 0 2 0 TOTAL 55 23 32 Control group 32 13 19 1 2 5 4 4 I 6 3 2 I J. Podwiriska et al. / FEMS Immunology were collected and stored frozen at - 70°C until they were tested. 2.3. IL-2 determination IL-2 activity in culture supemates was measured using ’ H-thymidine incorporation by the IL-2 dependent CTLL-2 cell line (kindly provided by M. Zimecki), as described by Gillis et al. [18]. Briefly, CTLL-2 cells cultured in RPMI 1640 medium (supplemented as medium for PBMC, see above) with addition of 20 IU ml-’ of highly purified human IL-2 (Biotest) were washed twice in RPM1 medium immediately before use to remove residual exogenous IL-2, and were adjusted to 1 X 10’ cells ml-‘. A volume of 100 ~1 of this suspension was distributed into each well of flat-bottomed microtitre plates which contained 100 ~1 of culture fluid, RPM1 or medium with a range of different concentrations of standard human IL-2 (Biotest). The cultures were incubated for 24 and 48 h at 37°C in a humidified environment containing 5% CO,. During the final 6 h of incubation, the cells were pulsed with 1 &i “H-thymidine in 20 ~1 PBS (Amersham, Arlington Heights, IL). The labelled cells were harvested using an automated Scatron harvester onto glass-fibre filter strips (Scatron). The fibre glass strips were air-dried for at least 4 h at 37°C. Individual discs were punched into 2.5 ml-plastic scintillation vials (Zorza, Poland) and 2 ml of scintillation fluid (consisting of 8 g POP (2,5-diphenyloxazole (Koch-Light Laboratories Ltd., UK) and 50 mg POPOP (1,4-di[2-(C5 phenyloxazolyll-benzene) (International Enzymes Ltd., UK) diluted in 1 1 of toluene (Poch, Poland) was added to each vial. Radioactivity was determined in a liquid scintillation counter ( p> model LS 3801 Beckman. All data are presented as means from triplicate cultures of the same tested samples. 2.4. Assay of serum IL-2 inhibitor The activity of the inhibitor in tested sera was measured by its ability to inhibit IL-2 mediated proliferation of a cytotoxic T lymphocyte line (CTLL-2) by the method of Emery et al. 1191 with slight modifications. A volume of 100 ~1 of this cell suspension, prepared as reported above, was added to each well of a microtitre plate (Greiner) containing 60 ~1 of RPM1 medium, 20 ~1 of tested serum and Medical Microbiology 12 I 199.5) 17-28 19 (10% final concentration) and 20 ~1 (20 IU> of highly purified human IL-2. Controls were: 20 ~1 of IL-2 and 80 ~1 of culture medium or medium without IL-2 (100 ~1). The cells were incubated for 24 h at 37°C in a humidified environment containing 5% CO,. During the final 6 h of incubation the cells were pulsed with 1 PCi ‘H-thymidine. The cells were harvested and examined as described above. The results were expressed as the percentage inhibition of IL-2 response in the presence of serum which was calculated as follows: cpm with serum % inhibition = I - cpm without serum x 100 2.5. Detection of serum-soluble IL-2 receptor (slL2R) Levels of sIL-2R in the serum of patients were determined using an ELISA test kit from T-cell Sciences (Cambridge, MA). Briefly, the sIL-2R available in the test samples or in the standards were bound to the polystyrene microtiter wells previously incubated with anti IL-2R monoclonal antibodies. With washing, non-reacting sample components were removed. A horseradish peroxidase conjugated antiIL-2R mAb directed against a second epitope on the IL-2R molecule, was bound to the IL-2R captured by the first antibody to complete the sandwich. After washing, substrate solution was added to the wells. The coioured product of the enzyme reaction was formed in proportion to the amount of sIL-2R present in the sample. The reaction was then stopped and the absorbance determined at 490 nm. The IL-2 receptor concentration was determined from the standard curve prepared from 5 IL-2 receptor standards. The IL-2R standard was the cell-free supernatant obtained from PHA in vitro stimulated T cells, which was assigned as a value of 1000 IL-2R U/ml. When the values were above their standard curve, samples were retested after dilution and results expressed accordingly. The final values were expressed as units per ml (U ml-‘). 2.6. Ability of CTLL-2 cells to proliferate Before using CTLL-2 cell line in experiments, its ability to proliferate in the presence of standard IL-2 20 J. Podwihsko et al. / FEMS Immunology and Medical Microbiology was examined. The IL-2 was used at concentrations from 1 to 256 U ml -I. The prepared standard curve indicated the sensitivity of cells and could be used to determine units of IL-2 designated as indicated in the previous paper [I 11. Only strongly proliferating cells were used in all experiments. 12 (1995) 17-28 (Becton Dickinson). Analysis was done using the computer program BDIS CONSORT 30-Ver F. Each time 15 000 cells were counted. Only Becton Dickinson reagents were used and the manufacturer’s instruction were followed. As a control, Simultest (IgG FITC/IgG, PE) was used. 2.7. Absorbtion of adherent ceils The monocytes were removed from a suspension of PBMC by adhering the cells to the Petri dishes during 2 h of incubation at 37°C in a humidified atmosphere containing 5% CO,. The venereal disease research (VDRL) slide flocculation test 2.8. l 2oo.ooo 180.000 laboratory = p<o.I ** = P<O.Ol n-l *** = P<O.O5 -. 160,000 This test was performed as described in the Manual of Tests for Syphilis [20]. 2.9. Treponema pallidurn haemagglutination 140.000 test 120.000 (TPHA) This test was performed according to Tomizawa using reagents of Cellognost-Syphilis H, (Behring, Germany). ; 100,000 et al. [2l], 2. IO. Captia 80.000 syphilis-M immunoenzymatic test 60.000 This test was performed using Mercia Diagnostics reagents as described by Gibowski and Machoriko [221. 2.1 I. Fluorescent treponemal antibody absorbtion 40.000 20.000 test (FTA-ABS) This test was performed according to the method of Hunter et al. [23]. 2.12. Lymphocyte markers The cell surface markers were analyzed using monoclonal antibodies against CD, (anti-Leu-3 FITC), Simultest: CD, (anti-Leu-4 FIX), CDs (antiLeu-8 PE and CD25 (IL-2R)) (Be&on Dickinson). To 100 ~1 of cell suspension 10 yl specific antibodies were added. The mixture was incubated 20-30 min at 4°C and the cells were counted by FACSCAN Fig. 1. IL-2 production by PBMC during the course of infection. PBMC were isolated from both normal and syphilitic people with different stages of disease and were stimulated in culture with a dose 7.8 pg ml-’ of ConA for 24 h. The culture supemates were assayed for IL-2 content using an IL-2 dependent CTLL-2 cell line. The results are expressed as the average f S.D. of cpm of triplicate cultures (m, average; 0, SD.). 0 = values for PBMC Controls. .I. Podwihka et al./ FEMS Immunology and Medical Microbiology 12 (1995) 17-28 2.13. Statistics 21 highest level of IL-2 was found in culture supernates of lymphocytes stimulated with ConA and PHA (not demonstrated) in primary seropositive syphilis. In subsequent stages of the disease, the level of IL-2 was decreased and the lowest was in lymphocyte supemates of patients with malignant syphilis and tabes dorsalis (difference not statistically significant) and in asymptomatic neurosyphilis, paralysis progressive and cerebrospinal syphilis (difference statistically significant). Nearly the same level of IL-2 was found when the cells were incubated for 48 h (data not presented). In culture supemates of nonstimulated lymphocytes the level of IL-2 was low (from 2000-5000 cpm) when standard IL-2 at a concentration of 20 U ml-’ was used as a control, to check ability of CTLL-2 cells to proliferate, the level was from 140000-160000 cpm (not indicated in Figs.). All experiments were carried out in triplicate; results were expressed as the mean f SD. Comparison between tests was done by Student’s t-test, with statistical significance considered to be P < 0.05 and nonparametric for comparison of two independent median Wilcoxon sum rank tests [24]. 3. Results 3. I. IL-2 production by PBMC stimulated with ConA and PHA PBMC from patients with different stages of syphilis (Table 1) as diagnosed on the basis of serological tests: (VDRL [20], TPHAT 1211, Captia Syphilis-M [22] and PTA-ABS [23]), and clinical examination were tested for IL-2 production; results are shown in Fig. 1. In comparison with cells from normal people, the 3.2. Suppression of IL-2 production by adherent cells Taking into account sent in cell suspensions the fact that monocytes premay produce prostaglandins _ 250,000 / * = PCO.05 200,000 150,000 E !? 100,000 50,000 0 ImPHA 24h +M DPHA 24h-M konA24h+M HConA24h-M 6PHA48h+M n PHA48h-M 1 Fig. 2. Ability of PBMC to produce IL-2 before and after absorption of adherent cells (Man) and stimulation with ConA and PHA for 24 and 48 h. 22 J. Padwihku et al./ FEM.7 Immunology and Medical Microbiology 12 (1995) 17-28 I 12ooo 22o.ooQ loom ea,ooo Bwo B wo.ooo 0000 4000 Bo.000 2000 0 0 Fig. 3. Ability cells for IL-2 production and titer of antibodies in sera, measured using the FTA-ABS test. which inhibit IL-2 production [25] we absorbed adherent cells from PBMC, and lymphocytes were examined for their ability to produce IL-2 (Fig. 2). As can be seen from Fig. 2, the culture supernates from PBMC deprived of monocytes had higher levels of IL-2. The highest level seems to be in those stages of syphilis where the ability of the cells for IL-2 production was the lowest as in secondary malignant syphilis and late stages of neurosyphilis. In early stages, primary seronegative and seropositive syphilis, this ability slightly increased and in the control it was virtually unchanged. 20 2B iBo,ooo 20 z % lOO.OW II 10 Pig. 4. IL-2 production by PBMC and level of IL-2 inhibitor in sera. The results am expressed as the average of cpm for IL-2 and percentage of inhibition for serum IL-2 inhibitor. J. Podwihska et al. / FEMS Immunology and Medical Microbiology ~60.066 I2 (1995) 17-28 23 666 Q 666 1w.006 Fig. 5. lL-2 production and level of slL2-R in sera. The results are expressed as the average of cpm for IL-2 and IU ml- ’ for sIL-2R 3.3. IL-2 production and level of antibodies The ability to produce IL-2 did not correlate with the titer of antibodies in sera of patients (Fig. 3). Fig. 3 demonstrates only the level of antibodies measured by FTA-ABS [23]. Similar results were obtained when the level of antibodies was examined by VDRL [20], TPHA [21] and Captia Syphilis-M [22] (data not presented). The highest level of anti- bodies was in malignant syphilis and tabes dorsalis where the ability to produce IL-2 was the weakest. 3.4. IL-2 inhibitor activity Taking into consideration that, in sera from patients with a suppressed cell-mediated immune response an inhibitor of IL-2 is present 1261 and that this factor may take part in a mechanism of home- Table 2 Proportion of lymphocytes with markers CD,, CD, aad CDs at different stages of syphilis Stages of syphilis Percentage of lymphocytes with markers: CD, C”3 Control group Primary seronegative syphilis Primary seropositive syphilis Secondary early syphilis Secondary relapse of syphilis Early latent syphilis Late latent syphilis Mahgnant syphilis Asymptomatic neurosyphilis Paralysis progressive Cembrospinalis syphilis Tabes dorsalis 69.88 f 74.40 f 81.95 f 72.26 f 72.44 f 72.63 f 76.87 f 50.60 74.90 f 54.37 f 68.48 f 68.80 8.38 4.04 7.42 13.65 6.09 8.42 4.60 8.74 2.85 13.48 45.72 f 52.50 f 53.80 * 47.04 * 51.00* 54.53 f 50.39 f 28.70 42.45 * 39.63 f 40.68 f 44.40 C”, 10.05 4.08 9.19 12.18 11.76 8.86 14.80 11.88 1.25 12.49 25.05 f 24.87 f 21.65 f 28.30 f 22.63 f 20.21 f 20.79 f 39.10 31.56 f 26.03 f 3 1.58 f 26.40 6. I8 1.53 12.66 6.23 4.47 5.57 7.9 1 11.78 14.06 7.62 24 i. Podwiriska et al./ FEMS Immunology and Medical Microbiology I2 (1995) 17-28 ostasis, the following questions arise: (1) what is the level of this factor in sera of patients with different stages of syphilis; and (2) does any correlation exist between the serum level of this inhibitor and ability of cells to produce IL-2? In all sera of normal people and syphilitic patients an IL-2 inhibitor was present. The highest level of this factor in comparison to the control was found in sera of patients with early and late latent syphilis where no clinical symptoms of disease were present. In other stages of syphilis the level of IL-2 inhibitor was maintained with slight fluctuation as in the control group. A comparison of PBMC ability to produce IL-2 with the level of IL-2 inhibitor in sera is shown in Fig. 4. Only at the beginning of the disease (primary seropositive syphilis) was the ability to produce IL-2 correlated with an increased level of inhibitor, and in * = PCO.1 ** = Pa01 *** = P<O.O5 secondary early syphilis both IL-2 production and level of inhibitor were decreased. In other stages of the disease a high level of inhibitor was accompanied with decreased ability to produce IL-2. 3.5. Soluble serum IL-2 receptor Other factors which may also be bound to IL-2 and inhibit its activity are soluble serum IL-2 receptors &IL-2R). In all stages of syphilis the level of sIL-2R was higher than in the control group and primary seronegative syphilis. The highest level was in malignant syphilis paralysis progressive and tabes dorsalis where PBMC had a very weak ability to produce IL-2 (Fig. 5). 3.6. Lymphocyte receptor for IL-2 It was interesting to examine the percentage of lymphocytes T and B with receptors for IL-2 in different stages of syphilis and their different ability to produce IL-2. Independently of the stage of syphilis and ability to produce IL-2, the percentage of cells with IL-2 receptors was distinctly higher than in the control group (not indicated). 3.7. Markers of T lymphocytes Fig. 6. Ability of PBMC to proliferate in the presence of 20 IU of standard IL-2. The rcaults arc expressed as average f SD. of cpm of triplicate cell cultures (m. average; 0, S.D.). The suppression of IL-2 production may be also connected with the diminished proportion of CD, and CDs lymphocytes in circulation. The percentage of cells with these markers as well as CD, in different stages of syphilis is demonstrated in Table 2. As seen in Table 2 a diminished percentage of lymphocytes CD, and CD, was only observed in syphilis with a severe course of the disease and distinctly diminished ability to produce IL-Z as in malignant syphilis ( P < 0.1) and paralysis progressive (P < 0.01). On the contrary, a diminished percentage of ceDs with the CDs marker was seen in early (P < 0.01) and late latent syphilis (P < 0.11, where no clinical symptoms of the disease were present and only a weakly diminished ability of PBMC to produce IL-2 was found. J. Podwikka et al. / FEMS Immunology 3.8. Cell proliferation in the presence of exogenous IL-2 The proliferation ability of lymphocytes in the presence of IL-2 (20 IU) is shown in Fig. 6. The greatest capacity for proliferation was seen in cells from patients with primary seropositive syphilis. In secondary early syphilis this ability distinctly decreased but in the next stages (secondary relapse of syphilis, early and late latent syphilis and asymptomatic neurosyphilis) it was partially restored. In all stages of symptomatic neurosyphilis as well as in malignant syphilis the ability to proliferate in the presence of exogenous IL-2 was very low (about one third of that in the control). 4. Discussion The results of the present study have demonstrated that the ability of PBMC of syphilitic patients to produce IL-2 develops from the start of the disease. The highest level of this cytokine was seen in primary seropositive syphilis. At this stage of the disease, lymphocytes also had the greatest ability to produce migration inhibition factor. In the light of these data, production of both factors (IL-2 and MIF) at the same time of disease, seems to indicate that IL-2 may stimulate a cell-mediated immune response and in this way contribute to protection against Treponema pallidum infection. In subsequent stages of syphilis this ability for IL-2 production was distinctly decreased and fell to a lower value than that in normal human lymphocytes, at which it was maintained throughout all later stages of the disease. The lowest level was found in supernates of cells from patients with malignant syphilis and tabes dorsalis, i.e. in severe stages of the disease. The data seem to suggest that decreased ability for IL-2 production may be an effective cause of increasing progression of the disease. The present study has also indicated that absorption of adherent cells from PBMC increased their ability to produce IL-2. These results are in agreement with those of Tomai et al. [lo] who additionally indicated 1251 that adherent cells stimulated with T. pallidum antigen produce PGE, which is generally considered to be an inhibitory factor [27]. It was also and Medical Microbiology 12 f 1995) 17-28 25 interesting to notice that, after absorption of adherent cells, the level of IL-2 in culture supemates was higher at those stages of syphilis where deepest suppression was observed. In the control group the ability of cells to produce IL-2 was almost unchanged. This seems to indicate that suppression of IL-2 production may be connected with stimulation of adherent cells in vivo by T. pallidum. Suppression of IL-2 production has no influence on the level of antibodies in sera which seems to suggest that lack of this interleukin did not disrupt stimulation of the humoral immune response. The production and biological activity of IL-2 is under complex control by cellular and humoral factors known as IL-2 inhibitor present in serum and other biological fluids [26]. It is believed that serum inhibitor acts in a homeostatic mechanism to restrict IL-2 action of the activated T lymphocytes. In the presence of this inhibitor, decreased IL-2 production and response to exogenous IL-2 was found in autoimmune disease [19,28,29] and in infectious disease associated with immunological defects, such as lepromatous leprosy [30] or acquired immunodeficiency syndrome (AIDS) [3 1,321. In the present study all sera of normal people and syphilitic patients contained IL-2 inhibitor, but the highest level of this factor was in sera of patients with early and late latent syphilis where no symptoms of the disease were present. On the other hand, in secondary early syphilis, malignant and cerebrospinalis syphilis with pathologic symptoms of the disease, the level of IL-2 inhibitor was very low. The data seem to suggest that IL-2 inhibitor may moderate the manifestations of Treponema pallidum infection. There are some suggestions that depression of IL-2 inhibitor is associated with a severe course of the disease and a poor prognosis, whereas a high level of inhibitor is associated with good prognosis in systemic lupus erythromatosis (SLE) [29] and in rheumatoid arthritis [19]. The mechanism of IL-2 inhibition is as yet unclear. Honda et al. [33] suggested that IL-2 inhibitor could be bound to IL-2 or to IL-2 receptor competing with IL-2 attachment. Cells examined in our experiments for the presence of receptors for IL-2 indicated that independently of the stage of syphilis and level of inhibitor in circulation, the percentage of cells with receptors for IL-2 was distinctly higher than that in the control. On the 26 .J. Podwiriska et al. / FEMS Immunology and Medical Microbiology I2 (1995) 17-28 other hand, the ability to proliferation in the presence of exogenous IL-2 was the same as the ability of cells to produce this interleukin. These results are difficult to explain. Also, the above data indicate that in sera of all patients the level of soluble IL-2 receptors (sIL-2R) was high. The highest level was in sera of patients whose PBMC had weak ability to produce IL-2 as in malignant syphilis and paralysis progressive. An elevated level of sIL-2R has been found also in sera of patients with autoimmune disease as well as in culture supemates of PBMC of the same patients [34]. Though we have not examined sIL-2R in culture supemates, nevertheless they may be present there and may bind IL-2 and in this way inhibit IL-2 activity. This question will be examined in the future. Phenotypic analysis of PBMC indicated that a severe course of syphilis and weakening ability to produce IL-2 is accompanied by a diminished percentage of CD, and CD, lymphocytes and increased percentage of CD,. On the other hand, in syphilis without clinical symptoms of the disease as in early and late latent syphilis, the percentage of CD,, cells was higher than CD,. The diminished percentage of CD, cells and decreased ability for IL-2 production or inhibition of its activity may lead to a decrease of the cell-mediated immune response and resistance against Treponema pallidum infection. References Podwibska, J. (1993) The role of humoral and cell-mediated immunity in protection against Treponemo pallidurn. Arch. Immunol. Ther. Exp. 41, 281-284. 121Metzger, M., Podwitiska, J. and Smog&, W. (1977) Cellmediated immunity in experimental syphilis in rabbits. Arch. Immunol. Ther. Exp. 25, 25-34. [31 Baughn, R.E. (1983) Immunotegulatoty effect in experimental syphilis. In: Pathogenesis and Immunology of Treponemal Infection &hell, R.F. and Musher, D.M., Eds.),pp. 271-295. Marcel Dekker Inc., New York. [41 Nathan, C.F., Remold, H.G. and David, J.R. (1973) Characterization of a lymphocyte factor which alters macrophage functions. J. Exp. Med. 137, 275-290. El Podwifiska, J. (1991) Circulating immune complexes in experimentrrl syphilis and their relation to immunological response against Treponema pallidum. FEMS Microbial. Immunol. 76, 83-92. bl Podwihska, J. and Chomik, M. (1992) Treponemicidal activity of anti-treponemal Iymphotoxins and their relation to circulating immune complexes and autolymphocytotoxins. FEMS Microbial. Immunol. 89, 345-352. [7] Podwibska, J. and Metzger, M. (1981) Treponemicidal activity of supematants from cultures of sensitized lymphocytes. Arch. lmmunol. Ther. Exp. 29, 671-677. [8] Fitzgerlad, T.J. and Elmquist, B.J. (1990) Soluble factors from rabbit spleen cells kill and lyse Treponema pallidum in vitro. Can. J. Microbial. 36, 71 I-717. [9] Podwihska. J. (1987) Identification of cells producing antitreponemal lymphotoxins (ATL). Arch. Immunol. Ther. Exp. 35,63-70. [IO] Tomai, MA.. Elmquist, B.J., Warn&a, S.M. and Fitzgerald, T.J. (1989) Macrophage-mediated suppression of ConA induced IL-2 production in spleen cells from syphilitic rabbits. J. lmmunol. 143, 309-314. [ 1I] Podwitiska, J., &ba, R., Chomik, M. and Bowszyc, J. (I 993) The ability of peripheral blood mononuclear cells of rabbits infected with Treponema pallidurn to produce IL-2. FEMS Immunol. Med. Microbial. 7, 257-264. [12] Smith, K.A. (1988) Interleukin-2; inception, impact and implications. Science 240, 1169- I 176. [I31 Collizzi, V. (1984) In vivo and in vitro administration of interleukin-2 containing preparation reverses T cell unresponsiveness in Mycobacferium bouis BCG-infected mice. Infect. lmmun. 45.25-28. [14] Collizzi, V. and Malkovsky, M. (1985) Augmentation of IL-2 production and delayed hypersensitivity in mice infected with Mycobacferium bouis and fed a diet supplemented with vitamin A acetate. Infect. Immun. 48, 581-593. [15] Leiva, L.E. and Lammie, P.J. (1989) Regulation of parasite antigen-induced T cell growth factor activity and proliferative responsiveness in Burgia pa/urn@-infected birds. J. Immunol. 142, 1304-1309. [16] Jamashita, T. and Boros, D.L. (1990) Changing patterns of lymphocyte proliferation, IL-2 production and utilization and IL-2 receptor expression in mice infected with Schisfosoma mansoni. J. Immunol. 145, 724-731. [I71 Tellez, A. and Rubinstein, P. (1970) Rapid method for separation of blood cells. Transfusion 10, 223-225. 1181Gillis, S.A., Ferm, A.M., Ou, W. and Smith, K.A. (1978) T cell growth factor; parameters of production and quantitative micro-assay for interleukin-2 activity. J. lmmunol. 120, 2027-2032. (191 Emery, P., Gentry, K.C., Kelso, A. and Mackay, I.R. (1988) Interleukin-2 inhibitor in synovial fluid. Clin. Exp. lmmunol. 72,60-66. [20] U.S. VenereaI Disease Research Laboratory. Manual of Tests for Syphilis (1969) Public Health Service Publication No 441, US Govt. Print. Office, Washington. ]21] Tomizawa, T., Kasamatsu, S. and Jamaya, S. (1969) Usefulness of the hemagglutination test using Treponema pallidurn antigen (TPHA) for the serodiagnosis of syphilis. Jap. J. Med. Sci. Biol. 22, 341-350. ]22] Gibowski, M., Machonko, T. (1990) Captia Syphilis-M test in serum of patients with early and late syphilis. Postepy Dermatologii 7, 363-372. ]23] Hunter, E.F., Deacon, W.E. and Meyer, P.E. (1964) An J. Podwiriska et al. / FEMS Immunology improved FTA test for syphilis, the absorption procedure (FTA-ABS). Public Hlth. Rep. 79, 410-412. [24] Daly, E.L.. Bourke, J.G. and McGilvary, J. (1992) Interpretation and uses of medical statistics. Blackwell Scientific Publications, London. [25] Fitzgerald, T.J., Tomai, M.A., Trachte, G.J. and Rice, T. ( I99 11 Prostaglandins in experimental syphilis: Tteuonemes _. stimulate adherent spleen cells to secrete prostaglandin E, and indomethacin upregulates immune functions. Infect. Immun. 59, 143-149. [261Kucharz. E.J. and Goodwin, S. (1988) Serum inhibitors of interleukin-2. Life Sci. 42, 148.5-1491. 1271Goodwin, J.S. and Webb, D.R. (19801 Regulation of the immune response by prostaglandins. Clin. Immunol. Immunopathol. 15, 106 122. 1281Fakushima, T., Kobayashi, K., Kasama, T., Kasahara, K., Tabata, M., Sekine, F., Negishi, M.. Ide, H. and Takahashi, T. (1987) Inhibition of interleukin-2 by serum in healthy individuals and in patients with autoimmune disease. Int. Arch. Allergy Appl. Immun. 84, 135-141. I291 Kucharz, E.J., Sierakowski, S. and Goodwin, J.S. (1987) Decreased activity of interleukin-2 inhibitor in plasma of patients with systemic lupus erythematosus. Clin. Rheumatol. 6, 87-90. and Medical Microbiology 12 (I 995) 17-28 21 N., Gelber, R.H., Larrick, J.W., Sasaki, 1301Mohagheghpour, D.T., Brennan, P.J. and Engelman, E.G. (1985) Defective cell-mediated immunity in leprosy: failure of T cells from lepromatous leprosy patients to respond to Mycobucterium leprae is associated with defective expression of interleukin-2 receptors and is not reconstituted by interleukin-2. J. lmmunol. 135, 1443-1449. t311Farmer, J.L., Gottlieb. A.A. and Nishihara, T. (1986) lnhibition of interleukin-2 production and expression of interleukin-2 receptor by plasma from acquired immune deliciency syndrome patients. Clin. Immunol. Immunopathol. 38, 235-243. [321Gupta, S., Gillis, S.. Thornton, M. and Goldberg, M. (1984) Autologous mixed lymphocyte reaction in man. XIV. Deliciency of the autologous mixed lymphocyte reaction in acquired immune deficiency syndrome (AIDS) and AIDS related complex (ARC): in vitro effect of purified interleukin-2 and interleukin-2. Clin. Exp. Immunol. 58, 395-40 I. 1331Honda, M., Ghan, C. and Shevach, E.M. (1985) Characterization and partial purification of a specific interleukin-2 inhibitor. J. lmmunol. 135, 1834- 1839. [341Cavallo, M.G., Pozzilli, P. and Thorpe R. (19941 Cytokines and autoimmunity. Clin. Exp. Immunol. 96, l-7.