Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
MONITORING DRUG THERAPY
LAKSHMAN KARALLIEDDE
OCTOBER 2011
Drug Therapy Monitoring Definition
Drug therapy monitoring, also known as Therapeutic Drug Monitoring (TDM),
is a means of monitoring drug levels in the blood.
Purpose
TDM is employed to measure blood drug levels so that the most effective
dosage can be determined, with toxicity prevented. TDM is also utilized to
identify noncompliant patients (those patients who, for whatever reason,
either cannot or will not comply with drug dosages as prescribed by the
physician).
Precautions
Because so many different factors influence blood drug levels, the following
points should be taken into consideration during TDM: the age and weight of
the patient; the route of administration of the drug; the drug's absorption
rate, excretion rate, delivery rate, and dosage; other medications the patient
is taking; other diseases the patient has; the patient's compliance regarding
the drug treatment regimen; and the laboratory methods used to test for the
drug.
REASONS FOR MONITORING DRUG TREATMENT
1.TO SEE WHETHER THERE IS A THERAPEUTIC RESPONSE
2.TO ASSESS DRUG TOXICITY
3.TO ASSESS COMPLIANCE
Examples
of
easily
measurable
therapeutic responses
•Urine output in patients treated with
desmopressin for
diabetes insipidus
•Intraocular Pressure in patients treated
with timolol eye drops
for glaucoma
• Muscle fatigue in patients treated with
pyridostigmine for myasthenia gravis
Monitoring drug treatment
1. Want our treatments to work
2. Do not wish treatments to cause harm.
Monitoring drug treatment is one way of seeing that a
treatment works, while protecting the patient from adverse
drug effects.
For many patients and many treatments clinical evaluation is
sufficient (e.g. Measuring blood pressure in a patient on
antihypertensive treatment).
When therapeutic goals cannot always be directly observed,
monitoring may require blood tests to determine whether
therapeutic levels have been reached.e.g the measurement of
the international normalised ratio (INR) in patients treated with
warfarin. Ensure that the therapeutic goal (prevention of
thrombosis is met)measuring INR helps to avoid the risk of
haemorrhage, which rises steeply as the INR increases above
2.0.
Monitoring drug treatment
Monitoring treatment to anticipate or detect adverse reactions to drugs before they
become inevitable or irreversible is very important.
For a monitoring test for an adverse drug reaction to be useful clinically, it should
satisfy criteria put forward for screening tests.
e.g. monitoring in patients treated with clozapine (atypical antipsychotic associated
with agranulocytosis in 0.8% of patients).
All patients taking clozapine have white cell counts performed weekly for the first 18
weeks of treatment and less often thereafter.
Clear criteria exist for when the drug should be withdrawn and patients continue
treatment only if the white cell count is satisfactory.
This has reduced the incidence of clozapine induced agranulocytosis and prevented
deaths from a serious adverse reaction.
Success is largely the result of
a. frequent monitoring at the time when the risk of agranulocytosis is highest
b. clear guidelines for action if results are abnormal.
The adverse reaction evolves slowly enough for once weekly monitoring to be
effective. By contrast serious hyperkalaemia could occur at any time in patients
treated for heart failure with spironolactone plus an angiotensin converting enzyme
inhibitor and evolve rapidly to cause lethal arrhythmia. Thus annual measurement
would be of little help in avoiding serious effects
Factors to take into account when monitoring for an adverse drug effect
The adverse effect
The effect should be potentially serious
The relation between the latent and overt effects should be known
The monitoring test
The test should be safe, simple, precise, and validated
The distribution of test values in the exposed population should be known and suitable cut-off values
established
The test should be acceptable to treated patients
A strategy in the face of a positive monitoring test should be agreed
The response to positive tests
An effective intervention should exist
This early intervention should make the outcome better than it would have been with delayed
intervention
Evidence for the intervention should be robust
The monitoring strategy
The strategy should reduce morbidity or mortality from the adverse effect
The strategy should be acceptable to patients and professionals
Benefits of monitoring should outweigh the physical and psychological harm
The cost of monitoring should be proportionate
A system for assuring the standards of the monitoring programme should exist
Possibility of reducing or removing risks of adverse effects by selection of drug or dosage, or by
pretreatment detection of susceptible people, should have been fully explored
DIFFICULTIES/PROBLEMS
1. Detection of drug induced liver injury. Statins can increase serum activity of
transaminase in about 3% of patients and rarely can lead to symptomatic hepatic
damage. This has prompted recommendations for monitoring. However, guidelines for
different statins differ both in recommended frequency of monitoring and advice on
the action to take if hepatic abnormalities are detected.
2. Little is understood about the relationship between mild abnormalities of liver
function and symptomatic liver injury, since liver function may improve even with
continued treatment with statin
3. It is unclear if or when treatment should be stopped
4. Infrequent monitoring as currently recommended is likely to miss most patients who
develop the sudden idiosyncratic hepatic reactions.
Monitoring for liver damage from statins may anyway be unnecessary—a meta-analysis
examining 112 000 person years of exposure to pravastatin found the frequency of
abnormal liver function tests (1.4%) to be similar in statin and placebo arms and in the
heart protection study treatment with statins at high dose (40 mg simvastatin) seemed
safe.
When considered with evidence about muscle damage from statins, the findings imply
that these drugs can be used without any regular monitoring (conclusion of a
retrospective analysis of 1014 patients in primary care, where the occasional finding of
abnormal laboratory values rarely resulted in drug discontinuation).
A policy of non-monitoring would prevent unnecessary discontinuation of statins.
Product information on drugs often suggests monitoring of one kind or another but does
not specify the frequency of testing or the strategy to adopt if tests are positive, and
many of the proposed tests fail to satisfy the criteria listed.
There is a need for better evidence on which to base monitoring strategies.
Meanwhile, adverse reactions will often be prevented more effectively (and
economically) by educating prescribers and increasing patients' awareness than by
empirical blood test monitoring.
After all, rational therapeutics demands a more careful approach to drug treatment than
simple opportunistic measurement in the outpatient clinic.
BMJwww.bmj.com
BMJ 327 : 1179 doi: 10.1136/bmj.327.7425.1179 (Published 20
November 2003)
Editorial
Munir Pirmohamed, professor of clinical pharmacology
Robin E Ferner, clinical pharmacologist
TDM is a practical tool that can help the physician provide effective and safe drug therapy
in patients who need medication.
Monitoring can be used to confirm a blood drug concentration level that is above or
below the therapeutic range, or if the desired therapeutic effect of the drug is not as
expected.
If this is the case, and dosages beyond normal then have to be prescribed, TDM can
minimize the time that elapses.
TDM is important for patients who have other diseases that can affect drug levels
Or
who take other medicines that may affect drug levels by interacting with drug being
tested.
As an example, without drug monitoring, the physician cannot be sure if a patient's lack
of response to an antibiotic reflects bacterial resistance, or is the result of failure to reach
the proper therapeutic range of antibiotic concentration in the blood.
In cases of life-threatening infections, timing of effective antibiotic therapy is critical to
success. It is equally crucial to avoid toxicity in a seriously ill patient. Therefore, if toxic
symptoms appear with standard dosages, TDM can be used to determine changes in
dosing.Blood demonstrates drug action at any specific time. drug levels examined from
Urine reflect the presence of a drug over many days (depending on the rate of excretion).
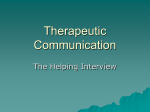
Therapeutic Drug Monitoring: Therapeutic And
Toxic Range
Drug Level∗ Use
Therapeutic
Toxic
Level∗
∗Values are laboratory-specific
∗∗Concentration obtained 30 minutes after the end of a 30-minute infusion.
Acetaminop Analgesic,
hen
antipyretic
mg/ml
Depends on >250
use
Amikacin
mg/
ml
12-25 mg/
ml∗∗
Antibiotic
>25
Aminophylli Bronchodila 10-20
ne ng/
tor
mg/ml
ml
>20
Amitriptylin Antidepress 120-150
e ng/
ant
ng/ml
ml
>500
Carbamaze Anticonvuls 5-12 mg/ml >12
pine
ant
mg/ml
Chloramphe Antibiotic
nicol
mg/ml
Digoxin
ng/ml
10-20
mg/ml
Cardiotonic 0.8-2.0
ng/ml
>25
>2.4
entamicin
Antibiotic
4-12 mg/L
>12
mg/L
Lidocaine
Antiarrhythmic
1.5-5.0 mg/ml
>5 mg/
ml
Lithium mEq/L
Antimanic
0.7-2.0 mEq/L
>2.0
Nortriptyline ng/
ml
Antidepressant
50-150 ng/ml
>500
Phenobarbital mg/
ml
Anticonvulsant
10-30 mg/ml
>40
Phenytoin mg/ml
Anticonvulsant
7-20 mg/ml
>30
Procainamide mg/
ml
Antiarrhythmic
4-8 mg/ml
>16
Propranolol ng/ml
Antiarrhythmic
50-100 ng/ml
>150
Quinidine
mg/ml
Antiarrhythmic
1-4 mg/ml
>10
Theophylline
mg/
ml
Bronchodilator
10-20 mg/ml
>20
Tobramycin
mg/
ml
Antibiotic
4-12 mg/ml∗∗
>12
Valproic acid
mg/
ml
Anticonvulsant
50-100 mg/ml
>100
Values are laboratory-specific
∗∗Concentration obtained 30 minutes after the end of a 30-minute infusion.
Blood specimens for drug monitoring can be taken at two different times: during the
drug's highest therapeutic concentration ("peak" level), or its lowest ("trough" level).
Occasionally called residual levels, trough levels show sufficient therapeutic levels;
whereas peak levels show poisoning (toxicity). Peak and trough levels should fall
within the therapeutic range.
Preparation
In preparing for this test, the following guidelines should be observed:
Depending on the drug to be tested, the physician should decide if the patient is to be
fasting (nothing to eat or drink for a specified period of hours) before the test.
For patients suspected of symptoms of drug toxicity, the best time to draw the blood
specimen is when the symptoms are occurring.
If there is a question as to whether an adequate dose of the drug is being achieved, it is
best to obtain trough (lowest therapeutic concentration) levels.
Peak (highest concentration) levels are usually obtained one to two hours after oral
intake, approximately one hour after intramuscular (IM) administration (a shot in the
muscle), and approximately 30 minutes after intravenous (IV) administration. Residual, or
trough, levels are usually obtained within 15 minutes of the next scheduled dose.
Risks
Risks for this test are minimal, but may include slight bleeding from the blood-drawing
site, fainting or feeling lightheaded after blood is drawn, or accumulation of blood under
the puncture site (hematoma).
Resources
Books
Pagana, Kathleen Deska. Mosby's Manual of Diagnostic and Laboratory Tests. St. Louis:
Mosby, Inc., 1998.
Gale Encyclopedia of Medicine. Copyright 2008 The Gale Group, Inc. All rights reserved.