Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
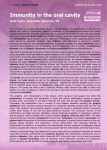
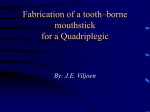
Management of patients with excessive gingival display for maxillary complete arch fixed implant-supported prostheses Avinash S. Bidra, BDS, MS,a John R. Agar, DDS, MA,b and Stephen M. Parel, DDSc University of Connecticut Health Center, Farmington, Conn Maxillary complete arch fixed implant-supported prostheses are a popular treatment option for edentulous patients. Excessive gingival display or gummy smile in edentulous patients is relatively uncommon. However, many partially edentulous patients or completely dentate patients with compromised dentition and excessive gingival display may seek a fixed implant-supported prosthesis. Some of these patients may be candidates for immediate implant placement and insertion of the prosthesis, while others may carry over their preexisting excessive gingival display to the edentulous state for a variable period of time. Both types of patients require meticulous treatment planning and often require additional preprosthetic interventions before the placement of dental implants. This report provides an overview of the etiology, diagnosis, treatment planning, and options for management of patients with excessive gingival display who seek a maxillary complete arch fixed implant-supported prosthesis. (J Prosthet Dent 2012;108:324-331) Improved surgical and prosthodontic treatment protocols and improved prosthetic designs and materials have resulted in the increased popularity of the maxillary fixed implant-supported prosthesis.1 It is known that the number of people in the United States receiving a complete denture prosthesis will increase despite an anticipated decline in the age-specific rates of edentulism.2 Douglass et al2 estimated that about 38 million adults will need 1 or 2 complete denture prostheses by the year 2020 because of the significant increase in the population older than 55 years. These projections were based on factors such as age-specific population, age-specific percentage of edentulism, declining trends in edentulism, and percentage use of dentures. The actual number of adults in need of complete dentures and subsequent implant-based rehabilitation may be even higher than projected in this study. This is because the study did not consider those completely dentate and partially eden- tulous adults with compromised or terminal dentition who may be indicated for edentulism when they seek comprehensive dental rehabilitation. Therefore, in the contemporary setting, patients seeking a maxillary fixed implant-supported prosthesis exist across all age groups and encompass clinical characteristics that a clinician would not expect to see in a typical elderly edentulous patient. Such clinical characteristics may include excessive gingival display (commonly called gummy smile), discordant occlusal plane and associated alveolar bone levels, unfavorable jaw relationships, and bony characteristics that may not be congruent with the patient’s age. These patients may be unwilling to accept a removable prosthesis (complete dentures or implant retained overdentures) for psychological or social reasons and desire their prosthesis to be fixed and not worn.1 Some of these patients may be willing to make large financial investments for treatment and may also be willing to manage the challenges in- volved in oral hygiene and the prosthetic complications associated with the fixed implant-supported prosthesis.1 All of these factors require the clinician to diagnose the condition and meticulously plan a treatment that will provide these patients with the optimal fixed implant-supported prosthesis. Patients seeking a maxillary fixed implant-supported prosthesis have been categorized into 4 groups for the purpose of treatment planning and choosing the appropriate design of a fixed prosthesis (Fig. 1).3 Class I patients are those requiring a gingival prosthesis for esthetic tooth proportions, prosthesis contour, and adequate lip support. Class II patients are those requiring a gingival prosthesis only to obtain esthetic tooth proportions and for prosthesis contour. Lip support is not a consideration in this group, because the difference in lip projection with and without any prosthesis is not significant. Class III patients are those who do not require any gingival prosthesis. While Presented at the 93rd Annual Meeting of the Academy of Prosthodontics, Hilton Head, SC, May 5, 2011. Assistant Professor and Assistant Program Director, Post-Graduate Prosthodontics. Professor and Program Director, Post-Graduate Prosthodontics. c Private practice, Dallas, Texas. a b The Journal of Prosthetic Dentistry Bidra et al 325 November 2012 gies of gingival display in dentate patients include (1) skeletal (conditions such as vertical maxillary excess)6,11; (2) dental (anterior dentoalveolar extrusion related to Angle Class II division 2 malocclusion)6-9,11; (3) gingival (altered passive eruption)12; (4) labial (thin, short and/or hypermobile maxillary lip)11-13; and (5) a combination of the above.6,7,11 Depending upon the etiology, patients present with a varying amount of gingival display; consequently, the management methods differ. 1 Representation of classification of patients for maxillary complete arch fixed implant-supported prosthesis showing 4 different groups. Red line depicts excessive gingival display and vertical arrow shows need for bone reduction for conversion of Class IV to another class. (Figure reproduced with publisher’s permission from Bidra AS, Agar JR. A classification system of patients for esthetic fixed implant-supported prostheses in the edentulous maxilla. Compend Contin Educ Dent 2010;31:366-79.) Class I, II, and III patients can either have a low smile or medium smile, Class IV patients are distinct as they are the only group of patients who have a high smile or excessive gingival display. Therefore, they require preprosthetic intervention and conversion to another class for optimal treatment. As such, they may require a gingival prosthesis based on the outcome of the preprosthetic intervention. The purpose of this article is to provide an overview of the options for the management of patients with excessive ginigival display (Class IV) seeking a maxillary complete arch fixed implant-supported prosthesis. Types of smiles In 1984, Tjan et al4 classified human smiles from a dental perspective into low, average, and high smiles. The authors defined a display of less than 75% of the anterior tooth length as a low smile; a display of 75% to 100% of the anterior tooth length and interproximal gingiva as an average smile; and a display of 100% of the anterior tooth length and contiguous band of gingiva as a high smile.4 This classification has been accepted by prosthodontists and orthodontists.1,5 Other Bidra et al authors have classified the excessive gingival display as a fourth type of smile.6-8 This type of smile is distinct from the high smile and has been defined as exposure of the total length of the maxillary anterior teeth along with an exposure of about 4 mm of gingival tissues.8,9 This type of smile may have a multifactorial etiology. Etiology of excessive gingival display Excessive gingival display in the edentulous patient has not been frequently reported.1,3,10 This may be partly attributable to edentulism being typically associated with elderly patients, who rarely have a high or excessive gingival display.5 The reasoning could be a decrease in the ability of muscles involved in the creation of a smile to display gingiva.5 However, it is important for a clinician performing fixed implant-supported rehabilitation to understand the etiologies of excessive gingival display in dentate patients. This is because many partially edentulous patients or completely dentate patients with terminal dentition who seek fixed implant rehabilitation may carry over their preexisting excessive gingival display to their edentulous state.1 Accepted etiolo- Diagnosis and treatment planning Patients with excessive gingival display who seek complete arch fixed implant-supported prostheses can present to the clinician in various ways. They can either be completely dentate with generalized compromised teeth, partially edentulous with a few uncompromised teeth, completely and recently edentulous, or completely edentulous for a long period of time (Fig. 2). Some completely dentate and partially edentulous patients may be candidates for extractions, immediate implant placement, and immediate insertion of a fixed prosthesis. Typically, the patient with a vertical maxillary excess (VME) has an anterior and posterior excessive gingival display due to the downward position of the entire maxilla, while the patient with Class II division 2 malocclusion has an anterior excessive gingival display due to the dentoalveolar extrusion of the anterior teeth. Patients with short clinical crowns can have a varying degree of excessive gingival display, and hypermobility of the maxillary lip can be found in combination with any of the previously described situations. By using complete denture principles, the optimal maxillary incisal edge and cervical edge positions of the prosthetic teeth should be determined at the diagnostic stage.1 This allows the clinician to determine the position of the prosthesis-tissue junction (PTJ) with respect to the existing bone level and the most apical (superior) position of the maxillary 326 Volume 108 Issue 5 A B C D 2 Patients with excessive gingival display seeking maxillary fixed implant-supported prosthesis can present in various ways: A, Dentate patient with compromised teeth. B, Partially edentulous patient with compromised teeth. C, Recently edentulous patient. D, Long-term edentulous patient. A B 3 A, Excessive gingival display in this patient had been managed without addressing preprosthetic interventions or following appropriate prosthetic contours. B, Intraoral image reveals unfavorable contours (complete ridge-lap) of intaglio surface of prosthesis to compensate for excessive gingival display, which led to significant oral hygiene problems, halitosis, and failure of multiple implants. lip during maximum smile.3 If the clinician determines the need for a gingival prosthesis, then it is acceptable to display prosthetic gingiva, but it is imperative that the PTJ should not be visible in the final prosthesis during maximum smile.3 This is because it is difficult to satisfactorily match the shade of the prosthetic gingiva with the natural tissues and avoid esthetic failures.1,3 It is important to understand that the incisal and cervical edge positions of the prosthetic diagnostic teeth can affect the amount of display of the gingival The Journal of Prosthetic Dentistry prosthesis. Diagnostic teeth that are shorter than ideal or positioned too incisally may exaggerate the display of prosthetic gingiva during a patient’s maximum smile.7 Bidra et al 327 November 2012 Management options From a maxillary fixed prosthetic standpoint, patients with excessive gingival display require the most complex treatment.3 This is because they require additional preprosthetic interventions, which adds to the complexity of the treatment. Regardless of the choice of preprosthetic intervention, it is imperative that the bony platform is superior to the cervical edge positions of the teeth. This allows sufficient space for a smooth anterior-inferior transition of the prosthesis from the implant platform to the labial surface of the teeth. This will also permit the intaglio surface of the final prosthesis to have a convex contour and avoids ridge-lap contours.3 Failure to create the bony platform superior to the PTJ can result in 1 of 2 complications. First, if the bony platform is inferior to the cervical edge positions of the teeth, then the prosthesis will require a ridge lap tissue surface to conceal the visibility of the PTJ due to the patient’s gingival display. Such unfavorable contours may temporarily solve esthetic issues but can compromise the patient’s oral hygiene and lead to associated complications (Fig. 3). It is impossible to adequately correct this situation without removing the implants and raising the bony platform to a position superior to the lip during maximum smile. Second, if the bony platform were at the same level as the cervical edges of the teeth, then the tissue surface would have a horizontal ledge that makes it difficult to maintain good hygiene. The correction of this situation may necessitate more superior or inferior positioning of the anterior teeth, which may compromise esthetics, occlusion, and oral hygiene performance. The various options for managing patients with ex- cessive gingival display who seek fixed implant-supported prostheses are further described. Ostectomy procedures Ostectomy (formerly called aveolectomy) is defined as the excision of bone or a portion of a bone, usually by means of a saw or chisel, for the removal of a sequestrum, the correction of a deformity, or any other purpose.14 This procedure is generally indicated in patients with mild to moderate gingival display attributable to dental (Angle Class II division 2 malocclusion), gingival (altered passive eruption), or labial (thin, short, and/or hypermobile maxillary lip) causes. An ostectomy should be undertaken before implant placement, such that the bony platform is superior to the most apical position of the maxillary lip in maximum smile15 (Fig. 4). The new bony A B C D 4 A, Partially edentulous patient with excessive gingival display desiring fixed prosthesis. B, After extractions, ostectomy was performed with reciprocating saw to raise level of bony platform superior to predetermined maximum lip position. C, Appearance of new bony platform before placement of implants and confirmed to be superior to level of lip during maximum smile. D, Posttreatment result shows prosthesis-tissue junction adequately concealed underneath lip during maximum smile. Bidra et al 328 Volume 108 Issue 5 A B 5 A, Esthetic failure in this patient with excessive gingival display occurred because implants had been placed without addressing preprosthetic interventions. Use of gingival prosthesis and posterior metal margins further compromised esthetics because of visibility of prosthesis-tissue junction. B, Situation was managed by eliminating posterior metal margins and gingival prosthesis and conversion to Class III. Long proximal contacts continued to compromise esthetic result. platform should ensure that there is adequate width and sufficient height for implant placement, without encroaching on the nasal floor or the maxillary sinus.15 If this is not possible, alternative sites for implant placement, which may change the design of the planned fixed prosthesis, should be carefully considered. A combination of advanced radiographic imaging and a bone reduction guide made from a diagnostic denture can help the clinician achieve the appropriate amount of reduction.15 Depending upon the excessive gingival display and the planned prosthetic design, the ostectomy procedure may be required only in the anterior region, where a gingival prosthesis may be needed; the posterior region can then be restored with a fixed dental prosthesis without gingival prosthesis. The patient could, therefore, be classified as a Class II in the anterior region and Class III in the posterior region.3 Lefort I osteotomy Lefort I osteotomy is commonly recommended in the orthodontic and orthognathic surgery literature for situations such as vertical impaction of the maxilla in the VME condition, to advance the maxilla, and to decrease facial height.6,7,16 In patients with a dolichofacial appearance and a retruded chin, this procedure can also involve autorotation of the mandible, which can improve the overall facial appearance.6,7 Several articles in the implant literature have also described the use of Lefort I osteotomy to advance the atrophic edentulous maxilla and in combination with interpositional grafts to provide bone augmentation for fixed implantsupported prostheses.17-21 The use of Lefort I osteotomy to correct excessive gingival display in an edentulous patient with VME has been reported previously in the prosthodontic literature.10 This procedure involved the vertical impaction of the maxilla, followed by the autorotation of the mandible and the subsequent fabrication of new complete dentures. Although no similar reports are presently found in the literature for patients seeking complete arch fixed implant-supported prosthesis, the same approach is indicated. The goal is to ensure that the Lefort I osteotomy can position the bony platform superior to the most apical position of the maxillary lip to avoid display of the PTJ. Excessive ostectomy is not a substitute for Lefort I osteotomy in VME patients because of the risk of encroaching on the nasal floor or maxillary sinus and also the risk of divesting any available bone for placement of implants.3 The Journal of Prosthetic Dentistry Preprosthetic orthodontic intrusion Preprosthetic orthodontic intrusion of the anterior teeth may be indicated in patients with an anterior excessive gingival display, attributable to Class II division 2 malocclusion.6,11 It may also be indicated in patients with a hypermobile maxillary lip and an insufficient height of bone in the anterior maxilla. In such situations if the planned fixed prosthetic design necessitates the placement of implants in the maxillary anterior region, ostectomy procedures should be avoided. This is because it can deprive the clinician of any available bone for placing implants in this region and risk encroaching on the nasal floor. Appropriate preprosthetic orthodontic intrusion by itself, or in combination with minor bone contouring, can ensure that when the teeth are extracted, the bony platform for implants is not only adequate but lies superior to the lip during maximum smile.3 This can prevent the visibility of the PTJ under maximum smile. Potential root resorption related to any rapid orthodontic intrusion movements are less of a concern in this situation because the teeth would eventually be extracted. Bidra et al 329 November 2012 Plastic surgery procedures When a patient’s excessive gingival display is due to a hypermobile maxillary lip not found in combination with other etiologies, and the patient refuses ostectomy, Lefort I, or preprosthetic orthodontic procedures, then plastic surgery procedures may be an option. These procedures can range from surgical techniques such as lip repositioning procedures11 or lip lengthening procedures such as V-Y cheiloplasty,13,22 or use of nonsurgical techniques such as botulinum toxin injections.9,23,24 The inherent approach with both modalities is to limit the apical movement of the upper lip during maximum smile. Depending on each patient, the outcome may be different and may require repetitive treatment. Patients choosing these options should be cautioned about the lack of longterm validity of such interventions. In lip lengthening procedures such as V-Y cheiloplasty, a V-Y shaped incision is made in the vestibule of the anterior maxilla with a vertical incision behind the philtrum of the maxillary lip. The incisions are then closed by mattress sutures, resulting in a vertical scar closure and eventual reorientation of the associated muscles.13,22 The lip repositioning procedure was initially described by Rubinstein and Kostianovsky25 by limiting the retraction of the elevator muscles involved in a smile. It has been reported by plastic surgeons and periodontists with minor modifications.26-29 This technique involves making 2 partial thickness incisions in the gingiva and mucolabial fold and dissecting an elliptical piece of tissue between them. Then, the upper lip is inferiorly positioned, and the inner labial mucosa is sutured to the gingiva about 4 mm above the free gingival margin.28,29 This procedure reduces the vestibular depth and restricts upper lip elevation during the smile, thereby reducing the amount of gingival tissue exposure. All of these procedures may allow the PTJ to be concealed underneath the upper lip during maximum smile. Bidra et al No intervention and conversion to a Class III patient This option can be selected as long as the patient does not present with skeletal or dental etiologies of excessive gingival display, which can preclude prosthetic teeth from being positioned for optimal esthetics. Additionally, this option may be chosen for those patients who refuse any preprosthetic interventions, such as ostectomy or plastic surgery procedures, to conceal the PTJ underneath the lip. Therefore, a gingival prosthesis should not be used in these patients, and they should be converted to a Class III situation (patients who do not require a gingival prosthesis).3 This is because when the PTJ is visible during maximum smile, the use of any gingival prosthesis (porcelain/composite resin/acrylic resin) can lead to esthetic failures as it is difficult to match the shade of the prosthetic gingiva and the natural tissues satisfactorily3 (Fig. 5). A slight gingival display, especially in younger women, has been reported to be esthetically acceptable.30 However, management of such situations in complete arch fixed implant-supported prosthetic rehabilitation is challenging.3 This is because achieving an esthetic interproximal papilla-like tissue between 2 implants or between an implant and pontic is often difficult.31,32 To overcome this situation, long proximal contacts are required between all prosthetic teeth, which can compromise the esthetic result. Furthermore, achieving optimal contours of other elements related to dentogingival esthetics, such as gingival levels, gingival symmetry, and gingival zenith, is challenging, but could otherwise be achieved relatively easily by using prosthetic gingiva.33,34 In completely dentate and partially edentulous patients, immediate placement and immediate loading may be helpful to obtain better soft tissue outcomes.35,36 The patient should be cautioned about the esthetic compromises involved with this option before proceeding with treatment. No intervention/reconsider removable prosthetic options Patients with excessive gingival display who refuse preprosthetic interventions or refuse to accept the esthetic compromises involved with the option of conversion to Class III should be counseled to reconsider removable prosthetic options.37,38 This could involve a conventional complete denture, implant-supported overdenture (complete palatal coverage or a horseshoe design), or a fixed-detachable overdenture that includes a locking feature to provide a more secure retentive feeling similar to the Marius Bridge.39 However, it is important to caution these patients that once the implants are placed for a removable prosthesis, any future desire to obtain a fixed prosthesis may necessitate the removal of these implants during preprosthetic intervention. This is followed by ostectomy procedures to establish the new bony platform superior to the most apical position of the maxillary lip and placement of new implants (Fig. 6). All of these can result in additional treatment procedures, time, and expense. Patients refusing this option should be encouraged to obtain treatment with a conventional complete denture or no treatment until they are certain about their treatment choice. SUMMARY This article provided a review of the etiology, diagnosis, treatment planning, and management options for patients with excessive gingival display who seeking a maxillary complete arch fixed implant-supported prosthesis. Patients with excessive gingival display can present in various ways, such as completely dentate with generalized compromised teeth, partially edentulous with a few good teeth, completely and recently edentulous, or completely edentulous for a long period of time. The management options range from preprosthetic hard or soft tissue interventions to providing no 330 Volume 108 Issue 5 A B C D E 6 A, Patient with excessive gingival display was unsatisfied with bar-supported overdenture and requested fixed prosthesis. B, Overdenture bar was so inferior (due to excess bone) that bar itself was revealed when lips were in repose. C, As patient desired fixed prosthesis, removal of previous implants and ostectomy to raise bony platform and placement of new implants was needed. D, Fixed implant-supported prosthesis was immediately inserted on new implants. E, Posttreatment result shows prosthesis-tissue junction adequately concealed underneath lip during maximum smile. treatment and reconsidering the removable prosthetic option. Successful communication with the patient at the treatment planning stage is imperative before proceeding with this expensive and potentially invasive treatment. REFERENCES 1. Bidra AS. Three-dimensional esthetic analysis in treatment planning for implant-supported fixed prosthesis in the edentulous maxilla: review of the esthetics literature. J Esthet Restor Dent 2011;23:219-36. 2. Douglass CW, Shih A, Ostry L. Will there be a need for complete dentures in the United States in 2020? J Prosthet Dent 2002;87:5-8. The Journal of Prosthetic Dentistry 3. Bidra AS, Agar JR. A classification system of patients for esthetic fixed implant-supported prostheses in the edentulous maxilla. Compend Contin Educ Dent 2010;31:366-79. 4. Tjan AH, Miller GD, The JG. Some esthetic factors in a smile. J Prosthet Dent 1984;51:24-8. 5. Desai S, Upadhyay M, Nanda R. Dynamic smile analysis: changes with age. Am J Orthod Dentofacial Orthop 2009;136:310.e1-10. Bidra et al 331 November 2012 6. Sarver DM. Esthetic orthodontics and orthognathic surgery. St. Louis: Mosby; 1998. p. 8-27. 7. Proffit WR, White RP, Sarver DM. Contemporary treatment of dentofacial deformity. St. Louis: Mosby; 2002. p. 403-500. 8. Fradeani M. Esthetic analysis: a systematic approach to prosthetic treatment. Hanover Park: Quintessence Publishing Co; 2004. p. 52-124. 9. Polo M. Botulinum toxin type A in the treatment of excessive gingival display. Am J Orthod Dentofacial Orthop 2005;127:214-8. 10.Massad JJ, Brannin DE, Goljan KR. Gingival smile enhancement for the edentulous patient by using a LeFort I osteotomy. J Prosthet Dent 1991;66:151-4. 11.Silberberg N, Goldstein M, Smidt A. Excessive gingival display--etiology, diagnosis, and treatment modalities. Quintessence Int 2009;40:809-18. 12.Garber DA, Salama MA. The aesthetic smile: Diagnosis and treatment. Periodontol 2000 1996;11:18-28. 13.Peck S, Peck L, Kataja M. The gingival smile line. Angle Orthod 1992;62:91-100. 14.The glossary of prosthodontic terms. J Prosthet Dent 2005;94:10-92. 15.Jensen OT, Adams MW, Cottam JR, Parel SM, Phillips WR 3rd. The All-on-4 shelf: maxilla. J Oral Maxillofac Surg 2010;68:2520-7. 16.Proffit, WR, Fields HW, Sarver DM. Contemporary orthodontics. 4th ed. St. Louis: Mosby; 1997. p. 688-710. 17.Sailer HF. A new method of inserting endosseous implants in totally atrophic maxillae. J Craniomaxillofac Surg 1989;17:299-305. 18.Kahnberg KE, Nilsson P, Rasmusson L. Le Fort I osteotomy with interpositional bone grafts and implants for rehabilitation of the severely resorbed maxilla: a 2-stage procedure. Int J Oral Maxillofac Implants 1999;14:571-8. 19.Ellis E 3rd, McFadden D. The value of a diagnostic setup for full fixed maxillary implant prosthetics. J Oral Maxillofac Surg 2007;65:1764-71. 20.Chiapasco M, Brusati R, Ronchi P. Le Fort I osteotomy with interpositional bone grafts and delayed oral implants for the rehabilitation of extremely atrophied maxillae: a 1-9-year clinical follow-up study on humans. Clin Oral Implants Res. 2007;18:74-85. 21.Hallman M, Mordenfeld A, Strandkvist T. A retrospective 5-year follow-up study of two different titanium implant surfaces used after interpositional bone grafting for reconstruction of the atrophic edentulous maxilla. Clin Implant Dent Relat Res 2005;7:121-6. 22.Sarver DM, Rousso DR. Plastic surgery combined with orthodontic and orthognathic procedures. Am J Orthod Dentofacial Orthop 2004;126:305-7. 23.Polo M. Botulinum toxin type A (Botox) for the neuromuscular correction of excessive gingival display on smiling (gummy smile). Am J Orthod Dentofacial Orthop 2008;133:195-203. 24.Gracco A, Tracey S. Botox and the gummy smile. Prog Orthod 2010;11:76-82. 25.Litton C, Fournier P. Simple surgical correction of the gummy smile. Plast Reconstr Surg 1979;63:372-3. 26.Miskinyar SA. A new method for correcting a gummy smile. Plast Reconstr Surg 1983;72:397-400. 27.Rosenblatt A, Simon Z. Lip repositioning for reduction of excessive gingival display: a clinical report. Int J Periodontics Restorative Dent 2006;26:433-7. 28.Humayun N, Kolhatkar S, Souiyas J, Bhola M. Mucosal coronally positioned flap for the management of excessive gingival display in the presence of hypermobility of the upper lip and vertical maxillary excess: a case report. J Periodontol 2010;81:1858-63. 29.Gupta KK, Srivastava A, Singhal R, Srivastava S. An innovative cosmetic technique called lip repositioning. J Indian Soc Periodontol 2010;14:266-9. 30.Geron S, Atalia W. Influence of sex on the perception of oral and smile esthetics with different gingival display and incisal plane inclination. Angle Orthod 2005;75:778-84. 31.Pradeep AR, Karthikeyan BV. Peri-implant papilla reconstruction: realities and limitations. J Periodontol 2006;77:534-44. 32.Tarnow D, Elian N, Fletcher P, Froum S, Magner A, Cho SC, et al. Vertical distance from the crest of bone to the height of the interproximal papilla between adjacent implants. J Periodontol 2003;74:1785-8. 33.Coachman C, Salama M, Garber D, Calamita M, Salama H, Cabral G. Prosthetic gingival reconstruction in fixed partial restorations. Part 1: introduction to artificial gingiva as an alternative therapy. Int J Periodontics Restorative Dent 2009;29:471-7. 34.Coachman C, Salama M, Garber D, Calamita M, Salama H, Cabral G. Prosthetic gingival reconstruction in fixed partial restorations. Part 3: laboratory procedures and maintenance. Int J Periodontics Restorative Dent 2010;30:19-29. 35.Tarnow DP, Emtiaz S, Classi A. Immediate loading of threaded implants at stage 1 surgery in edentulous arches: Ten consecutive case reports with 1- to 5-year data. Int J Oral Maxillofac Implants 1997;12:319-24. 36.Misch CE, Degidi M. Five-year prospective study of immediate/ early loading of fixed prostheses in completely edentulous jaws with a bone quality-based implant system. Clin Implant Dent Relat Res 2003;5:17-28. 37.Steigmann M. Treatment sequencing for the multiunit restoration: hard and soft tissue considerations. J Oral Maxillofac Surg 2007;65:53-63. 38.Bedrossian E, Sullivan RM, Fortin Y, Malo P, Indresano T. Fixed-prosthetic implant restoration of the edentulous maxilla: a systematic pretreatment evaluation method. J Oral Maxillofac Surg 2008;66:112-22. 39.Fortin Y, Sullivan RM, Rangert B. The Marius implant bridge: surgical and prosthetic rehabilitation for the completely edentulous upper jaw with moderate to severe resorption: a 5-year retrospective clinical study. Clin Implant Dent Relat Res 2002;4:69-77. Corresponding author: Dr Avinash S. Bidra University of Connecticut Health Center 263 Farmington Avenue, L6078 Farmington, CT 06030 Fax: 860-679-1370 E-mail: [email protected] Acknowledgments The authors thank Dr. Bridget Willet-Wenning DDS for sharing her clinical image (Figure 5). Copyright © 2012 by the Editorial Council for The Journal of Prosthetic Dentistry. Availability of Journal Back Issues As a service to our subscribers, copies of back issues of The Journal of Prosthetic Dentistry for the preceding 5 years are maintained and are available for purchase from Elsevier, Inc until inventory is depleted. Please write to Elsevier, Inc, Subscription Customer Service, 6277 Sea Harbor Dr, Orlando, FL 32887, or call 800-654-2452 or 407-345-4000 for information on availability of particular issues and prices. Bidra et al