Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
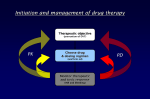
Therapeutic drug Monitoring What is therapeutic drug monitoring (TDM)? Individualization of drug doses by maintaining plasma/blood drug concentrations within a target range---- therapeutic range therapeutic window. Takes care of inter-individual variability. Therapeutic Window Therapeutic failure results when either the concentration is too low, ineffective therapy, or is too high, producing unacceptable toxicity. Between these limits of concentration lies a region associated with therapeutic success – regarded as a Therapeutic window. Wide therapeutic window A Toxicity Response Efficacy Drug concentration (log scale) B Narrow therapeutic window Toxicity Response Efficacy Drug concentration (log Scale) Major sources of Variability: •Compliance •Age- neonates, children, elderly •Physiology- gender, pregnancy •Disease- Hepatic, renal, cardiovascular, respiratory •Drug interactions •Environmental influences on drug metabolism •Genetic polymorphisms For which drugs is monitoring helpful? •Marked pharmacokinetic variability •Concentration related therapeutic and adverse effects •Narrow therapeutic index •Defined therapeutic (target) concentration range •Desired therapeutic effect difficult to monitor TDM useful in 2 major situations: • Drugs used prophylactically to maintain absence of a condition--seizures, cardiac arrhythmias. depressive/manic episodes, transplant rejection • To avoid serious toxicity--- Aminoglycoside antibiotics Sampling and drug analysis: Plasma/ serum; cyclosporin- whole blood. Timing: least variable point in dosing interval– predose/trough concentration. Wait for steady state to be achieved---at least 5 half-lives. Exceptions are there! Drugs with long half-life. HPLC, GLC, Immunoassays- sensitivity, specificity. Information required for interpretation: •Timing of sample in relation to last dose •Duration of treatment in with current dose •Age, gender •Other drug therapy •Relevant disease states •Reason for TDM- lack of effect, routine monitoring, suspected toxicity. Plasma protein binding: Free drug vs total drug concentration. Importance of plasma protein binding. Remember that only total drug concentration is measured but only the free drug is active! Drugs commonly monitored: Drug Amiodarone Digoxin Quinidine Theophylline Phenytoin Carbamazepine Sodium valproate Phenobarbitone Gentamicin Amikacin Vancomycin Lithium Therapeutic range (mg/L) 1.0-2.5 0.5-2.1microgram/L 2.0-5.0 10-20 10-20 5.0-12 50-100 15-40 peak>5, trough<2 peak>15, trough<5 peak20-40, trough<10 0.6-1.2mmol/L Target concentration intervention ESTIMATE INITIAL DOSE Target Dose Loading Dose Maintenance Dose BEGIN THERAPY ASSESS THERAPY Patient Response Drug Level REFINE DOSE ESTIMATE ADJUST DOSE High Performance Liquid Chromatography