Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
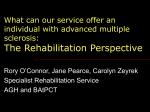
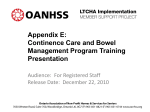
IF COMMUNITY NURSES VISIT THE CLIENT PLEASE CONTACT THEM REGARDING CONTINENCE ISSUES CARE HOME CONTINENCE REFERRAL FORM As a RGN/Carer you have regular close contact with the resident and will be very familiar with their continence issues, you can provide invaluable holistic information about the individual by completing this assessment form to help plan continence care. This should be done before requesting a Clinical Assessment by a Continence Specialist Nurse Name NHS No D.O.B Address Postcode Gender Tel Number: Date of Admission: Residential Previous Home Address: Nursing Please tick Named GP Faith Practice Name Postcode Veteran? No Yes Known Allergy No Yes Details: Learning Disability Additional Needs Communication Issues Capacity to Consent to referral No Yes Date Capacity tested Who holds the LPA? Lasting Power of Attorney in Place for Health? No Yes Medications and Home Remedies Taken – Please send in MARS Sheets Medical History Alcohol No Yes Units per week ? Smoker No Yes How many per day? What are you hoping to achieve by referring to the service? Current Incontinence Issues Please complete a Baseline Continence Chart for 3 days urinary, 7 days faecal to identify the number and pattern of incontinence episodes Urine Incontinence None Day Night Weekly Faecal Incontinence None Leakage? Daily Weekly Urine Tested Occasional Amount of Urine On Standing Up Negative/clear Light (Damp Pants) Before reaching the toilet Cloudy/Foul Smell Moderate (Wet Pants) Constant Dribble Infected Heavy (Needs Changing) Without Warning MSU Sent - Date Present Bowel Habit Open Daily Bristol Stool Type (circle) 3-4 Times a Week 1 2 3 4 5 6 7 (Please see chart) Less than 3 times a week NAME: NHS No: Fluid Intake Height How many drinks offered a day Amount of Drink consumed 1 Weight 2 ALL 3 ¾ 4 5 ½ ¼ Current MUST Score 6 0 Date Completed Patient preferred drink choice Reluctance to drink? 7 Mobility Levels 1 2 or above No Yes Aids Used Fully mobile Chair bound Able to get off the Toilet Alone Handrail in Toilet No Needs Assistance Bedbound Assisted Yes Raised Toilet seat No Yes Environmental Factors – Time taken to reach Toilet from (minutes) Lounge Dining Room Bedroom Bedroom Commode Dressing Ability Independent Some Support needed Cannot dress/undress Current Care Plan in place to support continence needs Daily Fluid Chart Daily Bowel Charts Daily Food Charts Urine Outputs Sheath with Drainage Urinal/Bedpan Catheter Intermittent Catheter Long Term Reusable Pads Disposable Pads Kyle Sheets No If so Number of pads used in 24 hours Leakage occurs with pads? Regularly Day/Night/Both Please state type of current pads used Occasionally Delete as appropriate PLEASE USE THIS SPACE FOR ANY ADDITIONAL INFORMATION THAT WILL AID ASSESSMENT FORM COMPLETED BY MAIN CARER AND DESIGNATION / R.G.N. / CARER SIGNATURE PRINT NAME DESIGNATION DATE HOME MANAGER SIGNATURE DATE Post : Continence Service, Clayton Brook Clinic, 59/60 Tunley Holme, Clayton Brook, Preston, PR5 8ES Email: [email protected] 2of 2 FAX : 01772 678084