Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
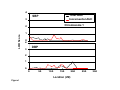
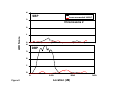
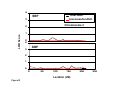
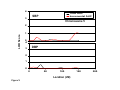
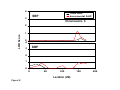
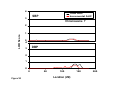
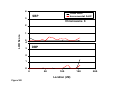
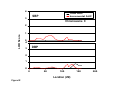
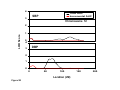
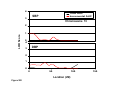
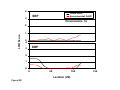
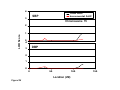
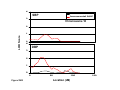
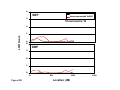
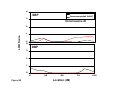
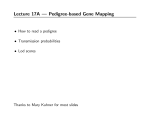
Autosomal Genome Scan for Loci Linked to Blood Pressure Levels and Trends Since Childhood The Bogalusa Heart Study Wei Chen, Shengxu Li, Sathanur R Srinivasan, Eric Boerwinkle, Gerald S. Berenson Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 Abstract—Genetic loci influencing the long-term levels and trends of blood pressure over time were investigated using 775 white siblings, ages 13 to 43 years, enrolled in the Bogalusa Heart Study, and 357 microsatellite markers on the 22 autosomal chromosomes. Subjects had been examined serially 2 to 12 times with 4365 serial observations over an average of 22 years from childhood to adulthood. Total and incremental area under the curve was calculated based on a cubic growth curve and used as long-term levels and trends, respectively. After adjusting for age, sex, and body mass index, heritability estimates of total area were 0.66 for systolic and 0.68 for diastolic blood pressure. Heritability of incremental area was 0.38 for systolic and 0.46 for diastolic blood pressure. Significant linkage to the total area of diastolic blood pressure (peak logarithm of odds [LOD]⫽3.9 at 73 cM) was observed on chromosome 2, with a region spanning from 44 cM to 103 cM showing supporting linkage evidence of LOD ⬎3.0. In addition, suggestive linkage for total area of systolic (LOD⫽1.6 at 182 cM) and diastolic blood pressure (LOD⫽2.0 at 36 cM) on chromosome 4 and diastolic blood pressure incremental area (LOD⫽2.2 at 28 cM) on chromosome 18 was noted. Several hypertension candidate genes such as ␣-adducin, -adducin, sodium bicarbonate co-transporter, and G protein-coupled receptor kinase 4 are located in these regions. Linkage evidence found in this community-based study indicates that regions on these chromosomes harbor genetic loci that affect the propensity for development of hypertension from childhood. (Hypertension. 2005;45:954-959.) Key Words: blood pressure E time within the same individual.8,9 This notion is supported by earlier findings from studies on genetics and epidemiology of blood pressure.10,11 Therefore, measures of long-term levels and trend of blood pressure may provide better insight into the identification of susceptibility loci for blood pressure or hypertension. The Framingham Offspring Study has reported genomewide linkage results of blood pressure in terms of long-term levels and trend using serial measurements during adulthood.10,12,13 However, information on the genetic loci linking longitudinal changes in blood pressure from childhood to adulthood is still limited. Longitudinal observations from the Bogalusa Heart Study, a community-based epidemiologic study of early natural history of cardiovascular risk factors beginning in childhood,14 provide an opportunity to examine the susceptibility loci influencing both between-person and within-person variability in blood pressure from childhood to young adulthood. This report provides genome-wide linkage analysis in white siblings using measures of long-term levels and trend derived from serial measurements of blood pressure extending over an average of 22 years beginning in childhood. ssential hypertension is a polygenic disorder that results from the interplay of multiple susceptibility genes and environmental factors.1 Numerous genome-wide linkage studies to localize genes influencing blood pressure and hypertension status in a number of populations and ethnic groups have found linkage evidence in regions on multiple chromosomes.2 However, most linkage studies on blood pressure and hypertension have thus far been cross-sectional in nature, representing between-person variability at a specific time point only. Blood pressure increases with age at different rates.3,4 In addition to levels, genes may also affect the longitudinal trends of blood pressure that represent within-person variability. A substantial genetic contribution to the changes in blood pressure over time has been demonstrated in longitudinal twin and family studies.5,6 A concept of “variability genes,” whose expression depends on environmental exposure, is proposed to explain the within-person variability.7 Further, using serial measurements of a trait at multiple time points dilutes the measurement errors and minimizes the short-term influences when the trait is subject to variation from time to Received February 3, 2005; first decision February 3, 2005; revision accepted February 28, 2005. From the Tulane Center for Cardiovascular Health and Department of Epidemiology (W.C., S.L., S.R.S., G.S.B.), Tulane School of Public Health & Tropical Medicine, New Orleans, La; and the Human Genetics Center and Institute of Molecular Medicine (E.B.), University of Texas–Houston Health Science Center, Houston, Tex. Correspondence to Gerald S. Berenson, MD, Tulane Center for Cardiovascular Health, 1440 Canal St, Suite 1829, New Orleans, LA 70112. E-mail [email protected] © 2005 American Heart Association, Inc. Hypertension is available at http://www.hypertensionaha.org DOI: 10.1161/01.HYP.0000161881.02361.11 954 Chen et al Genetic Loci for Blood Pressure Since Childhood 955 Figure 1. The area under the curve (AUC) of systolic blood pressure (SBP) derived from a growth curve model in white males. Individual 1: examined at ages of 10, 15, 19, 23, 29, and 35. Individual 2: examined at ages of 11, 16, 20, 26, 30, and 38. Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 Materials and Methods Study Cohort In the community of Bogalusa, Louisiana, 7 cross-sectional surveys of children aged 3 to 17 years were conducted between 1973 and 1994. In addition, 8 cross-sectional surveys of young adults aged 18 to 43 years who had been previously examined as children were conducted between 1976 and 2003. This panel design of repeated cross-sectional examinations conducted approximately every 3 years resulted in serial observations on the cohort. Eligible study subjects for this analysis comprise white siblings who participated 2 to 12 times (at least once in childhood and once in adulthood) during the period of 1973 to 2003 from childhood to adulthood. Siblings were identified based on Bogalusa sibship census database. After validation of the reported sibling relationship, there were 775 white siblings, ages 13.0 to 43.2 years at last examination, from 339 families (representing 517 full sib-pairs and 38 half sib-pairs) with 4365 observations. A majority of siblings (91.4%) were screened 3 or more times, and the average number of times examined was 5.6. The follow-up period ranged from 5 to 29 years (average, 22 years). This study was approved by the Institutional Review Board of the Tulane University Health Sciences Center. All adult subjects gave informed consent at each examination. For subjects younger than age 18 years, consent from parents was obtained. Examinations All examinations followed the same basic protocols described elsewhere.15 Indirect blood pressures were recorded in a relaxed atmosphere with Hg sphygmomanometers. Subjects were randomly assigned to 2 different stations. Well-trained observers recorded systolic blood pressure (SBP) at first and diastolic blood pressure (DBP) at fourth and fifth Korotkoff phases on the right arm in a relaxed, sitting position. Each observer recorded 3 measurements, resulting in a total of 6 readings, and the average was used as a blood pressure value at a single time point. The fourth phase was used for longitudinal analyses of DBP in children and adults because our earlier study showed the fourth phase to be more reliably measured in childhood and more predictive of adult hypertension.16 Blood pressure values were set to missing for subjects (n⫽51) who used antihypertensive medications at any examinations, and the remaining measurements were used for linkage analysis. Genotyping Genotyping of 357 highly polymorphic microsatellite markers on 22 autosomal chromosomes was accomplished using fluorescently labeled primers and an Applied Biosystems 377 sequencer (Foster City, Calif). The marker locations were determined using the genetic map provided by the Marshfield Medical Research Foundation. The mean spacing between adjacent markers was 9.0 cM (range, 0 to 25.5 cM). The average heterozygosity of the 357 markers was 0.77, with a range of 0.56 to 0.92. Details of the marker names and locations are available by request. The reproducibility of the genotyping for each marker was evaluated in 81 pairs of blind duplicate DNA samples. There was, on average, 99.7% concordance between the blind duplicate pairs, and no marker had an agreement rate ⬍96%. Statistical Analysis A cubic growth curve of blood pressure from childhood to adulthood was constructed for males and females separately using a random effects model with Statistical Analysis Software (SAS) Proc MIXED. In addition to the fixed population effects, the mixed model also incorporates random effects and has the form:17 Y⫽共0⫹b0兲⫹共1⫹b1)age⫹共2⫹b2兲age2⫹共3⫹b3兲age3⫹e where ⫽(0, 1, 2, 3)⬘ is a vector of fixed effect parameters, and b⫽(b0, b1, b2, b3)⬘ is a vector of random effect parameters. This random effects model allows the intercept, linear, and nonlinear parameters to vary from individual to individual, and the random coefficients represent the difference between the fixed population parameters and the true values for the individual. It also allows for repeated measurements and different numbers of unequally spaced observations across individuals.17 The fixed effect parameter estimates of the cubic growth curves of blood pressure in the sibling cohort were: Male: SBP⫽112.6⫹0.86age⫺0.56age2⫹0.03age3; DBP⫽68.2 ⫹0.92age⫺0.22age ⫹0.006age 2 3 Female: SBP⫽108.5⫹0.34age⫺0.75age2⫹0.06age3; DBP⫽68.9 ⫹0.53age⫺0.47age ⫹0.03age 2 3 Age was centered by subtracting 17.2, the term age2 was divided by 10, and age3 was divided by 20 to improve model fitting. Regression coefficients were all significant (P⬍0.0001) except for 0.006 (P⫽0.097) for DBP in males. As shown in Figure 1, using SBP in males as an example, the area under the curve (AUC) was calculated as the integral of the predicted growth curve parameters during the follow-up period for each individual.11,18 Total AUC is a measure of long-term levels, and incremental AUC (total AUC ⫺ baseline AUC) measures combined linear and nonlinear long-term trends. Because different individuals had different follow-up periods in this study cohort, the AUC values were divided by the number of follow-up years. The AUC method has advantages over the average value in that it can measure both long-term level and trend. Further, 956 Hypertension TABLE 1. May 2005 Means (SD) of Age, BMI, and BP of White Siblings Variable Male (n⫽359) Female (n⫽416) Total H2 (n⫽775) TABLE 2. Peak Multipoint LOD Scores (Positions, cM) for BP in White Siblings Systolic BP Age at first examination 9.3 (3.1) 9.1 (3.1) 9.2 (3.1) — Age at last examination 31.0 (7.1) 31.1 (6.9) 31.1 (7.0) — Chromosome BMI at first examination 17.4 (3.2) 17.4 (3.5) 17.4 (3.4) — BMI at last examination 28.0 (5.9) 27.8 (7.8) 27.9 (6.9) — Total AUC Diastolic BP Total AUC Incremental AUC Total AUC Incremental AUC 1 0.50 (6) 0.80 (114) 1.05 (198) 0.64 (86) 2 0.60 (87) 0.29 (259) 3.94 (73) 0.42 (170) 3 0.42 (90) 0.20 (129) 0.43 (161) 0.39 (0) Systolic BP 109.9 (7.5) 106.5 (5.8)* 108.1 (6.8) 0.66 4 1.63 (182) 0.99 (39) 2.04 (36) 0.55 (14) Diastolic BP 69.5 (5.5) 68.5 (4.1)* 69.0 (4.8) 0.68 5 0.15 (65) 1.06 (146) 0.60 (36) 0.22 (14) 6 0.30 (157) 1.23 (146) 0.64 (20) 0.93 (152) Incremental AUC Systolic BP 10.9 (4.5) 8.1 (5.2)* 9.4 (5.1) 0.38 7 0.23 (128) 0.21 (136) 0.70 (140) 0.43 (141) Diastolic BP 10.1 (3.3) 8.4 (3.5)* 9.2 (3.5) 0.46 8 0.39 (0) 0.47 (62) 1.38 (155) 0.50 (154) Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 AUC indicates area under the curve (mm Hg) divided by the number of follow-up years; BMI, body mass index (kg/m2); BP, blood pressure; H2, heritability. *P⬍0.001 for sex difference. the long-term trend (linear and nonlinear) estimated using multiple measurements is more reliable than using 2–time-point data. The biological relationship among siblings was verified using the RELTEST program (S.A.G.E. version 4.3)19 based on 357 autosomal markers. After verification of full-sibling and half-sibling relationships, genotype inconsistencies because of non-Mendelian inheritance were identified for each marker using the MARKERINFO program of S.A.G.E. Those genotypes of single individuals proven to be inconsistent were set to missing for that marker only. Maximum likelihood estimation of the marker allele frequencies was performed using the FREQ program of S.A.G.E. in siblings. A variance component method was implemented to test for evidence of linkage of a quantitative trait locus for total and incremental AUC of blood pressure. The genetic variance attributable to a specific chromosomal location was estimated based on specifying the expected genetic covariance between relatives as a function of the identity-by-descent relationships at a quantitative trait locus.20 Parameter estimates were calculated at 1-cM intervals along each chromosome. Heritability analysis and 2-point and multipoint variance component linkage analyses were performed using SOLAR 2.0,21 incorporating a simultaneous correction of covariates affecting the longitudinal levels and changes in blood pressure. These covariates were age (an average of ages at multiple time points), sex, and body mass index for total AUC. In addition, baseline blood pressure values were also included in the model for incremental AUC to control the regression-to-the-mean influence. Results As shown in Table 1, mean values of total and incremental AUC for SBP and DBP in males were significantly greater than those in females (P⬍0.001). Baseline blood pressure was negatively and significantly correlated with incremental AUC (r⫽⫺0.22 for SBP; r⫽⫺0.30 for DBP), adjusting for sex, baseline age, and baseline body mass index. In the polygenic model of variance components analyses by SOLAR, adjusting for age, sex, and body mass index, heritability estimates of total AUC were 0.66 for SBP and 0.68 for DBP. In contrast, heritability estimated using a single measurement at first examination was 0.49 for SBP and 0.36 for DBP. These values at the last examination were 0.45 for SBP and 0.46 for DBP. Heritability of incremental AUC was 0.38 for SBP and 0.46 for DBP, adjusting for baseline blood pressure in addition to the aforementioned covariates. The age range was 4 to 18 years at first examination, and 13 to 43 years at 9 0.05 (17) 0.69 (64) 0.73 (141) 0.65 (131) 10 0.40 (99) 0.91 (0) 0.26 (14) 0.24 (5) 11 0.18 (129) 0.19 (142) 0.06 (2) 0.23 (52) 12 0.49 (124) 0.30 (9) 1.54 (71) 0.46 (10) 13 0 0.98 (9) 0.62 (111) 0.91 (36) 14 0.04 (23) 0.76 (118) 1.53 (15) 0.60 (0) 15 0.93 (123) 0.31 (36) 0.66 (123) 0.29 (36) 16 0.53 (39) 0.66 (20) 0.22 (51) 1.47 (17) 17 0.86 (40) 0.07 (1) 1.18 (94) 0.01 (33) 18 0 0.97 (37) 0.32 (81) 2.17 (28) 19 0.37 (16) 0.68 (25) 0.37 (16) 0.48 (101) 20 0.42 (18) 0.69 (89) 0.59 (3) 0.02 (99) 21 0.34 (45) 0.25 (3) 22 0.11 (38) 0 0 0.21 (13) 0 0 last examination. Twenty-one subjects did not have adulthood blood pressure values because they were using antihypertensive medications and their blood pressure values were set to missing. Table 2 gives the maximum multipoint logarithm of odds (LOD) scores and locations for blood pressure AUC on 22 chromosomes. Total AUC of DBP showed significant linkage (LOD⫽3.9 at 73 cM) on chromosome 2. The point-wise empirical probability value corresponding to the LOD score of 3.9 is 0.00001. Taking into account multiple tests at every 1 cM in the present study, the genome-wide significance level is ⬍0.02 for the LOD score of 3.9 based on the genome-wide simulation study of sib-pairs.22 In addition, suggestive linkage was found for total AUC of DBP (LOD⫽2.0 at 36 cM) on chromosome 4 and incremental AUC of DBP (LOD⫽2.2 at 28 cM). For detailed LOD scores on each chromosome, please see http://hyper.ahajournals.org. Figure 2 shows multipoint LOD scores and locations on chromosome 2. A LOD score peak (LOD⫽3.9) for DBP total AUC was located at 73 cM from the p-terminal, with a region spanning from 44 cM to 103 cM supported by linkage evidence of LOD ⬎3.0. Markers within this region showing positive 2-point linkage were D2S305 (LOD⫽2.1), D2S337 (LOD⫽2.5), D2S388 (LOD⫽2.3), D2S391 (LOD⫽2.1), D2S2110 (LOD⫽2.6), and D2S2163 (LOD⫽2.4). There was no linkage evidence for DBP incremental AUC and SBP on chromosome 2. As shown in Figure 3, a LOD score peak Chen et al Genetic Loci for Blood Pressure Since Childhood 957 Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 Figure 2. Multipoint linkage results for total and incremental AUC for blood pressure in white siblings on chromosome 2: The Bogalusa Heart Study. AUC indicates area under the curve (mm Hg) divided by the number of follow-up years. Total AUC was adjusted for age, sex, and body mass index; incremental AUC was adjusted for age, sex, body mass index, and baseline blood pressure. Figure 4. Multipoint linkage results for total and incremental AUC for blood pressure in white siblings on chromosome 18: The Bogalusa Heart Study. AUC⫽area under the curve (mm Hg) divided by the number of follow-up years. Total AUC was adjusted for age, sex, and body mass index; incremental AUC was adjusted for age, sex, body mass index, and baseline blood pressure. (LOD⫽2.0) for DBP total AUC was observed at 36 cM on chromosome 4 near the marker D4S2994 (2-point LOD⫽2.1). The same location showed weak linkage to SBP total AUC (LOD⫽1.1 at 35 cM) and SBP incremental AUC (LOD⫽0.99 at 39 cM). Also, SBP had LOD score peaks near the q-terminal on chromosome 4 (LOD⫽1.6 at 182 cM for total AUC and LOD⫽0.95 at 170 cM for incremental AUC). In Figure 4, DBP incremental AUC showed a LOD score peak (LOD⫽2.2 at 28 cM) on chromosome 18 near the marker D18S843 (2-point LOD⫽2.0). SBP incremental AUC showed a maximum LOD score of 0.97 at 37 cM. No linkage evidence was found for total AUC on chromosome 18. Figure 3. Multipoint linkage results for total and incremental AUC for blood pressure in white siblings on chromosome 4: The Bogalusa Heart Study. AUC⫽area under the curve (mm Hg) divided by the number of follow-up years. Total AUC was adjusted for age, sex, and body mass index; incremental AUC was adjusted for age, sex, body mass index, and baseline blood pressure. Discussion In the present study, serial measurements of blood pressure from childhood to young adulthood were used for genomewide linkage analysis. Children and relatively younger adults of this cohort rather than older age groups may be more suited to investigate hypertension susceptibility loci because the genetically predisposed individuals tend to express blood pressure changes earlier in childhood despite the smaller variations. Further, blood pressure levels in younger subjects are relatively unobscured by prolonged lifestyle habits, less cumulative environmental exposure, and medical treatments. Blood pressure measurements in untreated subjects were used as a quantitative trait in this study, in contrast to qualitative phenotype of hypertension status used in other studies. The number of genome scans for hypertension or blood pressure has been increasing over the past decade.2 Most studies reported weak or suggestive linkage; a few studies attained significant linkage evidence.10,23–27 The present study found significant linkage evidence (LOD⫽3.9) at 73 cM on chromosome 2p13 for the long-term levels of DBP from childhood to young adulthood measured by total AUC. Although a number of regions on multiple chromosomes have been previously found in ⬎1 study,2 the region between 40 and 140 cM from the tip of the p-arm of chromosome 2 showed the most consistent and overwhelming linkage evidence for blood pressure loci.25–34 The finding on chromosomes 2 from this study replicates at least 10 other studies.25–34 The Family Blood Pressure Program selected the region between 40 and 140 cM on chromosome 2 on the basis of convincing linkage evidence in the previous studies to 958 Hypertension May 2005 Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 identify underlying candidate susceptibility genes for hypertension using combined positional candidate gene methods. Sodium bicarbonate co-transporter (SLC4A5) gene was identified as a primary candidate gene for hypertension in this region, with a LOD score of 2.84 at 93 cM.28 In the present study, the region spanning from 44 cM to 103 cM showed supporting linkage evidence of LOD ⬎3.0 (Figure 1). There are 6 markers (D2S305, D2S337, D2S388, D2S391, D2S2110, and D2S2163) within or near this region that had 2-point LOD scores of 2.11 to 2.57; D2S2110 located at 91 cM had the highest LOD score of 2.57. Of great interest, -adducin gene is located in this region, which has been previously implicated in blood pressure variation in animals and humans.35 Further, a 3-stage genome-wide search in a 12-generation pedigree demonstrated the most striking linkage result on chromosome 2p25-p24 region (9 to 23 cM), designated essential hypertension susceptibility 3 gene.26 The finding was strengthened by the evidence for linkage with marker D2S168 in a genome-wide scan of affected sib-pairs.34 In the previous longitudinal studies, significant genetic heritabilities5 and a recessive major gene effect6 have been demonstrated for the changes in blood pressure over time. In the Framingham Offspring Study, blood pressure slope and curvature over time during adulthood have been found to link to regions on chromosomes 7, 18, and 20.12,13 In this study, we found a LOD peak at 28 cM from the p-terminal on chromosome 18 for the incremental AUC of diastolic blood pressure, a combination of linear slope and nonlinear curvature. Positive linkage has also been observed around this region for long-term blood pressure levels10 and essential hypertension36 in other studies. Genes in 18p11 region are glucocorticoid deficiency-1 and melanocortin-2 receptor, a member of the G protein-coupled receptor family, which are involved in the regulation of cortisol secretion. The findings from the present and previous studies provide supporting evidence for the concept of “variability genes,” which may influence within-person variability in phenotypes over time through the gene– environment interactions.7 There is evidence for the role of ␣-adducin gene in blood pressure regulation and hypertension in animal studies and some human populations.35 Suggestive linkage to DBP total AUC was noted in this study on chromosome 4p16 where the ␣-adducin gene is located. Significant linkage evidence for blood pressure was also reported in this region in Dutch dyslipidemic families. However, no evidence was observed for an association between ␣-adducin polymorphisms and blood pressure in the same sample.24 In addition, another hypertension candidate gene, G protein-coupled receptor kinase 4,37 is closely linked to ␣-adducin gene in this location. Perspectives Essential hypertension is a polygenic disorder that results from the interplay of multiple susceptibility genes and environmental factors. However, most linkage studies on blood pressure and hypertension have thus far been cross-sectional in nature. Most previous studies reported weak or suggestive linkage; a few studies attained significant linkage evidence. Using serial measurements of blood pressure at multiple time points dilutes the measurement errors and minimizes the short-term influences. Therefore, measures of both long-term levels and trend of blood pressure may provide better insight into the identification of susceptibility loci for blood pressure or hypertension. Further, a substantial genetic contribution to the changes in blood pressure over time has been demonstrated. There is a need to investigate genetic loci for both levels and rate of change of blood pressure over time. The significant and suggestive linkage with long-term levels and trends of blood pressure found in this community-based study indicates that regions on these chromosomes harbor genetic loci that affect the propensity for development of hypertension from childhood. The quantitative trait loci identified in this study along with earlier studies serve as a basis for further fine-mapping strategies to identify and test responsible genes involved in the cause of hypertension. Acknowledgments This study was supported by grants HL-38844 from the National Heart, Lung, and Blood Institute and AG-16592 from the National Institute on Aging. Some of the results of this paper were obtained by using the program package S.A.G.E., which is supported by a US Public Health Service Research Resource Grant (1 P41 RR03655) from the National Center for Research Resources. References 1. Mein CA, Caulfield MJ, Dobson RJ, Munroe PB. Genetics of essential hypertension. Hum Mol Genet. 2004;13:R169 –R175. 2. Samani NJ. Genome scans for hypertension and blood pressure regulation. Am J Hypertens. 2003;16:167–171. 3. Kotchen JM, McKean HE, Kotchen TA. Blood pressure trends with aging. Hypertension. 1982;4:III128 –III134. 4. Pearson JD, Morrell CH, Brant LJ, Landis PK, Fleg JL. Age-associated changes in blood pressure in a longitudinal study of healthy men and women. J Gerontol A Biol Sci Med Sci. 1997;52:M177–M183. 5. Friedlander Y, Austin MA, Newman B, Edwards K, Mayer-Davis EI, King MC. Heritability of longitudinal changes in coronary-heart-disease risk factors in women twins. Am J Hum Genet. 1997;60:1502–1512. 6. Cheng LS, Carmelli D, Hunt SC, Williams RR. Evidence for a major gene influencing 7-year increases in diastolic blood pressure with age. Am J Hum Genet. 1995;57:1169 –1177. 7. Berg K. Gene-environment interaction; Variability gene concept. In: Goldbourt U, de Faire U, berg K, eds. Genetic Factors in Coronary Heart Disease. Dordrecht: Kluwer Academic Publishers; 1994:373–383. 8. Kupper LL. Effects of the use of unreliable surrogate variables on the validity of epidemiologic research studies. Am J Epidemiol. 1984;120: 643– 648. 9. Davis CE, Rifkind BM, Brenner H, Gordon DJ. A single cholesterol measurement underestimates the risk of coronary heart disease. An empirical example from the Lipid Research Clinics Mortality Follow-Up Study. JAMA. 1990;264:3044 –3046. 10. Levy D, DeStefano AL, Larson MG, O’Donnell CJ, Lifton RP, Gavras H, Cupples LA, Myers RH. Evidence for a gene influencing blood pressure on chromosome 17. Genome scan linkage results for longitudinal blood pressure phenotypes in subjects from the Framingham Heart Study. Hypertension. 2000;36:477– 483. 11. Cook NJ, Rosner BA, Chen W, Srinivasan SR, Berenson GS. Using area under the curve to predict adult blood pressure from childhood measures in the Bogalusa Heart Study. Stat Med. 2004;23:3421–3435. 12. Jacobs KB, Gray-McGuire C, Cartier KC, Elston RC. Genome-wide linkage scan for genes affecting longitudinal trends in systolic blood pressure. BMC Genet. 2003;4(Suppl 1):S82–S86. 13. Pinnaduwage D, Beyene J, Fallah S. Genome-wide linkage analysis of systolic blood pressure slope using the Genetic Analysis Workshop 13 data sets. BMC Genet. 2003;4(Suppl 1):S86 –S91. 14. The Bogalusa Heart Study 20th Anniversary Symposium. Am J Med Sci. 1995;310:S1–S138. Chen et al Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 15. Berenson GS, McMahan CA, Voors AW, Webber LS, Srinivasan SR, Frank GC, Foster TA, Blonde CV. Cardiovascular Risk Factors in Children. The Early Natural History of Atherosclerosis and Essential Hypertension. Oxford: Oxford University Press; 1980. 16. Elkasbany AM, Urbina EM, Daniels SR, Berenson GS. Prediction of adult blood pressure by K4 and K5 diastolic blood pressure in children: the Bogalusa Heart Study. J Pediatr. 1998;132:687– 692. 17. SAS Institute: SAS/STAT Software: Changes and Enhancements through Release 6.12. Cary NC: SAS Institute; 1997. 18. Chen W, Li S, Cook NR, Rosner B, Srinivasan SR, Boerwinkle E, Berenson GS. An Autosomal Genome Scan for Loci Linked to Longitudinal Burden of Body Mass Index from Childhood to Young Adulthood in White Sibships: The Bogalusa Heart Study. Int J Obesity. 2004;28: 462– 469. 19. S.A.G.E. (2002). Statistical Analysis for Genetic Epidemiology, Release 4.3. Computer program package available from the Department of Epidemiology and Biostatistics, Case Western Reserve University, Cleveland, Ohio. 20. Almasy L, Blangero J. Multipoint quantitative-trait linkage analysis in general pedigrees. Am J Hum Genet. 1998;62:1198 –1211. 21. SOLAR. (2001). Squential Oligogenic Linkage Analysis Routine. Computer program package available from the Department of Genetics, Southwest Foundation for Biomedical Research, San Antonio, Texas. 22. Lander E, Kruglyak L. Genetic dissection of complex traits: Guidelines for interpreting and reporting linkage results. Nat Genet. 1995;11: 241–247. 23. Morrison AC, Cooper R, Hunt S, Lewis CE, Luke A, Mosley TH, Boerwinkle E. Genome scan for hypertension in nonobese African Americans: the National Heart, Lung, and Blood Institute Family Blood Pressure Program. Am J Hypertens. 2004;17:834 – 838. 24. Allayee H, de Bruin TW, Michelle Dominguez K, Cheng LS, Ipp E, Cantor RM, Krass KL, Keulen ET, Aouizerat BE, Lusis AJ, Rotter JI. Genome scan for blood pressure in Dutch dyslipidemic families reveals linkage to a locus on chromosome 4p. Hypertension. 2001;38:773–778. 25. Kristjansson K, Manolescu A, Kristinsson A, Hardarson T, Knudsen H, Ingason S, Thorleifsson G, Frigge ML, Kong A, Gulcher JR, Stefansson K. Linkage of essential hypertension to chromosome 18q. Hypertension. 2002;39:1044 –1049. 26. Angius A, Petretto E, Maestrale GB, Forabosco P, Casu G, Piras D, Fanciulli M, Falchi M, Melis PM, Palermo M, Pirastu M. A new essential Genetic Loci for Blood Pressure Since Childhood 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 959 hypertension susceptibility locus on chromosome 2p24 –p25, detected by genomewide search. Am J Hum Genet. 2002;71:893–905. Atwood LD, Samollow PB, Hixson JE, Stern MP, MacCluer JW. Genome-wide linkage analysis of blood pressure in Mexican Americans. Genet Epidemiol. 2001;20:373–382. Barkley RA, Chakravarti A, Cooper RS, Ellison RC, Hunt SC, Province MA, Turner ST, Weder AB, Boerwinkle E; Family Blood Pressure Program. Positional identification of hypertension susceptibility genes on chromosome 2. Hypertension. 2004;43:477– 482. Krushkal J, Ferrell R, Mockrin SC, Turner ST, Sing CF, Boerwinkle E. Genome-wide linkage analyses of systolic blood pressure using highly discordant siblings. Circulation. 1999;99:1407–1410. Hsueh WC, Mitchell BD, Schneider JL, Wagner MJ, Bell CJ, Nanthakumar E, Shuldiner AR. QTL influencing blood pressure maps to the region of PPH1 on chromosome 2q31–34 in Old Order Amish. Circulation. 2000;101:2810 –2816. Rice T, Rankinen T, Province MA, Chagnon YC, Perusse L, Borecki IB, Bouchard C, Rao DC. Genome-wide linkage analysis of systolic and diastolic blood pressure: the Quebec Family Study. Circulation. 2000; 102:1956 –1963. Rice T, Rankinen T, Chagnon YC, Province MA, Perusse L, Leon AS, Skinner JS, Wilmore JH, Bouchard C, Rao DC. Genomewide linkage scan of resting blood pressure: HERITAGE Family Study. Health, Risk Factors, Exercise Training, and Genetics. Hypertension. 2002;39: 1037–1043. Cooper RS, Luke A, Zhu X, Kan D, Adeyemo A, Rotimi C, Bouzekri N, Ward R, Rorimi C. Genome scan among Nigerians linking blood pressure to chromosomes 2, 3, and 19. Hypertension. 2002;40:629 – 633. Zhu DL. Wang HY, Xiong MM, He X, Chu SL, Jin L, Wang GL, Yuan WT, Zhao GS, Boerwinkle E, Huang W. Linkage of hypertension to chromosome 2q14 – q23 in Chinese families. J Hypertens. 2001;19: 55– 61. Bianchi G, Tripodi G. Genetics of hypertension: the adducin paradigm. Ann N Y Acad Sci. 2003;986:660 – 668. Rutherford S, Johnson MP, Griffiths LR. Sibpair studies implicate chromosome 18 in essential hypertension. Am J Med Genet. 2004;126A: 241–247. Felder RA, Sanada H, Xu J, Yu P-Y, Wang Z, Watanabe H, Asico LD, Wang W, Zheng S, Yamaguchi I, Williams SM, Gainer J, Brown NJ, Hazen-Martin D, Wong LJC, Robillard JE, Carey RM, Eisner GM, Jose PA. G protein-coupled receptor kinase 4 gene variants in human essential hypertension. Proc Nat Acad Sci. 2002;99:3872–3877. Autosomal Genome Scan for Loci Linked to Blood Pressure Levels and Trends Since Childhood: The Bogalusa Heart Study Wei Chen, Shengxu Li, Sathanur R Srinivasan, Eric Boerwinkle and Gerald S. Berenson Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 Hypertension. 2005;45:954-959; originally published online April 4, 2005; doi: 10.1161/01.HYP.0000161881.02361.11 Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2005 American Heart Association, Inc. All rights reserved. Print ISSN: 0194-911X. Online ISSN: 1524-4563 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://hyper.ahajournals.org/content/45/5/954 Data Supplement (unedited) at: http://hyper.ahajournals.org/content/suppl/2006/09/04/01.HYP.0000161881.02361.11.DC1 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Hypertension is online at: http://hyper.ahajournals.org//subscriptions/ Appendix Figure Legend Multipoint linkage results for total and incremental AUC for blood pressure in white siblings on chromosomes 1 to 22: The Bogalusa Heart Study AUC=area under the curve (mmHg) divided by the number of follow-up years. Total AUC was adjusted for age, sex and BMI; incremental AUC for age, sex, BMI and baseline blood pressure. 4 Total AUC SBP Incremental AUC 3 Chromosome 1 2 LOD Score 1 0 4 DBP 3 2 1 0 0 50 100 150 Location (cM) Figure I 200 250 300 4 Total AUC Incremental AUC SBP 3 Chromosome 2 2 LOD Score 1 0 4 DBP 3 2 1 0 0 Figure II 100 Location (cM) 200 300 4 Total AUC SBP Incremental AUC 3 Chromosome 3 2 LOD Score 1 0 4 DBP 3 2 1 0 0 50 100 150 Location (cM) Figure III 200 250 4 Total AUC SBP Incremental AUC 3 Chromosome 4 2 LOD Score 1 0 4 DBP 3 2 1 0 0 Figure IV 50 100 Location (cM) 150 200 4 Total AUC Incremental AUC SBP 3 Chromosome 5 2 LOD Score 1 0 4 DBP 3 2 1 0 0 50 100 Location (cM) Figure V 150 200 4 Total AUC Incremental AUC SBP 3 Chromosome 6 2 LOD Score 1 0 4 DBP 3 2 1 0 0 50 100 Location (cM) Figure VI 150 200 4 Total AUC Incremental AUC SBP 3 Chromosome 7 2 LOD Score 1 0 4 DBP 3 2 1 0 0 Figure VII 50 100 Location (cM) 150 200 4 Total AUC Incremental AUC SBP 3 Chromosome 8 2 LOD Score 1 0 4 DBP 3 2 1 0 0 50 100 Location (cM) Figure VIII 150 200 4 Total AUC Incremental AUC SBP 3 Chromosome 9 2 LOD Score 1 0 4 DBP 3 2 1 0 0 50 100 Location (cM) Figure IX 150 200 4 Total AUC Incremental AUC SBP 3 Chromosome 10 2 LOD Score 1 0 4 DBP 3 2 1 0 0 50 100 Location (cM) Figure X 150 200 4 Total AUC Incremental AUC SBP 3 Chromosome 11 2 LOD Score 1 0 4 DBP 3 2 1 0 0 50 100 Location (cM) Figure XI 150 4 Total AUC Incremental AUC SBP 3 Chromosome 12 2 LOD Score 1 0 4 DBP 3 2 1 0 0 50 100 Location (cM) Figure XII 150 200 4 Total AUC Incremental AUC SBP 3 Chromosome 13 2 LOD Score 1 0 4 DBP 3 2 1 0 0 50 100 Location (cM) Figure XIII 150 4 Total AUC Incremental AUC SBP 3 Chromosome 14 2 LOD Score 1 0 4 DBP 3 2 1 0 0 50 100 Location (cM) Figure XIV 150 4 Total AUC Incremental AUC SBP 3 Chromosome 15 2 LOD Score 1 0 4 DBP 3 2 1 0 0 50 100 Location (cM) Figure XV 150 4 Total AUC Incremental AUC SBP 3 Chromosome 16 2 LOD Score 1 0 4 DBP 3 2 1 0 0 50 100 Location (cM) Figure XVI 150 4 Total AUC Incremental AUC SBP 3 Chromosome 17 2 LOD Score 1 0 4 DBP 3 2 1 0 0 50 100 Location (cM) Figure XVII 150 4 Total AUC SBP Incremental AUC 3 Chromosome 18 2 LOD Score 1 0 4 DBP 3 2 1 0 0 Figure XVIII 50 100 Location (cM) 150 4 Total AUC SBP Incremental AUC 3 Chromosome 19 2 LOD Score 1 0 4 DBP 3 2 1 0 0 Figure XIX 50 100 Location (cM) 150 4 Total AUC SBP Incremental AUC 3 Chromosome 20 2 LOD Score 1 0 4 DBP 3 2 1 0 0 Figure XX 25 50 Location (cM) 75 100 4 Total AUC SBP Incremental AUC 3 Chromosome 21 2 LOD Score 1 0 4 DBP 3 2 1 0 0 Figure XXI 10 20 30 Location (cM) 40 50 4 Total AUC SBP Incremental AUC 3 Chromosome 22 2 LOD Score 1 0 4 DBP 3 2 1 0 0 Figure XXII 10 20 30 Location (cM) 40 50