Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
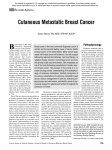
C as e R epo rt A bs tra ct Anterior abdominal wall cutaneous metastases detected by F-18 fluorodeoxyglucose-positron emission tomography/computed tomography in a patient with breast carcinoma Cutaneous metastases from internal malignancies are rare with a reported incidence between 0.7% and 10%. It may be the first symptom in 7% of the patients with cancer. We report a case with distant solitary skin metastases in anterior abdominal skin from breast cancer detected on F‑fluorodeoxyglucose‑positron emission tomography/computed tomography imaging. Key words: Breast cancer, F-18 fluorodeoxyglucose-positron emission tomography/ computed tomography, skin metastases, staging Koramadai Karuppusamy Kamaleshwaran, Sudhakar Natarajan1, Anjali Malaikkal, Vyshakh Mohanan, Ajit Sugunan Shinto Departments of Nuclear Medicine and PET/CT and 1Oncology, Comprehensive Cancer Care Centre, Kovai Medical Centre and Hospital Limited, Coimbatore, Tamil Nadu, India Address for the Correspondence: Dr. Koramadai Karuppusamy Kamaleshwaran, Department of Nuclear Medicine, PET/CT and Radionuclide Therapy, Comprehensive Cancer Care Centre, Kovai Medical Centre and Hospital Limited, Coimbatore ‑ 641 014, Tamil Nadu, India. E‑mail: [email protected] Access this article online Website: www.oghr.org DOI: 10.4103/2348-3113.139658 Quick response code: INTRODUCTION Cutaneous metastases from internal malignancies are rare with a reported incidence between 0.7% and 10%.[1] Although the most common carcinoma to metastasize to the skin is malignant melanoma, seconded by breast carcinoma, breast cancer is very common in females and cutaneous metastasis of breast cancer is the commonly encountered metastasis in clinical practice.[2,3] We report a case of distant solitary skin metastases over the anterior abdominal skin from breast cancer, detected on an F‑18 fluorodeoxyglucose‑positron emission tomography/computed tomography (F‑18 FDG‑ PET/CT) scan. In addition to the detection of skin metastases, F‑18 FDG‑PET/CT was also useful in staging the disease. CASE REPORT A 45‑year‑old woman diagnosed to have left‑sided breast carcinoma was subjected to F‑18 FDG‑PET/CT [Figure 1a] scan to stage the disease. Intense uptake is noted in the soft tissue lesion in the left breast and axillary nodes along with FDG avid sclerotic lesion was also noted in the sternum [Figure 1b]. There was a FDG avid hypodense liver lesion noted in segment I [Figure 1c]. Intense FDG avid skin thickening [standardized uptake value [(SUV) =15] was noted over right lower abdominal wall [Figure 1d]. Hence, in addition to demonstration of primary breast, bone and liver metastasis, F‑18 FDG‑PET/CT also revealed unsuspected skin lesion. Clinical examination revealed a skin lesion in the right abdominal wall. Subsequently, the patient underwent neoadjuvant chemotherapy. DISCUSSION Differential diagnosis of the skin lesions and subcutaneous nodules would include cutaneous lymphoma, melanoma, neurofibromatosis, and metastases from other internal malignancies.[1] The breast, stomach, lung, uterus, large intestine, and kidneys are the most frequent internal organs to produce cutaneous metastases. Cancers that have the highest propensity to metastasize to the skin include melanoma (45% of cutaneous metastasis cases), breast (30%), nasal sinuses (20%), larynx (16%), and oral cavity (12%).[2] Because breast cancer is so common, cutaneous metastasis of breast cancer is the most frequently encountered type of cutaneous metastasis in most clinical Oncology, Gastroenterology and Hepatology Reports| Jan-Jun 2015 | Vol 4 | Issue 1 64 Kamaleshwaran, et al.: Cutaneous metastasis from breast cancer detected by FDG PET/CT cutaneous metastases may be the presenting symptom it usually represents advanced disease and poor prognosis. FDG PET‑CT can potentially be used as a one‑stop‑shop imaging modality in patients with cutaneous/subcutaneous metastases from FDG avid primary malignancies. FDG PET‑CT may also find a role in evaluating the response of these lesions to treatment. In our case, in addition to demonstration of FDG uptake in skin metastases, PET/CT also revealed liver and sternal metastases, thereby defining true extent of the disease. Our case also highlights the fact that F‑FDG avid nodules in skin in a case of breast carcinoma should always bring up suspicion of skin metastases. b c REFERENCES a d 1. Figure 1: Whole body fluorodeoxyglucose‑positron emission tomography/computed tomography (FDG PET/CT) maximum intensity projection images (a). Axial fused PET/CT showing primary left breast mass and sternal lesion (b) (arrows). Hypodense mass in the liver (c) (arrows), and intense FDG uptake with a standardized uptake value max of 15 in the anterior abdominal wall skin lesion on the right side (d) (arrows) practices.[3] Cutaneous metastases can occur either by lymphatic or hematogenic spread and is most commonly seen in the head and neck regions and trunk.[4] The recognition of cutaneous metastases often dramatically alters therapeutic plans, especially when metastases signify persistence of cancer originally thought to be cured. Some tumors metastasize with predilection to specific areas. Recognition of these patterns can be useful in directing the search for an underlying tumor. F‑18 FDG–PET/CT has been widely used in staging breast cancer and shown to be better than conventional imaging modalities and also changes management in significant number of patients.[5] However, distant skin metastases from breast cancer detected by FDG‑PET/CT have been rarely reported in the literature.[6,7] Though 65 2. 3. 4. 5. 6. 7. Lookingbill DP, Spangler N, Helm KF. Cutaneous metastases in patients with metastatic carcinoma: A retrospective study of 4020 patients. J Am Acad Dermatol 1993;29:228‑36. Brenner S, Tamir E, Maharshak N, Shapira J. Cutaneous manifestations of internal malignancies. Clin Dermatol 2001;19:290‑7. Krathen RA, Orengo IF, Rosen T. Cutaneous metastasis: A meta‑analysis of data. South Med J 2003;96:164‑7. Lookingbill DP, Spangler N, Sexton FM. Skin involvement as the presenting sign of internal carcinoma. A retrospective study of 7316 cancer patients. J Am Acad Dermatol 1990;22:19‑26. Eubank WB, Mankoff D, Bhattacharya M, Gralow J, Linden H, Ellis G, et al. Impact of FDG PET on defining the extent of disease and on the treatment of patients with recurrent or metastatic breast cancer. AJR Am J Roentgenol 2004;183:479‑86. Manohar K, Mittal BR, Bhattacharya A, Singh G. Asymptomatic Distant subcutaneous metastases detected by (18) F‑FDG‑PET/CT in a patient with breast carcinoma. World J Nucl Med 2012;11:24‑5. Harisankar CN. Widespread subcutaneous metastases in a patient with breast cancer: Evaluation with fluoro deoxy‑glucose positron emission tomography‑computed tomography. Indian J Nucl Med 2013;28:190‑1. How to cite this article: Kamaleshwaran KK, Natarajan S, Malaikkal A, Mohanan V, Shinto AS. Anterior abdominal wall cutaneous metastases detected by F-18 fluorodeoxyglucosepositron emission tomography/computed tomography in a patient with breast carcinoma. Onc Gas Hep Rep 2015;4:64-5. Source of Support: Nil, Conflict of Interest: None declared. Oncology, Gastroenterology and Hepatology Reports| Jan-Jun 2015 | Vol 4 | Issue 1