Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
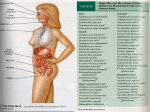
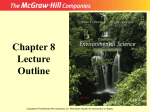
Lowering the Toxic Body Burden Using Diet, Lifestyle, and Other Strategies Dan Lukaczer, ND Applying Functional Medicine in Clinical Practice London, England October 2015 ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine etelling the Patient’s Story Physiology and Function: Organizing the Patient’s Clinical Imbalances Antecedents Assimilation Defense & Repair (Predisposing FactorsGenetic/Environmental) (e.g., Digestion, Absorption, Microbiota/GI, Respiration) (e.g., Immune, Inflammation, Infection/Microbiota) Triggering Events (Activators) Structural Integrity Energy (e.g., from Subcellular Membranes to Musculoskeletal Structure) (e.g., Energy Regulation, Mitochondrial Function) Classes of Toxicants emotional cognitive regulation, grief, function, sadness, anger, perceptual patterns • Metals etc. meaning & purpose, • Persistent Organic Pollutants relationship with something e.g., e.g., e.g., greater Mediators/Perpetuators (Contributors) Spiritual Communication Biotransformation & Elimination • Biological Toxins (e.g., Endocrine, Neurotransmitters, (e.g., Toxicity, Detoxification) Transport Immune messengers) Biotransformation (e.g., Cardiovascular, Lymphatic • Electromagnetic System) & Elimination • Psych/Spiritual Personalizing Lifestyle Factors Sleep & Relaxation Nutrition & Hydration (e.g., Toxicity, Detoxification) Stress & Resilience Relationships & Networks ©2015 The2011 Institute for Functional Medicine Name:____________________________ Date:___________ CC:_____________________________________ © Copyright Institute for Functional Learning Objectives • Define what a toxicant is, outline our increasing exposure to toxins, and evaluate the health consequences of a chronic, low level toxic load • Understand the process of biotransformation or detoxification and how it may be modified • Develop competency in assessing for chronic toxicity • Develop strategies to minimise toxic exposure, increase mobilisation, biotransformation, and excretion of toxins. • Be able to implement a foundational detoxification programme ©2015 The Institute for Functional Medicine Functional Medicine & Toxicology: Fundamental Principles 1. Exposure to environmental toxins is widespread, increasing and lifelong. 2. The total body burden of these toxins can act synergistically to cause physiologic dysfunction. 3. This dysfunction can lead to chronic illnesses in susceptible individuals. 4. Susceptibility is largely defined by an individual’s ability to biotransform, detoxify and eliminate exogenous and endogenous toxins. 5. Lifestyle, diet and nutraceuticals can enhance detoxification, prevent disease and restore health. ©2015 The Institute for Functional Medicine Which patients might benefit from a focus on toxins and biotransformation? • Feels vaguely unwell & persistently fatigued • Has experienced sudden onset of autoimmune disease or chronic neurologic disorder • Is sensitive to all sorts of fumes, solvents cosmetics, and detergents • Has a personal or strong family history of cancer • Has a long history of constipation • Has a past medical history of an acute toxic exposure ©2015 The Institute for Functional Medicine What is a Toxicant? • Any substance that causes structural damage or functional disturbances. • Exposure can occur through ingestion, inhalation, absorption, injection, etc., or through internal metabolic processes. – Exogenous – Endogenous ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine Types of Exogenous Toxicants • Pesticides – Insecticides, herbicides • Industrial compounds and chemical byproducts • Volatile organics, solvents and detergents, toxic metals, plasticisers, insulators (asbestos) • • • • • • Combustion/incineration pollutants Synthetic medications or natural phytochemicals Food additives and preparation by-products Cosmetic additives Electromagnetic radiation Psycho-spiritual ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine Types of Endogenous Toxicants • Reactive oxygen and nitrogen species (hydroxyl, superoxide, peroxyl, peroxynitrite) – By-product of respiration (mitochondria) – By-product of hepatic and gastrointestinal detoxication – Response to microbial attack (oxidative burst) – Consequence of tissue ischaemia (upregulation of xanthine oxidase) • Lipid peroxides (rancid fats) • Oxidised glucose and advanced glycosylated end products (AGEs) ©2015 The Institute for Functional Medicine Types of Endogenous Toxicants Imbalanced metabolism – Major inborn errors of metabolism (enzymatic) • Homocysteinemia • Phenylketonuria – “Minor” enzymatic dysfunctions (polymorphisms) – Urea cycle abnormalities: hyperammonaemia from inability to metabolise nitrogen ©2015 The Institute for Functional Medicine Types of Endogenous Toxicants Products of dysbiosis – Bacteria: putrescine, cadaverine, ammonia, etc. – Yeasts: arabinose, tartrate, citramalate, etc. – Secondary bile acids (deconjugated) – Beta glucuronidase (elaborated by bacteria and causing enterohepatic recirculation of hormones and other toxins) ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine Increasing Exposure • Since WWII, over 85,000 synthetic chemicals have been registered with the US EPA • >140,000 chemicals are on the European market (UNEP.org) • Each year, an estimated 2,000 new chemicals are introduced for use in everyday items including foods, personal care products, prescription drugs, household cleaners, pesticides, and lawn care products ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine Body Burden: The Pollution in People Mount Sinai School of Medicine, New York http://www.ewg.org/sites/bodyburden1/es.php Laboratory tests uncovered 167 chemical pollutants in blood & urine from nine volunteers, including an average of 53 carcinogens in each person. The people tested do not work with chemicals and do not live near an industrial facility. ©2015 The Institute for Functional Medicine Bisphenol-A • Commercial plasticiser: over 8 billion pounds produced every year (lining canned food & drinks; water bottles; cash register receipts); over 100 tons released into the atmosphere every year • Readily absorbed through skin and gut mucosa • More than 90% of people in US have measurable BPA in their bodies Endocr Rev. 2009; 30(1): 75–95. ©2015 The Institute for Functional Medicine The “Exposome” Combined Exposures from All Sources That Reach the Body’s Internal Chemical Environment Science, 2010, Vol 330: 460-461 ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine Are “low” levels of toxicants (nanograms or picograms per mL) significant? ©2015 The Institute for Functional Medicine “The demonstration of biological effects at very low levels of exposure suggests that two toxicological axioms—(1) all chemicals have thresholds below which they cause no adverse effects, and (2) that ‘the dose makes the poison’— should be reevaluated.” Public Health Reports, 2002, Vol 117: 315-323 ©2015 The Institute for Functional Medicine Chronic Low-Level Toxicity • Biologic effects of many toxicants are not linear – very low doses can have profound physiologic effects • Chemical sensitivity varies considerably, depending on species, life stages, biochemical individuality and synergistic effects from multiple toxicants ©2015 The Institute for Functional Medicine How Low is Low Enough? Lead poisoning was diagnosed historically if whole-blood lead levels were found to be: 60 mcg/dl - 1960s 30 mcg/dl - 1975 25 mcg/dl - 1985 10 mcg/dl - 1991 Each 10 mcg rise in lead = fall in children’s IQ by 4.6 pts. From 1 to 10 mcg = fall in IQ by 7.4 pts. N Engl J Med 2003 Apr 17;348(16):1517-26. ©2015 The Institute for Functional Medicine Lead The understanding of lead toxicity has advanced substantially in the past 3 decades and focus has shifted from high-dose effects in clinically symptomatic individuals to the consequences of exposure at lower doses that cause no overt or apparent symptoms. More refined epidemiological techniques and better outcome measures has lowered the least observable effect level for lead until it approaches zero. Needleman H, Lead poisoning Annu Rev Med. 2004;55:209-22. ©2015 The Institute for Functional Medicine Arsenic “Long-term exposure to arsenic has been found to be associated with an increased risk of diabetes mellitus, hypertension, ischemic heart disease, and cerebral infarction in a dose-response relationship … after adjustment for other cardiovascular risk factors” Wang CH, et al., Biological gradient between long-term arsenic exposure and carotid atherosclerosis. Circulation 2002 Vol 105: 1804-1809. ©2015 The Institute for Functional Medicine Organochlorines Organochlorine insecticides produce a direct toxic action on the dopaminergic tracts of the substantia nigra and may contribute to the development of Parkinson’s Disease in those rendered susceptible by virtue of cytochrome P-450 polymorphism, excessive exposure, or other factors.” Corrigan FM, et al., Organochlorine insecticides in substantia nigra in Parkinson's disease. J Toxicol Environ Health A. 2000 Feb 25;59(4):229-34. ©2015 The Institute for Functional Medicine Bisphenol-A • Endocrine disruptor: can mimic effects of oestrogen (and other hormones) and interfere with cellular signaling • Higher levels of urinary excretion linked to diabetes, obesity, heart disease, liver inflammation • Also linked to cancer, thyroid disorders, infertility Endocr Rev. 2009; 30(1): 75–95. ©2015 The Institute for Functional Medicine PLOS One, 2014, Volume 9(10): e110509 ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine State of the Science: Endocrine Disrupting Chemicals • Many endocrine-related disorders are on the rise • The speed which the increases in disease incidence have occurred in recent decades rules out genetic factors as the sole plausible explanation • Numerous laboratory studies support the idea that chemical exposures contribute to endocrine disorders in humans and wildlife. • The most sensitive window of exposure to EDCs is during critical periods of development, such as foetal development & puberty World Health Organization, 2012 ©2015 The Institute for Functional Medicine State of the Science: Endocrine Disrupting Chemicals • Environmental chemicals can exert endocrine disrupting effects on more than just estrogen, androgen, and thyroid hormone action. Some are known to interact with multiple hormone receptors simultaneously. • Disease risk due to EDCs may be significantly underestimated. • An important focus should be on reducing exposures by a variety of mechanisms. World Health Organisation, 2012 ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine Synergistic Effects of Toxic Metals: The Sum Is Greater then the Parts • The administration of an essentially no response level (LD1) of a mercury salt together with 1/20th of the LD1 of a lead salt killed all the animals. • “Generally, a combination was synergistic when the most toxic member was present at or near its LD1 dose in the presence of a much less toxic member.” Schubert et al., Combined effects in toxicology – a rapid systematic testing procedure: cadmium, mercury and lead. J Toxicology & Environ Health 1978 4:763. ©2015 The Institute for Functional Medicine www.childenvironment.org Mount Sinai School of Medicine ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine Dave’s Chief Complaints • Weight Gain (30 lbs in last decade) – Mostly over the last 5-7 years, round the waist • • • • Elevated cholesterol and triglycerides levels Increased Blood Pressure Fatigues more easily than in past Less stamina in exercise and physical activity • Some muscle and joint stiffness ©2015 The Institute for Functional Medicine Exposures from Construction Sites and Electrical Supplies Loves to cook “foodie” Electrician; working on construction sites since mid 20s 50 52 25 54 57 Increased Triglycerides Hypertension, Incr Chol & LDL Incr glucose Weight Gain & Fatigue Avid exerciser and runner Reduced exercise Weight Gain/Inc Waist Circ Hypertension Dyslipidemia Fatigue/Reduce Stamina ©2015 The Institute for Functional Medicine Obesity Overweight VAT (Incr WHR) Hypertension Endothelial Dysfunction Erectile Dysfunction Joint Stiffness Mild Testosterone Def Insulin Resistance Metabolic Syndrome Adequate and Restful Inconsistent walking Inflammation VAT (Incr WHR) Low D InflamVascular Risks Fatigue Muscle Soreness Oxidative Stress Occupational Exposure Lead exposure Heavy Metal concern Low Glutathione Insulin Resistance Blood Sugar Elevation HTN and Met Syn Low Anti-oxidants Moving, job satisfaction, excited about Reduced Magnesium change to position for retirement , Methylation concerns happy in marriage Low B2, B6, B12, Folic Acid ©2015 The Institute for Functional Medicine Lead and CVD Circulation 2009;120:1056-1064 ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine POPs and Diabetes • Investigation of the association between diabetes prevalence and persistent organic pollutants (POPs) in 2,016 adult participants in the NHANES 1999-2002. • After adjustment for age, sex, race, ethnicity, poverty income ratio, BMI, and waist circumference, diabetes prevalence was strongly associated with lipid-adjusted serum concentrations of all six POPs tested. • Participants were classified according to the sum of the six POPs. The adjusted odds ratios for risk of diabetes and sum POPs was 1.0, 14.0, 14.7, 38.3, and 37.7 Lee et. al., A strong dose-response relation between serum concentrations of persistent organic pollutants and diabetes: results from the National Health and Examination Survey 1999-2002. Diabetes Care. 2006 Jul;29(7):1638-44. ©2015 The Institute for Functional Medicine POPs and Diabetes • 749 nondiabetics were assessed for 19 POPs • POPs detectable in > or = 60% of participants. • Among subclasses, organochlorine (OC) pesticides were most strongly associated with HOMA-IR (a measure of insulin resistance. • POPs may be associated with type 2 diabetes risk by increasing insulin resistance, and POPs may interact with obesity to increase the risk of type 2 diabetes. Lee et. al., Association between serum concentrations of persistent organic pollutants and insulin resistance among nondiabetic adults: results from the National Health and Nutrition Examination Survey 1999-2002. Diabetes Care. 2007 Mar;30(3):622-8. ©2015 The Institute for Functional Medicine Conclusions: There is Plausible Evidence to Link Toxic Exposure with Risk of: • Selected cancers • Autoimmune disease • Neurological diseases: ALS, Parkinson’s disease, Alzheimer’s disease • Neuropsychiatric illnesses: depression, anxiety, inattention, hyperactivity • Chronic fatigue syndrome, fibromyalgia, multiple chemical sensitivity • Allergies, asthma • Cardiovascular disease ©2015 The Institute for Functional Medicine Conclusions: Chronic Toxicant Exposure may: • Amplify other pathological processes • Create or contribute to a wide variety of chronic diseases • Lead to toxicant-induced loss of tolerance ©2015 The Institute for Functional Medicine “We are what we….. Eat Drink Breathe Touch …and can’t Eliminate ©2015 The Institute for Functional Medicine TOTAL TOXIC LOAD results from Total Toxic Exposure minus Ability to Biotransform and Excrete Toxins ©2015 The Institute for Functional Medicine From. Larry Needham, PhD: CDC NCEH Presentation (2004) ©2015 The Institute for Functional Medicine Learning Objectives • Define what a toxicant is, outline our increasing exposure to toxins, and evaluate the health consequences of a chronic, low level toxic load. • Understand the process of biotransformation or detoxification and how it may be modified. • Develop competency in assessing for chronic toxicity. • Develop strategies to minimise toxic exposure, increase mobilisation, biotransformation, and excretion of toxins. • Be able to implement a foundational detoxification programme. ©2015 The Institute for Functional Medicine Detoxification Chemical changes of a xenobiotic, phytochemical or endogenous compound that render it less toxic and/or more readily excreted. ©2015 The Institute for Functional Medicine “Detoxification is central to understanding functional assessment in medicine, not so much because we live in a toxic environment but because detoxification is the biggest item in each individual’s biochemical budget. “It handles waste not only from our environment, but from every process in all the organs and systems of the body.” Sidney Baker, MD Detoxification and Healing ©2015 The Institute for Functional Medicine How are toxicants transformed and eliminated from the body? Biotransformation The process of chemically modifying a substance to render it less toxic and more readily excreted in the urine or stool. Biotransformation occurs with both exogenous and endogenous compounds. ©2015 The Institute for Functional Medicine Biotransformation is… • A constantly active process • ATP (energy) dependent • Highly nutrient dependent • Polymorphic: marked inter-individual variability ©2015 The Institute for Functional Medicine Biotransformation is… • Inducible by toxicants, drugs, phytochemicals • Additive (e.g. affected by total load) • Redundant (multiple substrates processed through same pathways) ©2015 The Institute for Functional Medicine Cellular Biotransformation: Xenobiotics, Phytochemicals & Endogenous Compounds • Hydrophilic compounds: readily excreted in urine and/or bile. • Lipophilic compounds: must be chemically altered into hydrophilic compounds to facilitate elimination. ©2015 The Institute for Functional Medicine Cellular Biotransformation of Lipophilic Compounds Process of detoxication typically involves two steps: – Phase I bioactivation (“functionalisation”) – Phase II conjugation ©2015 The Institute for Functional Medicine Types of Reactions Parent Compound Activated Intermediate WaterSoluble Compound Phase I Phase II Cytochrome P450 enzymes: Oxidation Reduction Hydrolysis Glucuronosyl Transferase (UGT) Sulfo-transferases (SULT) Amino Acid Conjugation Glutathione Conjugation Acetylation Methylation ©2015 The Institute for Functional Medicine Enzymatic Biotransformation • Phase I & II enzymes are highly polymorphic: considerable individual variation in activity based on genotype • Phase I & II enzymes can be induced or inhibited by diet, chemical compounds and hormones • Upregulation of phase I relative to phase II can increase production of highly toxic compounds • Upregulation of phase II leads to elimination of toxins ©2015 The Institute for Functional Medicine Cellular Biotransformation of Lipophilic Compounds • All tissues have some activity • Majority of reactions occur in liver • Relatively high activity in GI tract, lungs, kidneys, skin, and blood brain barrier ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine Intestinal bacteria play a major role in biotransformation and detoxification and may explain some of the differences in xenobiotic metabolism between individuals Mol Nutr Food Res. 2013 Jan;57(1):84-99 ©2015 The Institute for Functional Medicine Phase I Reactions • Introduce or expose a functional group on the parent compound; • Making it more polar. • May activate inert compounds (e.g. pro-drugs & pro-carcinogens) ©2015 The Institute for Functional Medicine Cytochrome P450 Mono-oxygenases The Primary Phase I Enzyme System Activity in humans includes over 200,000 substrates: – Pharmaceuticals – Xenobiotics – Phytochemicals – Cholesterol, steroids, eicosanoids, retinoids, vitamin D ©2015 The Institute for Functional Medicine Relative contribution of CYP450 enzymes to known drug metabolism ©2015 The Institute for Functional Medicine CYP450 Phenotypic Variability • Activity can range from 5 fold in constitutive expression to 400 fold as result of drug interactions • Genetic polymorphisms can result in increased, decreased or null activity ©2015 The Institute for Functional Medicine CYP450: Inhibition • Phase I inhibition can increase blood levels of a drug or hormone • A major cause of drug-drug and drugphytochemical interactions ©2015 The Institute for Functional Medicine CYP450 Inhibitors • • • • • • • • Cimetidine: multiple enzymes Antifungal medications SSRIs (fluoxetine, paroxetine, fluvoxamine) Grapefruit juice (furanocoumarins): CYP3A4 Berberine: CYP2D6, CYP3A4, CYP2C9 Green tea catechins: CYP1A1, 1A2, 1B1 Garlic: CYP2E1 Star fruit juice: CYP2A6, CYP1A2, CYP3A4 ©2015 The Institute for Functional Medicine CYP450 Induction • Phase I induction can decrease blood levels of a drug or hormone • Commonly induced enzymes: CYP 1A; CYP1B1; CYP2E1 • Occurs by upregulation of transcription • Imbalanced induction (phase 1 > phase 2), may result in pathological detoxification • Result is increased risk of cancer and inflammatory disease ©2015 The Institute for Functional Medicine Phase II Reactions • Covalent linkage between parent compound functional group and water-soluble moiety • Product generally inactive and excreted via bile or urine ©2015 The Institute for Functional Medicine Phase II Enzymes • Resulting conjugates are highly polar, usually inactive & rapidly excreted in urine and/or feces (through biliary route) • High molecular weight conjugates excreted in bile are subject to enzymatic cleavage by intestinal microflora, allowing enterohepatic recirculation (e.g. oestrogen, organochlorines) ©2015 The Institute for Functional Medicine Phase II Enzymes: Conjugating Reagents • Glucuronic acid (uridine-diphosphateglucuronosyltransferases: UGT) • Sulfate (sulfonyltransferases: SULT) • Glutathione (gluthathione-S-transferases: GST) • Acetate (N-acetyltransferases: NAT) • Amino acids (taurine, glycine, glutamine) • Methyl group (methyltransferases; e.g. COMT) ©2015 The Institute for Functional Medicine Phase II Enzymes • Under basal conditions, Phase II enzymes do not operate at maximum capacity • Phase II activity (UGT, GST, NQO1) can be substantially increased by genetic induction, primarily via Nrf2/ARE pathway • SNPs in Phase II (UGT, SULT) affect individual susceptibility to toxicants and drugs • Supporting Phase II conjugation is an effective strategy for protection against chronic disease • Objective is to induce Phase II enzymes with minimal effects on Phase I ©2015 The Institute for Functional Medicine Imbalanced Detoxification Non-Polar Xenobiotic Phase I Phase II CYP P450 Conjugation Reactive Intermediate Inert Water-Soluble Metabolite Damage to DNA, RNA, Proteins ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine Why some people retain toxins, or are more sensitive to toxins 1. 2. 3. 4. 5. 6. 7. 8. 9. Overwhelming toxic load Poor biotransformation/elimination Polymorphisms in phase I & II enzymes Intestinal dysbiosis Nutrient deficiencies High sugar, low protein diets Oxidative stress Chronic inflammation Stress, emotional trauma ©2015 The Institute for Functional Medicine Learning Objectives • Define what a toxicant is, outline our increasing exposure to toxins, and evaluate the health consequences of a chronic, low level toxic load • Understand the process of biotransformation or detoxification and how it may be modified • Develop competency in assessing for chronic toxicity • Develop strategies to minimise toxic exposure, increase mobilisation, biotransformation, and excretion of toxins. • Be able to implement a foundational detoxification programme. ©2015 The Institute for Functional Medicine Assessing Chronic Toxicity: History • Exposome history • Home & work environment • Diet & Lifestyle • Medical Symptoms questionnaire (MSQ) • Toxicity Exposure Questionnaires (TEQ) • History of reactions to drugs, chemicals, odours, etc. ©2015 The Institute for Functional Medicine How Many People Are We Talking About? Chemical intolerance occurs in 1 of 5 primary care patients yet is rarely diagnosed by busy practitioners. Chemical Intolerance in Primary Care Settings: Prevalence, Comorbidity, and Outcomes Ann Fam Med, 2012, Vol 10: 357-365 ©2015 The Institute for Functional Medicine Medical Symptoms Questionnaire (MSQ) 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. HEAD EYES EARS NOSE MOUTH/THROAT SKIN HEART LUNGS DIGESTIVE TRACT JOINTS/MUSCLE WEIGHT ENERGY/ACTIVITY MIND EMOTIONS OTHER 71 questions Scored: 0 – 4 Total: 0 – 284 ©2015 The Institute for Functional Medicine Toxin Exposure Questionnaire (TEQ) Exposure Sources: • • • • • • Community Home Occupational Hobbies Diet & Lifestyle Medical/Dental ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine How Toxic are You? • Take out the TEQ-20 that is in your folder and complete it for yourself • Then discuss with your group members ©2015 The Institute for Functional Medicine Intake & Medical History Key Questionnaires TEQ MSQ Environmental Exposures Known Toxic Exposures: Occupational, Lifestyle, Residential, Medical? FUNCTIONAL LAB TESTS Nutritional & Assimilation Physical Exam & Conventional Labs Patient Sensitivity Level Toxicity Signs/Symptoms? Nutritional Deficiencies? Detox & Elim. Capacity? Toxic Damage Genetic Body Burden Susceptibility Review of Findings & Intervention Programme ©2015 The Institute for Functional Medicine Assessing Chronic Low-level Toxicity • Physical findings • Markers of increased susceptibility (SNPs) • Markers of toxic damage • Oxidative stress • GGT • Direct measurement of toxins ©2015 The Institute for Functional Medicine Assessing Toxicity • Identify triggers – Toxic metals: hair, blood, urine analysis pre and post DMSA challenge – Organic toxicants (fat biopsy; blood, urine) – Stool analysis – Hepatic detoxification and oxidative stress profiles – Intestinal permeability testing • Identify mediators – Extra and intracellular antioxidant level – Oxidative stress markers – Essential fatty acid profile ©2015 The Institute for Functional Medicine Learning Objectives • Define what a toxicant is, outline our increasing exposure to toxins, and evaluate the health consequences of a chronic, low level toxic load • Understand the process of biotransformation or detoxification and how it may be modified • Develop competency in assessing for chronic toxicity • Develop strategies to minimise toxic exposure, increase mobilisation, biotransformation, and excretion of toxins. • Be able to implement a foundational detoxification programme. ©2015 The Institute for Functional Medicine Functional Medicine Strategies for Living in a Toxic World 1. Minimise exogenous toxic exposure 2. Optimise bowel health, mobilisation and excretion of toxins 3. Optimise balanced Phase I and II biotransformation of toxins ©2015 The Institute for Functional Medicine Strategy 1 Minimise Toxic Exposure ©2015 The Institute for Functional Medicine Top Ten Lifestyle Choices to Decrease Toxin Exposure 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. Avoid using pesticides/herbicides in home and garden Filter water with R/O and carbon filter Use non-toxic cleaning agents Use nontoxic building materials & carpets whenever possible in any project or remodel Use “natural” cosmetics, nail polish and fragrances Consider ‘organic whenever possible’ in food, but prioritise organic meat and dairy. Be careful with consumption of large predator fish. Do not get amalgam fillings and/or consider removal Avoiding living near high tension power lines Clean furnace filters regularly; consider HEPA filter ©2015 The Institute for Functional Medicine Reducing Exposures to Harmful Chemicals Daily Activity Questionnaire Patient Nameto _______________________________________________________________ Date___________________ Exposure potentially harmful chemicals on a daily basis is virtually unavoidable. The majority of the 85,000 chemicals registered for production under the U.S. Toxic Substances Control Act Please check the one best response for each activity described below: 1 (TSCA) were grandfathered in with little or no health and safety testing. Medical conditions linked to toxic chemicals include obesity, metabolic syndrome, diabetes, cardiovascular disease, SEDENTARY BE HAVIOR Alzheimer’s and Parkinson’s, cancers, and complaints such as fibromyalgia and t ofmultisystem the day o 1 Mos 2 multiple chemical sensitivities. Sitting while watching TV, at o 2 Half of the day a computer, driving, talking on the phone, or reading o 3 Some of the day 4 Rarely Tota l _________ o are Ten categories of toxic chemicals known to be especially prevalent, persistent, and detrimental to human and environmental health: ACTIVITIES OF DAILY LIVING o 1 Need some assistance 1. heavy metals: lead (Pb), o mercury arsenic (As), cadmium (Cd), aluminum (Al) 2 Slight(Hg), dif culty Bathing, dressing, feeding 2. polycyclic self, toilet aromatic hydrocarbons (PAHs) dif culty o 3 Minimal 3. plastics (phthalates) Tota l _________ o 4 No problem 4. phenols, particularly bisphenol A (BPA) LAUNDR Y o 1 Unable 5. organochloride pesticides (OCs) o 2 Occasionally 6. organophosphate pesticides (OPs) o 3 Regularly in small steps or with help 7. polychlorinated dibenzo-dioxin & furanwithout (dioxins) help Tota l _________ o 4 Regularly 8. polychlorinated biphenyls (PCBs) COOKING 1 Unable 9. polybrominated diphenyl o ethers (PBDEs) Take-out, breakfast, or simple lunch only o 2(PFCs) 10. polyfluorinated compounds o o 3 4 Simple microwave or crockpot meal Regular meals o 2 0-1 per day Tota l _________ Reducing Dietary Exposures HOUS KEEPING organic and low-fat 1. EChoose no-fat animal products such as dairy, eggs, meats (PAHs, o 1orUnable 2 Light dusting, straighten up o PBDEs). OCs, OPs, dioxins, PCBs, 3 Regular housekeeping small steps or with help 2. Choose cooking methodsothat are low-char and in that allow animal fats to drip away, such 4 Fully capable PCBs, PBDEs) Tota l _________ o OPs, as steaming. (PAHs, OCs, dioxins, 3. Consult local wildlife agencies before eating freshwater fish (PCBs, dioxins, PBDEs). GR OCE RY SHOPPING o 1 Unable 4. Never eat farmed salmono(PCBs), avoid eating larger carnivorous fish (Hg, PBDEs, 2 Occasional (once or twice per month) PCBs) and use the Environmental Working (EWG) Good Seafood Guide.3 but withGroup assistance o 3 Frequent, problem Tota l _________ o 4 Nosteel 5. Use glass, ceramic, or stainless containers for heating and storing hot food. (phthalates). SOCIAL ACTIVITIES o 1 Unable 6. Avoid plastic water bottles, travel mugs and bladder-style hydration reservoirs and do Church, temple, o 2 Infrequently not wash plastic food or beverage containers under high heat (phthalates). family and friends (once or twice per month) o 3 Occasionally 7. Avoid using vinyl cling wrap do only buy canned foods that are BPA-free. (BPA). Frequently (weekly or more often) Tota l _________ o 4and 8. Avoid high-fructose corn syrup and rice syrup (As) and processed foods containing BHT, DRIVING 1 Unable o artificial colorings and sweeteners. BHA, benzoate, sulfites, and Very limited o 2 organic 9. Choose local, seasonal, and produce whenever possible. Wash all fruits and o 3 Cautious, local trips vegetables using mild additive-free soap and clean water (OCs, OPs). Tota l _________ o 4 Distant trips or traf c 10. Choose organic versions of the EWG “Dirty Dozen” list of high-pesticide produce. (OCs, ERRANDS OR4LIGHT CHORES OPs). o 1 None Post of ce, drop of a child o 3 2-3 per day Reducing Home & Office Exposures 4 No or few restrictions l _________ o Water 1. Consult the EWG Drinking Database5 and consider testing your waterTota supply. Use a NSF-certified water filter if indicated (Pb, As, Cd, trihalomethane, atrazine, benzene, Grand Tota l _________ etc.). 2. Clear standing water out of plumbing lines in your home or office by flushing the toilet or Version 4 © 2015 The Institute for Functional Medicine letting the tap run for several minutes before pouring out tap water for consumption (Pb, other metals). 3. Filter shower water (chlorine, OCs), and don't buy new vinyl shower curtains (phthalates). 4. Filter air in your bedroom and office using filters, ionizers or plants.6 (airborne toxins). ©2015 The Institute for Functional Medicine Strategy 2 Optimise bowel health, mobilisation and excretion of toxins ©2015 The Institute for Functional Medicine Optimising Bowel Health • For allergic or vulnerable individuals: • Oligoantigenic diets • Nutrient dense functional foods • Bowel rehabilitation programme (5R) ©2015 The Institute for Functional Medicine Utilising the 5R Bowel Programme for Detoxification • • • • Remove pathogens Replace enzymes & hydrochloric acid Repair damaged intestinal mucosa Re-inoculate with – Prebiotics (arabinogalactan, inulin) – Probiotics • Rebalance ©2015 The Institute for Functional Medicine Agents That Repair Intestinal Mucosa • Probiotics • Plant fibres • L-glutamine – 5-15 grammes daily • Arabinogalactan (Western Larch bark) – 2-10 grammes daily ©2015 The Institute for Functional Medicine Agents That Repair Intestinal Mucosa • Aloe vera mucopolysaccharides – 100-500 mg daily • Licorice root (deglycyrrhizinated) – 500-2000 mg daily • Bovine colostrum – 5-15 grammes daily ©2015 The Institute for Functional Medicine Enhancing Mobilization and Excretion of Toxins • Exercise and Saunas = sweat • Polysaccharides from algae & seaweeds – Chlorella pyrenoidosa – Fucus (bladderwrack) – Laminaria (kelp) • D-glucaric acid • Cholegogues and cholerectics ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine Physiologic Effects of Sauna • Increases peripheral circulation. • Decreases circulation to muscles, kidney and viscera. • Increases metabolic rate. • Increases O2 consumption. ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine “These results suggest that the administration of nori prevented dioxin from being efficiently absorbed and reabsorbed from the gastrointestinal tract, and might be useful for protecting humans exposed to dioxin from ill effects.” Biosci Biotechnol Biochem, 2002, 66(11): 2306-2313 ©2015 The Institute for Functional Medicine Cracked-Cell Chlorella • Studied extensively in Japan, where it is widely used as nutritional supplement (1000 tons produced per year). • Increases excretion of: – – – – Lead Cadmium Uranium Mercury • Accelerates elimination of chlorinated hydrocarbons: – PCBs – Chlordecone (Kepone) ©2015 The Institute for Functional Medicine Beta-glucuronidase and Elimination of Toxins Toxins Conjugation (Glucuronosyl Transferase) Carcinogens Made Harmless Tumour Promoters Deconjugation Excretion from Body Steroid Hormones Sterols Deconjugation by (β-Glucuronidase) D-Glucarate ©2015 The Institute for Functional Medicine Beta Glucuronidase • Salvage enzyme that recycles conjugated compounds • Found in tissues throughout the body, concentration varies with each individual • High levels associated with increased cancer risk (esp. breast) • Elevated levels found with – dysbiosis (GI) – exposure to xenobiotics (cigarette smoke, PAHs, nitrosamines) ©2015 The Institute for Functional Medicine D-glucaric acid (Calcium or Potassium D-glucarate) • Found in cruciferous vegetables, citrus, apples, apricots, bean sprouts & cherries • Inhibits beta-glucuronidase • Regulates blood levels of bile acids & steroid hormones • Protects against cancer of breast, prostate, lung, colon, bladder, & skin (animal studies) • Dosage: 500-1000 mg tid ©2015 The Institute for Functional Medicine Oregon Grape Root ©2015 The Institute for Functional Medicine Cholagogues & Cholerectics: Enhancing Secretion of Toxins by Increasing Bile Flow • • • • • • • • Berberine (Coptis chinensis) Coffee Turmeric (Curcumin) Milk thistle Globe Artichoke Greater Celandine Dandelion Taurine ©2015 The Institute for Functional Medicine Strategy 3 Optimise balanced Phase I and II biotransformation of toxins ©2015 The Institute for Functional Medicine Overload Phase I? ©2015 The Institute for Functional Medicine Nutritional & Phytochemical Support for Assisted Biotransformation • Adequate protein source for enzyme production • Conjugant precursors for phase II reactions • Enzymatic cofactors for phase I & II • Transcription inducers of phase II enzymes ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine Phase 2 Response from Fruits/Vegetables Apples Oranges Lemons Grapefruit Pears Rhubarb Mango Avocado Peach Nectarine Grapes Dates Figs Apricot Spinach Beets Lettuce Chicory Mizuna Corn Peas Carrots Potato Tomato Blueberries Raspberries Plum Pumpkin Squash Green Beans Watermelon Canteloupe Honeydew Strawberries Oregano Basil Cardamon Cinnamon Cloves Pepper Noni Juice Collards Turnips Leeks Garlic Chives Onion Broccoli Watercress Cauliflower Cabbage Brussels Sprouts Arugula Kale Kohlrabi Daikon Red Radish Horseradish Chinese Cabbage Bok Choy ©2015 The Institute for Functional Medicine Phase II Enzyme Inducers • Glucosinolates – Sulforaphane – Phenylethylisothiocyanate (watercress) – Di-indolylmethane (active form of I3C) • Flavonoids – Ellagic acid – Green tea catechins ©2015 The Institute for Functional Medicine Phase II Enzyme Inducers • Organosulphur compounds – Garlic – NAC, glutathione • • • • • Curcuminoids (turmeric) Milk Thistle (silymarin) Artichoke (cynarin) Rosemary (carnosol) Monoterpenes (citrus peel, cherries) ©2015 The Institute for Functional Medicine Sulforaphane • Discovered in 1992 at Johns Hopkins • Over 560 scientific papers now published • Glucoraphanin precursor found in broccoli (sprouts & seeds), Brussels sprouts & kale • Potent transcription inducer of phase II detoxification & antioxidant enzymes: – GST transferases – Epoxide hydrolases – Quinone reductases – Glucuronosyl transferases ©2015 The Institute for Functional Medicine Glucosinolates • Precursors to bioactive isothiocyanates (ITC) – Often hydrolysed to ITC by enzyme myrosinase – or converted by gut flora (Phenylethyl ITC ) – Include indole-3-carbinol, Diindolylmethane and sulphorphane • Rich sources include broccoli & watercress, but all crucifers contain glucosinolates • Bifunctional modulators – Inhibition of specific phase I enzymes – Induction of phase II enyzmes • Glucuronosyltransferases • Glutathione-S-transferases ©2015 The Institute for Functional Medicine Cooked or Raw? isothiocyanate production is more extensive after consumption of raw vegetables but that isothiocyanates still arise, albeit to a lesser degree, when cooked vegetables are consumed. ©2015 The Institute for Functional Medicine Turmeric (Curcuma Longa) ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine Cofactors That Support Phase II Conjugation • • • • • • Glycine Taurine Glutamine Sodium sulfate Pantothenic acid Magnesium Methylators: – Methylfolate – Methylcobalamin – Trimethylglycine – SAMe – Phosphatidylcholine ©2015 The Institute for Functional Medicine Nutrition and Cellular Protection • Increasing evidence indicates that anti- inflammatory nutrients, in particular dietary long-chain omega-3 polyunsaturated fatty acids and plant-derived flavonoids, can be used as a therapeutic approach to deter toxicological insults and pathologies associated with exposure to environmental pollutants • It appears that fish-derived omega-3 fatty acids are extremely protective against pollutant-induced inflammation, and membrane domains such as caveolae or other types of lipid rafts may provide a regulatory platform for cellular protection by omega-3 fatty acids Hennig, et al, Nutrition Can Modulate The Toxicity of Environmental Pollutants EHP, 2012, Vol 120(6): 771-774 ©2015 The Institute for Functional Medicine Enhance Antioxidant Reserves Imbalanced Detoxification is a Major Source of Free Radicals Phase II Phase I Conjugation CYP P450 Reactive Intermediate Non-Polar Xenobiotic Inert Water-Soluble Metabolite Damage to DNA, RNA, Proteins ©2015 The Institute for Functional Medicine Nutrition and Cellular Protection • Study data suggest that antioxidant nutrients, such as vitamin E and dietary flavonoids, as well as a high ratio of omega-3 to omega-6 fatty acids, can protect against endothelial cell damage mediated by persistent organic pollutants. • Diets rich in antioxidants and anti-inflammatory nutrients can improve health and decrease vulnerability to additional chemical stressors. Hennig, et al, Nutrition Can Modulate The Toxicity of Environmental Pollutants EHP, 2012, Vol 120(6): 771-774 ©2015 The Institute for Functional Medicine Antioxidants for Detox: Useful Sources • Rosemary • Curcumin (turmeric) • Flavonoids – – – – – Anthocyanidins (berries, grapes, beets) Ellagic acid (pomegranate, strawberries) Quercitin (fruit and vegetable skin) Green tea catechins (polyphenols) Trans-resveratrol (Cabernet; Merlot) ©2015 The Institute for Functional Medicine Antioxidants for Detox: Useful Sources • • • • Carotenoids (Lycopene) Tocopherols (esp. gamma & alpha) NAC/ Glutathione Alpha lipoic acid • Coenzyme Q10 ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine Glutathione • The primary intracellular non-enzymatic antioxidant: present in all living cells • High concentrations in brain parenchyma & liver • Neutralises exogenous & endogenous peroxides • Phase II conjugating agent for heavy metals, external toxicants, carcinogens, pharmaceuticals ©2015 The Institute for Functional Medicine Dietary Supplements to Optimize Reduced Glutathione Levels • • • • • • Vitamin C: 500-3000 mg N-acetyl cysteine, 600-3000 mg/day Lipoic acid, 200-1800 mg/day Curcumin: 500-3000 mg/day Milk thistle: 1000-2000 mg/ day Whey protein concentrates, 2-3 servings/day (2040 grams) ©2015 The Institute for Functional Medicine Detoxification Basics Liver detoxification pathways and supportive nutrients © 2007 The Institute for Functional Medicine Selected Phytonutrients with roles in Detoxification Phytonutrient Sources Detox Effects Dosage Curcumin (diferulomethane) Turmeric • Upregulation of Phase II • Cholagogue & Cholerectic • Antioxidant & Antiinflammatory 500-3000 mg/day and dietary sources Glucosinolates: • Induces Phase II detox enzymes • Induces Antioxidant enzymes >100 mg/day • Sulforaphane • Phenylethylisothiocyanate • Di-indolemethane Cruciferous Vegetables • Cabbage • Broccoli • Brussels sprouts • Watercress Ellagic Acid Walnuts, pomegranate, raspberries, strawberries • • • • 250 mg/day Catechins Green Tea Cocoa • Bi-functional Modulator of Phase I and II enzymes • Antioxidant • Binds toxins >500 mg/day Organosulfates • Γ-glutamylcysteines • Cysteine sulfoxides Alliums • Garlic • Onion • Increases Glutathione • Induce phase II 1000mg/day (as Garlic) Silymarin Milk Thistle • Hepatoprotectant • Antioxidant • Increases glutathione 400-1200mg/day Hepatoprotectant Binds some toxins Inhibits CYP1A1 of carcinogens Induces Phase II ©2015 The Institute for Functional Medicine Learning Objectives • Define what a toxicant is, outline our increasing exposure to toxins, and evaluate the health consequences of a chronic, low level toxic load • Understand the process of biotransformation or detoxification and how it may be modified • Develop competency in assessing for chronic toxicity • Develop strategies to minimise toxic exposure, increase mobilisation, biotransformation, and excretion of toxins. • Be able to implement a foundational detoxification programme. ©2015 The Institute for Functional Medicine First, start with food ©2015 The Institute for Functional Medicine Dietary Protocols should be: • Flexible and adaptable • Relatively easy and straightforward to use • Designed to allow for consistent evaluation ©2015 The Institute for Functional Medicine Core Food Plan Modifications Elimination Diet Comprehensive Elimination Diet Core Food Plan Low Glycaemic Impact Cardiometabolic Food Plan Detox Foods Detoxification Food Plan ©2015 The Institute for Functional Medicine ©2015 The Institute for Functional Medicine Comprehensive Guide ©2015 The Institute for Functional Medicine Complementing Dietary Protocols with Oligoantigenic Food Products • Generally easily digested • Enhanced compliance from use of single formula • Versatility of administration (powder versus pills) • Nutrient dense formulations can supply antioxidants and other nutrients specific for application ©2015 The Institute for Functional Medicine Foundation Detox Protocol • Hypoallergenic dietary programme: – Detox diet programme – Increased dietary fibre content (or supplement) – Clean source of low allergy protein • Nutritional support for Phase 1/Phase 2 • Antioxidant and Phase 2 induction support • Sauna, hot/cold hydrotherapy ©2015 The Institute for Functional Medicine Foundation 4-6 Week Programme: Moderate Intensity • Programme A: • Begin detox diet • After 1 week, work in one day in which diet consists of steamed vegetables, rice and 3 servings of detox functional food • Maintain programme for 4-6 weeks • Programme B: • • • • • Begin detox diet Begin to ramp up with clean supplemental detox functional food Work up to 2-3 servings with detox diet Maintain programme for 4-6 weeks Gradually ramp down while maintaining detox diet ©2015 The Institute for Functional Medicine Foundation 21 Day Programme: Aggressive • Day 1: • • Begin detox diet Begin ramp up of supplemental nutritional support • Day 7-11: – Gradually eliminate dietary protein sources, grains, fruits and vegetables – Begin to ramp up with clean detox functional food • Day 11-13: – ‘fasting’ for 3 days on detox functional food and nutritional support only • Day 14-21: – Gradually ramp down on detox functional food while ramping back up on full diet protocol ©2015 The Institute for Functional Medicine Alternative Foundation 17 Day Programme Aggressive • Day 1-7: • Begin detox diet • Day 8-11: – Gradually eliminate dietary protein sources, grains, fruits and vegetables – Begin to ramp up with detox functional food • Day 12-14: – Cruciferous vegetables and detox functional food for 3 days • Day 15-17: – Gradually ramp down on detox functional food while ramping back up on full detox diet protocol ©2015 The Institute for Functional Medicine What are the main variables to clinical response? • Genetic limitations on detoxification (Phenotypic status) • Genetic predisposition to toxicant-related illness such as autoimmunity and cancer • General health, current/past illnesses, medications • Quantity, intensity, duration, and diversity of exposure • Diet and antioxidant status • Age and Gender • Gastrointestinal flora and bowel frequency ©2015 The Institute for Functional Medicine Functional Medicine & Toxicology: Fundamental Principles 1. Exposure to environmental toxins is widespread, increasing and lifelong. 2. The total body burden of these toxins can act synergistically to cause physiologic dysfunction. 3. This dysfunction can lead to chronic illnesses in susceptible individuals. 4. Susceptibility is largely defined by an individual’s ability to biotransform, detoxify and eliminate exogenous and endogenous toxins. 5. Lifestyle, diet and nutraceuticals can enhance detoxification, prevent disease and restore health. ©2015 The Institute for Functional Medicine Precautionary Principle: “We (as physicians) must act on facts…and on the most accurate interpretation of them, using the best scientific information. That does not mean that we must sit back until we have 100% evidence about everything. When the state of the health of the people is at stake…we should be prepared to take action to diminish those risks even when the scientific knowledge is not conclusive.” Horton. Lancet. 1998;352(9124):251 ©2015 The Institute for Functional Medicine “In every case of every malady there are two sets of factors at work in the formation of the morbid picture, namely, internal or constitutional factors inherent in the sufferer and usually inherited from his forebears, and external ones which fire the train.” Archibald Garrod Inborn Factors in Disease (1908) ©2015 The Institute for Functional Medicine