Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
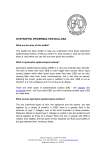
From www.bloodjournal.org by guest on June 17, 2017. For personal use only. Comparative Evaluation of Diepoxybutane Sensitivity and Cell Cycle Blockage in the Diagnosis of Fanconi Anemia By Helga Seyschab, Richard Friedl, Yujie Sun, Detlev Schindler, Holger Hoehn, Sabine Hentze, and Traute Schroeder-Kurth Fanconi anemia (FA) is a clinically and genetically heterogenous disease that is usually diagnosed on the basis of chromosomal instability reflecting the hypersensitivity towards the DNA cross-linking agents diepoxybutane (DEB) andlor mitomycin C. A lesswell-known cellular feature that characterizes FA patients is an intrinsic cell cycle disturbance consisting of prolonged progression through, and arrest within, the G2 phase compartment of the cell cycle. In a collaborative blind study, we have evaluated 72-hour lymphocyte cultures from 66 patients with clinicalsuspicionof FA both for DEB sensitivity and cell cycle disturbance. A concordant result was obtained in 63 of 66 cases. Each of the 3 discor- F ANCON1 ANEMIA (FA)is an autosomal recessive disease that is genetically heterogenous. If untreated, the course is fatal because of progressive bone marrow failure. Symptomatic therapy consists of blood cell transfusions and ccprticoids. Curative therapy consists of bone marrow transplantation. Less than 50% of FA patients exhibit a pattern of congenital anomalies suggestive of the correct diagnosis before the onset of aplastic anemia.’ Four complementation groups have been described.’ The only gene to be cloned to date specifies complementation group C located on chromosome 9q22.3 Although sequence and molecular structure of the FACC gene are known: its function remains to be elucidated. The cellular phenotype ofFA consists of chromosomal instability, a cell cycle defect, and increased sensitivity towards certain clastogens as well as Until the DNA sequences of all complementation groups are known, the differential diagnosis of FA depends on the determination of the cellular phenotype. When establishing the International Fanconi Anemia Registry (IFAR), Auerbach and Schroeder-Kurth agreed on the use of diepoxybutane (DEB) as the best discriminating agent for the diagnosis of FA.’ Because of their increased sensitivity towards DEB, FA cells are by this definition DEB+, whereas cells of non-FA patients are DEB-. Diagnostic problems arise in a distinct subgroup of patients in whom the result of the DEB test shows borderline values. A practical problem with the DEB test is that DEB itself is a powerful carcinogen. Many laboratories therefore use mitomycin C (MMC) as a less-dangerous substance for sensitivity testing. However, results of both agents are not fully concordant? In contrast to the numerous studies on DEB and MMC testing, the diagnostic potential of the defective cell cycle seen in FA cells has not beensystematically explored. The present study therefore has been designed as a comparative study in which peripheral blood samples of 66 patients with clinical suspicion of FA were evaluated in parallel for their DEB sensitivity and cell cycle defect. Our study seeks to answer the following questions: ( l ) Do DEB and cell cycle testing identify the same patients as FA or non-FA? (2) If so, what are the premises under which the cell cycle assay could be used for the differential diagnosis of FA? (3) If not, what are the reasons for discordant classification and what are the limitations of the cell cycle assay? Blood, Vol 85,No 8 (April 15). 1995:pp 2233-2237 dant, but only 1 of the concordantcases presented with overt leukemia. Seventeen cases were identified as classical FA because of their increased DEB sensitivity and G2 phase blockage. Fivecases showed acellcycle disturbance but only borderline DEB sensitivity. These casesmight represent atypical or nonclassical forms of FA. They would have been missed by cell cycle studies without concomitant DEB testing. Used in conjunction, cytogenetic and flow cytometric testing provide for the currently optimal diagnosis of FA in nonleukemic patients. 0 1995 by The American Societyof Hematology. MATERIALS AND METHODS Patients. Peripheral blood samples from patients suffering from hematologic diseases such as anemia, pancytopenia, aplastic anemia, thrombocytopenia, or combinations of these symptoms and from patients who presented with a spectrum of congenital phenotypic anomalies reminiscent of FA were sent to the laboratory at Heidelberg, Germany for DEB testing. With informed consent of the families, an aliquot of the blood sample was transferred in parallel to the laboratory in Wurzburg, Germany for cell cycle studies. After 3 years of blind, parallel testing the laboratories compared their results. Cytogenetic studies. The buffy coat was suspended in 40 mL of complete Chromosome Medium 1A (Biotest-Institut, Berlin, Germany) of which 3 X 10 mL was incubated as parallel experimental lymphocyte cultures for 72 hours at 37.5”C. One culture remained untreated; one received, after 48 hours, 0.1 &nL MMC (Serva, Heidelberg, Germany); and the third was treated, after 24 hours, with 0.1 pglmL DEB (Aldrich, Steinheim, Germany). Colcemid was added after 70 hours, followed by standard procedures for chromosome preparation and staining with Giemsa solution. One hundred metaphases were evaluated from each culture, but not all cultures yielded scorable metaphases. To be included in the study, a cytogenetic result had to be available at least for the DEB-treated culture. Structural chromosome aberrations were specified as follows: percentage of aberrant metaphases; breaks per cell; aberrations per aberrant cell; and types of aberrations. The cut-off values for the discrimination between FA and non-FA patients were as described previously.’ Flow cytometric studies. For cell cycle analysis by means of 5-bromo-2’-deoxyuridine (BrdU)/Hoechst 33258-ethidium bromide (EB) flow cytometry, mononuclear blood cells were isolated from Fromthe Department ofHuman Genetics, University of Wurzburg, Wurzburg, Germany; and the Department of Anthropology and Human Genetics, University of Heidelberg, Heidelberg, Germany. Submitted August 12, 1994; accepted November 29, 1994. Supported in part by a DFG grant to SFB I72 (H.H.). Address reprint requests to Helga Seyschab, PhD, Department of Experimental Oncology, St Jude Children’s Research Hospital, 332 N Lauderdale, PO Box 318, Memphis, TN 38101-0318. The publication costs of this article were defrayed in part by page charge payment. This article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. section 1734 solely to indicate this fact. 0 1995 by The American Society of Hematology. 0006-4971/95/8508-0006$3.00/0 2233 From www.bloodjournal.org by guest on June 17, 2017. For personal use only. SEYSCHAB ET AL 2234 16 32 18 64 80 96 112 12 1281 '4 It I6 32 40 64 80 96 112 11 BrdU/HOECHST FLUORESCENCE D I6 32 heparinized bloodviathe standard Ficoll sedimentation technique (density. 1.077 glmL: Ficoll-Paque: Pharmacia, Uppsala, Sweden). A totalof 1 X 10' cellslmL each was placed into 25-cm' culturegrade plastic flasks (Nunc, Wiesbaden, Germany) containing 5 mL of RPMl 1640 medium (GIBCO, Grand Island, NY), supplemented with 1% autologous serum. 15% heat-inactivated fetal calf serum (GIBCO). 1 X IO-' mol/L 2'-deoxyuridine (Sigma, Deisenhofen, Germany), 2 X IO-' mol/L 1-monothioglycerol (Sigma), and I X 10" mol/L BrdU (Sigma). Cells were stimulated using 1.8 pglmL phytohemagglutinin (Wellcome Diagnostics, Burgwedel. Germany) and incubated at37.5"C in 5% COz incubators using atmospheric oxygen conditions. After 72 hours, the samples were centrifuged and resuspended in freezing medium containing RPMl 1640. 10% fetal calf serum, and 10% dimethyl sulphoxide and stored frozen at -20°C until analysis. Before bivariate flow cytometric measurements. the frozen aliquots were thawed, pelleted, and resuspended at 4 X IO5 cellslmL in staining buffer containing 0. I mol/L Tris-HCI. pH 7.4.0.154 moll L NaCI, 0.5 mmol/L MgCl I mmol/L CaCl?. 0.1% NP40,and 0.2% bovine serum albumin (Sigma). The cells were stained with 1.2 pglmL Hoechst 33258 (Sigma), incubated for 15 minutes at 4°C. then stained with 1.5 pglmL ethidium bromide (Serva). and incubated for another 15 minutes at 4°C. Dual-parameter flow cytometry was performed with an arc-lamp flow cytometer (ICP-22: Phywe AG, Goettingen. Germany) interfaced to a personal computer. The examples shown in Fig I illustrate the principle of qualitative and quantitative cell cycle differences that can be assessed by the BrdUlHoechst cell cycle assay. Figure IA depicts the 72-hour cell ', 40 M 89 96 112 BrdU/HOECHST FLUORESCENCE l Fig l . Bivariate cytograms of peripheral blood lymphocytes stimulated with phytohemagglutinin and cultured for 72 hours without treatment. Each cytogram represents the BrdUl Hoechst andthe EB fluorescence by increasing channel numbers. The quantitative analysis is given in Table 1. (A) Healthy donor. The respectivecellcycle phasesoffourcellcyclesdisplayed are denoted asfollows: GO-G1 and G 2 are the respective compartments of the first cycle; Gl', Gl", and G l " ' stand forthe second, third, and fourth cell cycle G1-phases, respectively; G2' and 62" are the respective G 2 compartments of the second and third cellcycle. (B) FA patient. The elevated G 2 phases of the first and second cell cycle are marked by arrows. IC and D) Cell cycle analysis over four consecutive cell cycles (CC) of the cytograms shown in the respective upper panels. cycle distribution of lectin-activated mononuclear blood cells from a 6-year-old healthy donor. Most of his cells have progressed into the second and third cell cycle. There are very few cells left in the G2 phase compartment ofthefirstcell cycle. In contrast, the 72hour cell cycle distribution of a 5-year-old DEB' patient with the clinical diagnosis of FA (Fig IB) exhibits striking accumulations of second cell cells in the G2 phase compartments of thefirstand cycle (arrowheads). Exposure toMMC or DEB accentuates these accumulations in FA cultures, but, in addition, causes other cell cycle changes that are not found in untreated cultures such as used for this study (data not shown). The quantitative evaluation of these cytograms (shown in thebottom panels ofFig 1) uses electronic framing ofthe respective cell cycles and computerized cell cycle fitting as described by Rabinovitch et al."' An important prerequisite for the applicability of the BrdU-Hoechst technique in thehuman peripheral blood cell system is that incorporation of the base analogue does not by itself cause a cell cycle disturbance. This fact has been established in previous studies withhealthyblood donors of various ages." RESULTS Cytogenetic testing. Table 1 summarizes the results of the cytogenetic testing. Usingthe criteria established previously by Schroeder-Kurth et al," the lymphocytes of 42 of the 66 patients tested were not sensitive towards DEB, because their blood cultures showedlessthan 20% aberrant cells after DEB exposure. The breakage rate in this group From www.bloodjournal.org by guest on June 17, 2017. For personal use only. 2235 DIAGNOSIS OF FANCONIANEMIA Table 2. Resutts of Cell Cvcle Testing Table 1. Results of Cytogenetic Testing Sum of G1 Sum of S Sum of G2 % Aberrant Cellst Breaks/Cells Aberrant Cell Category N PhasesIGF PhasedGF PhasedGF 1-20 1 4-42 0.03-0.28 0.0-0.1 0.04-1.28 1.90-8.55 0.05-0.85 1.60-6.00 0.65-2.30 1.0-1.7 1.0-1.7 1.0-2.5 1.2-8.15 1 .O-1.8 1.2-6.2 1.8-2.8 Controls G2G2' 30 43 23 0.43 f 0.06 0.45 ? 0.09 0.27 f 0.07+ 0.40 2 0.06 0.40 f 0.07 0.31 ? 0.06* 0.17 ? 0.03 0.15 f 0.05 0.42 f 0.10* Aberrationd Category N 42 0-1 42 Spont MMC 38 DEB'S 54-1 19 17 Spont MMC 56-1 13 DEB*§ 5 DEB- 00 5-40 00 29-68 Seventy-two-hour lymphocytecultures were treated after 24 hours with 0.1 pg/mL DEB. Standard chromosome preparations were scored for structural chromosome aberrations. The results are ranges of values. Not all patient cultures yielded scorable metaphases in the last two categories. Abbreviations: DEB-, lack of DEB sensitivity; DEB+. DEB sensitive; DEB*, borderline sensitive; MMC, MMC-induced breakage; Spont, spontaneous chromosome breakage. t Ranges of aberrations observed. Includes 1 case with exceptional sensitivity (see Table 4, case no. 6). 5 Results of spontaneous and MMC-induced breakage are given in Table 4. * was less than 0.28 breakdcell, and there were no cells with more than 1.7 breaks. This group will be referred to as DEB-. The cells of 19 patients proved sensitive towards DEB, as evidenced by their elevated chromosomal breakage rates. In these DEB-sensitive patients, an average of 88.6% aberrant cells and an average of more than 5.63 breakskell were found, including single metaphases with more than 10 breaks. This group will be referred to as DEB+ (Table 1). The cytogenetic classification of 5 of the 66 patients proved difficult. These patients were classified as FA-like, because their cells showed a significant increase of chromosomal instability after exposure to DEB. However, their values remained well below the level of 80% to 100% aberrant cells typically found in FA cultures. Moreover, not a single cell with more than 10 aberrations was found in this group. These patients will be referred to as DEB'. More details on these patients will be given in Table 4 (see below). A cytogenetic result was not obtained in all untreated (spontaneous) or MMC-treated cultures. However, the data in Table 1 show that DEB+ cases did not overlap with DEB- cases in their percentages of aberrant cells after MMC exposure. This finding also held for the category breaks per cell, but was not true for the untreated cultures. The evaluation of spontaneous breakage obviously does in no way suffice for the distinction between FA and non-FA patients. Cellcycletesting. The results of cell cycle testing are summarized in Table 2. The cell cycle distributions of patients and controls are presented as cumulative proportions of cells within each of three cell cycle compartments (GI, S, and G2) of four consecutive cell cycles. Because the fraction of noncycling cells (GO) varies greatly among individuals (eg, as a function of donor age), cumulative cell cycle distributions were calculated relative to the growth fraction. The growth fraction (GF) was defined as the sum of all proliferating cells except the nonproliferating GO phase Cell cycle analysis was performed on72-hour lymphocyte cultures. Proliferation-independent parameters were calculated as a ratio of the sum of the respective cell cycle compartments versus the growth fraction. The values are mean f SD. P < .0001 (Student's t-test). cells. Table 2 shows that the cell cycle parameters of 43 of the 66 patients did not deviate significantly from those of 30 healthy controls. Specifically, there was no evidence for G2 phase blockage (sum of G2 phases/GF). This group of patients will be referred to as G2-. The lymphocyte cultures of each of the remaining 23 patients showed a marked shift of their cell cycle distributions. In addition to deviations affecting the G1- and S-phase compartments, there were highly significant accumulations of cells in the G2-phase compartments. Such G2-phase accumulations were described previously for patients with Fanconi The group of 23 patients exhibiting a disturbed cell cycle distribution will be denoted as G2+. Correlationbetween DEB and cell cycletesting. Because the primary emphasis of this study was onthe comparison between DEB and cell cycle testing, only those results are shown in Table 3. DEB- patients were, as a rule, G2(1 exception), whereas DEB+ patients were G2+ (2 exceptions). All 5 DEB' cases showed G2-phase blockage. In the DEB+ group, the degree of DEB sensitivity (expressed as breaks per cell) was weakly correlated to the extent of G2 phase blockage ( r = .36). However, this weak correlation was caused by a single patient whose lymphocytes were both highly DEB sensitive and G2 arrested. When this patient's data were omitted from the regression analysis, chromosome breakage rates and the extent of G2-phase blockage were unrelated ( r = M). Exceptional cases. Table 4 lists clinical, cytogenetic, andflow cytometric details of exceptional cases. None of these patients displayed radial ray defects, hyperpigmentation, or other dysmorphic features, except microcephaly (patients no. l and 2). The group of DEB' (borderline-positive) patients consisted of 2 patients with the clinical diagnosis Table 3. Correlation Between DEB and Cell Cycle Testing in 66 Patients With Clinical Suspicion of FA G2- DEBDEB+ DEB*$ 41 2t - G2+ It 17 5 Sixty-six patients with clinicalsuspicion of FA were tested in parallel for DEB sensitivity and cell cycle disturbance. The numbers of patients in each category is listed. t Patients no. 6 through 8, Table 4. Borderline positive; patients no. 1 through 5, Table 4. * From www.bloodjournal.org by guest on June 17, 2017. For personal use only. SEYSCHAB ET AL 2236 Table 4. Exce@ional Cams: Clinical, Cytogenetic, andFlow Cytometric Details Case No. Clinical Information Culture Transient thrombocytopenia. microcephaly, A A ? Anemia, thrombocytopenia, microcephaly Anemia, thrombocytopenia; BMT+ Mild anemia, thrombocytopenia; twin brother to no. 5 AA (deceased); twin brother to no. 4 6 AA, ALL (deceased) 7 MDS, AML? 8 (deceased) AA, ALL; BMT' Lymphocyte Test % Aberrant Cells Spont 1 Spont 0.09 2 MMC 1 MMC 2 DEB 1 DEB 0.90 2 Spont 0.56 MMC DEB Spont MMC DEB Spont 1 Spont 2 MMC DEB 1 DEB 2 Spont 1 Spont 2 MMC DEB 1 DEB 2 Spont MMC DE B Spont 1 Spont 2 MMC DEB Spont DEB 5 6 48 14 33 32 38 44 50 3 28 29 12 5 54 12 64 11 11 52 10 68 85 100 0.92 1.40 0.03 0.56 0.65 0.13 0.05 1.90 0.16 1.98 0.13 0.12 1.60 0.40 2.30 2.85 10.0 +++ +++ 64 100 5 10 BreaksKell Aberrant 0.05 1.20 0.22 1.10 2.20 7.20 0.05 0.14 Aberrations1 Cell 1.o 1.3 1.8 1.3 2.3 2. l 1.5 2.0 2.8 1.o 1.8 1.8 1.1 1.o 3.2 1.3 2.2 1.2 1.1 2.3 1.1 2.6 35.0 10.0 ++c 2.8 5.8 1.o 1.2 GF Flow Cytometric Classification DEB* 0.478 G2' DEB* 0.400 G2' DEB* 0.347 G2' DEB* 0.397 0.373 G2' DEB* 0.516 0.435 G2 DEB"' 0.097 G2- DEB- 0.305 0.212 G2' G2- DEB- 0.319 G2' Cytogenetic Classification X21 Detailed clinical, cytogenetic and flow cytometric data from the exceptional cases found in this study. Abbreviations: AA, aplastic anemia; AML, acute myeloid leukemia; BMT', successful bone marrowtransplantation; DEBX, borderline sensitivity to DEB, atypical Fanconi anemia (FA-like syndrome); DEB+, sensitive to DEB (classical FA); DEB-, not sensitive to DEB (non-FA); DEB"', extremely sensitive to DEB (no quantitative evaluation possible); G2'. G2-phase blockage (typical for FA); G2-, no GP-phase blockage (non-FA); ZG2/GF, sum of G2 phases over growth fraction; MDS, Myelodysplastic syndrome; Spont, spontaneous chromosome breakage. of anemia and thrombocytopenia (patients no. 2 and 3) and 3 patients with the diagnosis of incipient aplastic anemia (patients no. 1,4,and 5). In contrast to their borderline DEB and MMC sensitivities on repeated testing, each of these patients displayed unequivocal evidence for GZphase blockage. Table 4 also includes data on the 3 patients in this studyin whom DEB and cell cycle testing were clearly discordant (see Table 3). The clinical parameter common to these three discordant individuals (patients no. 6 through 8) was the presence of hematoproliferative disease, although the presence of acute lymphoblastic leukemia (ALL) is not typical for FA.'4 Whereas patients no. 6 and 7 experienced a rapid progression of their disease precluding any further cytogenetic or cell genetic testing, patient no. 8 is alive and well after a successful bone marrow transplant. DISCUSSION There is an impressive body of evidence that substantiates the validity of the DEB test for the diagnosis of Fanconi anernia.I5 Indeed, the DEB test undoubtedly represents the gold standard against which any new test must be measured. Despite this excellent record, the DEB test isnot trivial because it requires a high degree of cytogenetic expertise and meticulous attention to cell culture and safety conditions. These limitations have motivated several groups to look for alternatives to cytogenetic testing. One such alternative is the cell cycle test, which is based on the observation that FA cells experience difficulties in traversing the S and G2 compartments of the cell cycle.6~"~'6 A number of reports describe the diagnostic potential of the cell cycle test for Fanconi anemia, 13.17-20but this is the first study that blindly compares cell cycle and DEB testing. Our comparative study shows a remarkable concordance between the results of parallel DEB and cell cycle testing in patients with clinical suspicion of FA. A concordant result was obtained in 63 of 66 cases. All 3 discordant cases, but only 1 of the 63 concordant cases had clinical evidence for overt leukemia. It is conceivable that leukemic cells lack the cell cycle disturbance that is characteristic of nonneoplastic FA cells. The selective growth advantage of leukemic cells would be difficult to reconcile with a severe inhibition of From www.bloodjournal.org by guest on June 17, 2017. For personal use only. DIAGNOSIS OF FANCONIANEMIA cell cycle progression. We conclude from these results that both increased DEB sensitivity and a cell cycle disturbance should be considered as consistent manifestations of the FA gene defect(s) in nonleukemic peripheral blood mononuclear cells. A similar high degree of concordance between cell cycle and cytogenetic results was reported by Berger et al, 2o who used nitrogen mustard in both cytogenetic and cell cycle testing. More importantly, these investigators also failed to obtain concordance in 3 patients with myelodysplasia or overt leukemia. The presence of hematoproliferative disease therefore imposes a definitive limitation on the cell cycle test. Given the likely extent of genetic heterogeneity in FA, the high rate of concordance between DEB+ and G2+-positive cases is rather impressive. In our cohort of 66 patients, the DEB test proved more sensitive than the cell cycle assay with regard to uncovering possible genetic heterogeneity, because 5 of the 24 DEB-positive patients showed unusually low levels of DEB sensitivity. These patients may represent a special complementation group or a subgroup denoting an FA-like entity. The course of their disease differs somewhat from classical FA in that their hematologic symptoms were less severe and progressed very slowly, if at all. Because a G2-phase cell cycle disturbance was observed in all of these patients, DEB testing seems to single out subgroups of patients with atypical FA or FA-like disease that would have been missed by the cell cycle studies alone. On the other hand, the cell cycle disturbance may precede the onset of severe aplastic anemia, as has been observed previously in a 2-year-old child.” In summary, our study confirms that both analytical methods can reliably differentiate between FA and non-FA cells. Cultured lymphocytes with elevated sensitivity towards DEB will display a G2-phase cell cycle defect and vice versa. However, this holds only for nonleukemic cells. Despite this limitation, we still consider the cell cycle test a valuable adjunct to the differential diagnosis of childhood anemias. Owing to its speed and simplicity, the cell cycle test permits a far more liberal screening of patients withany type of dysmorphia or hematologic disturbance that could herald Fanconi anemia. In particular, the many patients carrying the clinical diagnosis of aplastic anemia could be prescreened by cell cycle testing. Confirmatory DEB studies would be required only in cases with evidence for G2-phase arrest. Used in such a sequence, cell cycle and DEB testing offer a fast and economical approach towards the definitive diagnosis of a disease whose clinical presentation is quite variable.’ The unambiguous classification at the level of the cellular phenotype provides the only solid basis for current efforts to identify complementation groups and to characterize their underlying genetic defect(s) at the molecular level. REFERENCES 1. Auerbach AD, Rogatko A, Schroeder Kurth TM: International Fanconi Anemia Registry: Relation of clinical symptoms to diepoxybutane sensitivity. Blood 73:391, 1989 2. Strathdee CA, Duncan AMV,Buchwald M: Evidence for at 2237 least four Fanconi anaemia genes including FACC on chromosome 9. Nature Genet 1:196, 1992 3. Strathdee CA, Gavish H, Shannon WR, Buchwald M: Cloning of cDNAs for Fanconi’s anaemia by functional complementation. Nature 356:763, 1992 4. Gibson RA, Buchwald M, Roberts RG, Mathew CG: Characterisation of the exon structure of the Fanconi anaemia group-C gene by vectorette PCR. Hum Mol Genet 2:35, 1993 5. Schroeder TM, Anschuetz F, Knopp A: Spontane Chromosomenaberrationen bei familiirer Panmyelopathie. Humangenetik 1:194, 1964 6. Dutrillaux B, Aurias A, Dutrillaux AM, Buriot D, Prieur M: The cell cycle of lymphocytes in Fanconi anemia. Hum Genet 62:327, 1982 7. Auerbach AD, Adler B, Chaganti RSK: Prenatal and postnatal diagnosis and carrier detection of Fanconi anemia by a cytogenetic method. Pediatrics 67:128, 1981 8. Joenje H, Arwert F, Eriksson AW, De Koning H, Oostra AB: Oxygen-dependence of chromosomal aberrations in Fanconi’s anaemia. Nature 290:142, 1981 9. Schroeder-Kurth TM, Zhu TH, Hong Y,Westphal I: Variation in cellular sensitivities among Fanconi anemia patients, non-Fanconi anemia patients, their parents and siblings, and control probands, in Schroeder-Kurth TM, Auerbach AD, Obe G (eds): Fanconi Anemia. Clincal, Cytogenetic and Experimental Aspects. Berlin, Germany, Springer Verlag, 1989, p 105 10. Rabinovitch PS, Kubbies M, Chen YC, Schindler D, Hoehn H: BrdU-Hoechst flow cytometry: A unique tool for quantitative cell cycle analysis. Exp Cell Res 174:309, 1988 11. Kubbies M, Schindler D, Hoehn H, Rabinovitch PS: BrdUHoechst flow cytometry reveals regulation ofhuman lymphocyte growth by donor-age-related growth fraction and transition rate. J Cell Physiol 125:229, 1985 12. Kubbies M, Schindler D, Hoehn H, Schinzel A, Rabinovitch PS: Endogenous blockage and delay of the chromosome cycle despite normal recruitment and growth phase explain poor proliferation and frequent endomitosis in Fanconi anemia cells. Am J Hum Genet 37:1022, 1985 13. Schindler D, Kubbies M, Hoehn H, Schinzel A, Rabinovitch PS: Presymptomatic diagnosis of Fanconi’s anaemia. Lancet 1:937, 1985 14. Butturini A, Gale RP, Verlander PC, Adler-Brecher B, Gillio AP, Auerbach AD: Hematologic abnormalities in Fanconi anemia. An International Fanconi Registry study. Blood 84:1650, 1994 15. Auerbach AD: Fanconi anemia diagnosis and the diepoxybutane (DEB) test. Exp Hematol 21:731, 1993 16. Latt SA, Kaiser TN, Lojewski A, Dougherty L, Juergens L, Brefach S, Sahar E, Gustashaw K, Schreck RR, Powers M, Lalande M: Cytogenetic and flow cytometric studies of cells from patients with Fanconi’s anemia. Cytogenet Cell Genet 33:133, 1982 17. Schindler D, Kubbies M, Hoehn H, Schinzel A, Rabinovitch PS: Confirmation of Fanconi’s anemia and detection of a chromosomal aberration (1Q12-32 triplication) via BrdU/Hoechst flow cytometry. Am J Pediatr Hematol Oncol 9:172, 1987 18. Miglierina R, Le Coniat M, Gendron MC, Berger R: Diagnosis of Fanconi anemia by flow cytometry. Nouv Rev FrHematol32:391, 1990 19. Miglierina R, Le Coniat M, Berger R: A simple diagnostic test for Fanconi anemia by flow cytometry. Anal Cell Pathol 3:111, 1991 20. Berger R, Le Coniat M, Gendron MC: Fanconi anemia. Chromosome breakage and cell cycle studies. Cancer Genet Cytogenet 69:13, 1993 From www.bloodjournal.org by guest on June 17, 2017. For personal use only. 1995 85: 2233-2237 Comparative evaluation of diepoxybutane sensitivity and cell cycle blockage in the diagnosis of Fanconi anemia H Seyschab, R Friedl, Y Sun, D Schindler, H Hoehn, S Hentze and T Schroeder-Kurth Updated information and services can be found at: http://www.bloodjournal.org/content/85/8/2233.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.