Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
220
Influence of Ribose, Adenosine, and "AICAR" on the
Rate of Myocardial Adenosine Triphosphate Synthesis
during Reperfusion after Coronary Artery Occlusion
in the Dog
M. Mauser, H.M. Hoffmeister, C. Nienaber, and W. Schaper
From the Max-Planck-Institute, Department of Experimental Cardiology, Bad Nauheim, Federal Republic of Germany
Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017
SUMMARY. Recovery of adenosine triphosphate after myocardial ischemia is limited by the slow
adenine nucleotide de novo synthesis and the availability of precursors of the nucleotide salvage
pathways. We determined the adenine nucleotide de novo synthesis in the dog by infusion of
[uC]glycine and the acceleration of adenine nucleotide built up by intracoronary infusion of ribose
together with [14C]glycine or radiolabeled 5-amino-4-imidazolcarboxamide riboside or adenosine
in the same animal model and with the same dosage of substrates (9 mmol) in postischemic and
nonischemic myocardial tissue. After 45 minutes of occlusion of a side branch of the left coronary
artery, the ischemic area was reperfused for 3 hours, and needle biopsies were taken for
biochemical analysis. Adenine nucleotide de novo synthesis was found to be very slow (1.5 nmol/
g wet weight per hour). The rate was doubled after ischemia. Adenine nucleotide synthesis was
accelerated 5-fold by ribose, the basic substrate of the adenine nucleotide de novo synthesis, 9fold by 5-amino-4-imidazolcarboxamide riboside, an intermediate of the adenine nucleotide de
novo synthesis and 90-fold by adenosine, a substrate of the nucleotide salvage pathway.
Therefore, only adenosine infusion resulted in a measurable increase of adenosine triphosphate
levels after 3 hours of reperfusion, but over a longer time period, ribose or 5-amino-4-imidazolcarboxamide riboside also can be expected to replenish reduced myocardial adenosine triphosphate
faster than adenine nucleotide de novo synthesis. Studies with radiolabeled 5-amino-4-imidazolcarboxamide riboside showed significant incorporation of radioactivity into 5-amino-4-imidazolcarboxamide ribose triphosphate which had also risen measurably during 5-amino-4-imidazolcarboxamide ribose infusion, and which is not normally found in heart muscle. (Circ Res 56:
220-230, 1985)
IT is a well-established fact that ischemia leads to a
depletion of adenosine triphosphate (ATP) (Chang,
1938; Burdette, 1956; Berne, 1963; Gerlach et al.,
1963) which is not readily reversible upon reoxygenation of tissue, especially when the coronary occlusion (or other forms of oxygen deprivation) lasted
longer than 10 minutes (Danforth et al., 1960; Kammermeier et al., 1963, 1964; Isselhard et al., 1964,
1970a; Schaper et al., 1979). The slow rate of ATP
synthesis after ischemia (Zimmer et al., 1973) is
mainly the result of two factors. (1) The conversion
of glucose-6-phosphate to ribose-5-phosphate proceeds extremely slowly in mammalian heart muscle
(Zimmer and Gerlach, 1978; Ibel et al., 1982). (2)
Substrates for the salvage pathways, notably adenosine, but possibly also inosine and hypoxanthine,
are rapidly washed out of the tissue upon reflow
and are hence lost for salvage (Katori and Berne,
1966; Fox et al., 1979).
Clinical efforts to reestablish blood flow in acute
myocardial infarction by fibrinolysis (Schmutzler et
al., 1966; Rentrop et al., 1981) were reported to be
successful, but mechanical function of the reperfused segment often returns only after a long delay.
This effect is known from animal experiments
(Kloner et al., 1981). Other probable metabolic effects of ischemia and reperfusion that cannot be
measured in human patients may also be dependent
on ATP. A fast restitution of ATP levels during
reflow after ischemia appears highly desirable. We
report here in a comparative study the three most
promising substances, i.e., ribose, 5-amino-4-imidazolcarboxamide riboside (AICAR), and adenosine,
for repletion of purine nucleotides.
Methods
Experimental Design
Thirty-eight dogs of either sex weighing approximately
28 kg were anesthetized with subcutaneous piritramide (5
kg) and intravenous sodium pentobarbital (15 mg/kg).
They were artificially respired with a Bird respirator system using a gas mixture containing 30% nitrous oxide,
70% oxygen. The oxygen concentration was adjusted to
Mauser et al. /Acceleration of ATP Synthesis
Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017
give an arterial P02 between 100 and 120 mm Hg. The
PCO2 varied between 38 and 45 mm Hg. A Millar catheter
tip manometer was advanced into the left ventricle via the
left carotid artery, aortic blood pressure was monitored
with a catheter (via the right femoral artery) that was
connected to a Statham P23 pressure transducer. A venous
line was established via the left femoral vein. Under
fluoroscopic control, a Flexo pulmocath catheter (F4) was
advanced into the descending branch of the left coronary
artery (LAD) via a transfemoral guiding catheter for intracoronary infusion. The dogs were anticoagulated at the
beginning with 5000 IU heparin, intravenously, followed
by the same dose after 2 hours. Left thoracotomy and
exposure of the heart was performed via the 5th intercostal
space and a side branch of the LAD was prepared at its
origin. A snare was placed around the artery for occlusion
and reperfusion. The whole preparation was allowed to
stabilize for 30 minutes. After 45 minutes of occlusion of
the LAD sidebranch, the ischemic area was reperfused for
3 hours. Reperfusion was documented by fluoroscopic
control. Nine millimoles (1 ml/min of a 50 mM solution)
of ribose (seven dogs), AICAR (seven dogs), or adenosine
(eight dogs) were infused via the intracoronary catheter
into the LAD proximal to the previously occluded vessel.
One group with saline infusion (seven dogs) served as a
control.
Radiolabeled nucleosides (5-amino-2-3H diazole-4-carboxamidriboside, [3H]AICAR, or 2-[3H]adenosine) were
added to 'cold' nucleosides to obtain a specific activity of
4.5 mCi in 9 mmol total amount infused (n •= 3 dogs for
each nucleoside).
Ribose incorporation was measured by infusion of 9
mmol ribose for 3 hours, together with l-[14C]glycine
(specific activity 55.4 mCi/mmol) with an infusion rate of
0.8 mCi/hr (n = 3).
Purine de novo synthesis was measured by intracoronary infusion of l-[14C]glycine (specific activity 55.4 mCi/
mmol) for 3 hours with an infusion rate of 0.8 mCi/hr (n
= 3 dogs).
Needle biopsies (Tru-Cut) for biochemical analysis of
nucleotides, nucleosides, and creatine phosphate were
taken before any intervention, at the end of 45 minutes
of regional ischemia, and after 3 hours of reperfusion. In
dogs that received ribose, AICAR, or adenosine infusion,
biopsies after 3 hours of reperfusion were obtained from
the previous ischemic area, from nonischemic areas distal
to the intracoronary substrate infusion, and from nonischemic areas that received the substrate via recirculation
(posterior of the heart). The experiment was terminated
after the last biopsy with 10 ml of concentrated potassium
chloride, the heart was removed, sliced in bread-loaf
fashion, and myocardial rings were incubated in p-nitroblue terrazoliumchloride to exclude hearts with marked
subendocardial infarctions. Since we occluded only a sidebranch of the LAD, no infarction occurred within 45
minutes of ischemia which would have occurred if the
whole LAD had been occluded for the same time period.
ECG, left ventricular pressure, LV dP/dt, and aortic
pressure were recorded on a direct-writing inkjet recorder.
Instantaneous myocardial oxygen consumption was calculated on-line according to Bretschneider's equation
(Bretschneider et al., 1970) by a digital computer, and kept
in a range between 6 and 7 ml O2/IOO g per min. In dogs
receiving AICAR, blood samples from the left atrium and
the inferior vena cava were obtained before ischemia and
in short intervals during AICAR infusion.
221
Tissue Sampling and Biochemical Analysis
Extraction Procedures
Biopsies (10-25 mg) were frozen immediately (2-3 seconds) in liquid nitrogen and weighed on a Kettler balance
in precooled vials. The frozen tissue was homogenized in
ice cold 0.6 M perchloric acid (400 ^1) with an ultrasound
homogenizer (Sonicator Cell Disruptor W-225 R) for 10
seconds. The homogenate was centrifuged at 12,000 rpm
for 3 minutes, and 350 ti\ of the supernatant were neutralized with the required volume of 6 N KOH, resulting
in a total volume of about 420 /d. The supernatant was
decanted and stored in liquid nitrogen until it was analyzed, within the next 3 days. Blood samples were immediately centrifuged at 3000 rpm for 5 minutes, and 200 /xl
of serum were added to 500 /il of 0.6 N perchloric acid.
The supernatant extract was neutralized with 6 N KOH
and stored at -36°C.
Nucleotide and Nucleoside Analyses
ATP and creatine phosphate values were determined
using bioluminiscence, as described by Ellis and Gardner
(1980). Normal ATP values in the dog are reported to be
4 Mmol/g wet weight with this method. ADP, AMP, IMP,
NAD, and AJCAR-monophosphate were separated and
quantified by high performance liquid chromatography
(HPLC), using a Varian 5000 gradient controller combined
with a Dupont spectrophotometer and a Dupont integrator. A 50-fA sample of the undiluted supernatant extract
was injected onto a Zorbax-NH2 column (Dupont) and
developed isocratically with 5 mM NH,H2PO4 (pH 2.8) for
15 minutes, followed by a linear gradient of 5 mM to 750
mM NH^HzPO* (pH 4.5) at a flow rate of 2 ml/min.
Nucleosides and AICAR were separated on a Dupont
ODS column using a linear gradient of 0 to 30% methanolwater (vol/vol) within 25 minutes. Uric acid and AICAR
in plasma were separated on a Dupont ODS column using
a linear gradient of 30 mM KH2PO4 (pH 3.5) to 30%
methanol diluted in 30 mM KH2PO4 (pH 3.5) within 25
minutes.
The peaks found at 254 nm were identified by comparison of retention times with external standards. Peak areas
were quantified by using peaks of known concentration
and expressed in nmol/g or jimol/g wet weight. Since
Reimer (Reimer et al., 1981) showed that tissue water after
regional ischemia changes in the first hours of reperfusion
by only 3%, no dry weight determinations were made.
For separation of amino acids in myocardial tissue, 20
fil of a solution containing 800 mg o-phtalaldehyde and
200 n\ mercaptoethanol in 10 ml methanol were added to
150 ^1 of the sample for pre-column derivatization. A
linear gradient of 30 minutes was established between
solution A (tetrahydrofuran, methanol, 0.05 M sodium
acetate, pH 5.9, 0.8/19.2/80, vol/vol/vol) and solution B
(methanol, 0.05 M sodium acetate, pH 5.9, 80/20, vol/vol)
on a Waters Radial Compression System using a C-18
column. Amino acids were detected with a fluorescence
spectrophotometer (Kratos) at an emission wavelength of
228 nm and a 470 nm cut-off filter.
Analysis of [3H]AICAR, [3H]Adenosine, and
Incorporation
["QGlycine
Four biopsies were extracted together in one vial, as
described above, to obtain larger amounts of nucleotides.
Fifty microliters of the supernatant extract were injected
Circulation Research/Vo/. 56, No. 2, February 1985
222
Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017
onto a DuPont ODS column and developed by means of
a paired ion gradient system. A linear gradient was established, using 5 mM tetrabutylammonium phosphate with
30 mM KH2PO4 (pH 5.5) and 2% to 40% acetonitrile within
40 minutes. This resulted in a good separation of guanosine triphosphate (GTP), AICAR-triphosphate, and ATP.
There was no coelution of ADP and adenylsuccinate
which occurs with the ion-exchange method used for
quantification of the nucleotides. AICAR triphosphate was
identified as described by Sabina et al. (1982). We sampled
AMP, ADP, IMP, ATP, and, if present, AICAR triphosphate by collecting the outflow of the HPLC column for
the entire peak into scintillation vials containing 10 ml
xylene scintillation fluid (Packard Instruments). Radioactivity was counted on a Packard Tri-Carb liquid scintillation counter and expressed in counts/min per 100 mg wet
weight. To verify that radioactivity is not found in any
other compound of the chromatogram, the column outflow of one biopsy of each experiment was sampled
continuously in 30s fractions. No loss or interchange of
the tritium atoms from [3H]AICAR or [3HJadenosine was
detected, since the radioactivity baseline was always low
and stable, and radioactivity was found only in anabolic
or catabolic products of AICAR or adenosine.
For quantification of [3H]AICAR and [3H]adenosine incorporation into the nucleotides, the specific activity of
the substrates in the infusate was determined by quantification of the substrate concentration by HPLC. The
column outflow during the substrate peak was sampled,
and radioactivity was counted in a liquid scintillation
counter, as described above. Since there is no measurable
AICAR content and only a minimal adenosine content in
reperfused myocardial tissue, the specific activity of the
infused substrates equals that of the tissue, and radioactivity incorporated into nucleotides can directly be converted into concentration.
In the experiments with [14C]glycine as a marker of the
nucleotide synthesis, specific activity of myocardial tissue
glyrine was measured directly, by the HPLC separation
method, as described above. A total of 43.3 jimol of glycine
was infused intracoronary within the 3-hour period. This
increases plasma glycine levels by only 2.5%, assuming a
50 ml/min flow in the LAD. Because of the dilution of the
intracoronary infusate in the whole body fluid, the recdrcularing radioactive glycine can be neglected, as compared
to the activity in the intracoronary blood, i.e., the specific
activity of glycine in the peripheral venous plasma was
under 3%, compared to the calculated specific activity in
the intracoronary plasma. Furthermore, the specific activity of myocardial tissue glycine in myocardial areas that
received [I4C]glycine only via retirculation was only 7%
compared to areas of intracoronary [MC]glycine infusion.
Therefore, because of the rapid exchange of glycine
between blood and cells (Elwyn et al., 1972), a constant
tissue-specific activity can be expected within minutes of
the 3-hour infusion period and can be maintained over
the infusion period.
Chemicals
AICAR, adenosine, ribose, NR,H2PO4, KH2PO4, tetrabutylammonium phosphate, and all nucleotides and nucleosides for HPLC-standards were obtained from Sigma
Chemicals. [3H]Adenosine and [uC]glycine were made by
Amersham Inc. [3H]AICAR was made to our specification
by Amersham, Inc. Fireflyluciferase was obtained by Lumac and creatine kinase by Boehringer Mannheim.
Statistics
Statistics were done by paired or unpaired /-test. All
values are expressed as means ± SE, unless otherwise
mentioned.
TABLE 1
Hemodynamics
HR
Saline
Ribose
AICAR
Adenosine
110.5 ±8.0
91.8 ±6.2
86.4 ± 6.5
99.5 ± 8.7
94.3 ± 5.7
80.5 ± 9 . 1
86.4 ± 6.1
95.6 ± 7 . 1
102.0 ± 6.2
83.6 ± 8 1
106.0 ± 7.1
113.0 ± 6.9*
Control
129.0 ± 5 . 2
126.0 ± 7.2
119.0 ± 3 . 2
137.0 ± 9 . 4
Ischemia
(45 min)
Reflow
(180 min)
120.0 ± 6.0
125.0 ± 4.4
120.0 ± 2.9
129.0 ± 7.7
117.0 ± 5 . 1
124.0 ± 8.2
106.0 ± 7.1
118.0 ±9.2*
Control
(beats/min)
Ischemia
(45 min)
Reflow
(180 min)
LVPsys
(mm/Hg)
MVO2
(ml/100 g per
min)
Control
8.74 ± 0.41
6.51 ± 0.56
6.28 ± 0 33
7.71 ±0.51
Ischemia
(45 min)
Reflow
(180 min)
7.29 ± 0.43
6.08 ± 0.51
6.84 ± 0.48
7.41 ± 0.54
6.98 ± 0.31
6.50 ± 0.62
7.41 ± 0.37
8.24 ± 0.57*
Results (in all tables) are expressed as means ± SE.
* P < 0.05 (compared to control) (paired f-test).
Mauser et a/./Acceleration of ATP Synthesis
223
TABLE 2
Results
Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017
Hemodynamics
Global hemodynamic parameters, such as heart
rate, left ventricular pressure, and aortic pressure,
remained unchanged over the entire experiment in
the control-, ribose-, and AICAR-treated group (Table 1). In the adenosine-treated group, heart rate
was significantly higher and aortic mean pressure
lower during adenosine infusion, which is due to
the peripheral vasodilating effect of adenosine. The
hemodynamic changes were larger during the first
hour of reperfusion and changed toward normalization during the following 2 hours of adenosine
infusion, resulting in an 11% reduction of aortic
mean pressure and a 10% increase of heart rate after
3 hours of adenosine infusion (Table 2). Subsequently, the instantaneous myocardial oxygen consumption (MVO2) was found to be stable in a range
between 6 and 7 ml 02/min per 100 g in the control-, ribose-, and AICAR-treated group, but increased during adenosine infusion.
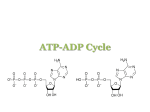
Effects of Ischemia on High-Energy Phosphates
In our experimental model, 45 minutes of regional
ischemia led to a marked depression of tissue ATP
by 50% (Fig. 1) and creatine phosphate by 80-90%
(Table 3). AMP concentrations were doubled and
ADP concentration remained unaltered. The breakdown products of AMP, like adenosine, inosine, and
Heart Rate (HR) and Mean Aortic Pressure (AOPJ after 45
Minutes of Ischemia and during 3 Hours of Reperfusion with
Intracoronary Adenosine Infusion (3 mM/hr)
Control
Ischemia (45 min)
Reflow (60 min)
Reflow (120 min)
Reflow (180 min)
HR
AOPm
99.5 ± 8.7
95.6 ± 7.1
132.1 ± 7.2*
123.2 ± 6.8t
113.4 ± 6.9f
113.0 ± 7 . 3
109.5 ±5.7
83.4 ± 8.8*
92.6 ± 7.6|
99.0 ± 9.3t
•P<0.02.
fP<0.05.
hypoxanthine/xanthine, were markedly increased.
NAD was decreased by 24.6% (Table 3).
Effect of Reperfusion on High Energy
Phosphates
ATP de Novo Synthesis
Adenine nudeotide de novo synthesis was measured by l-[14C]glycine incorporation into nudeotides. Specific activity of [14C]glydne in myocardial
tissue after 3 hours of [14C]glydne infusion is shown
in Table 4. From the known specific activity and the
detected radioactivity in the ATP and ADP, the
nudeoside synthesis rates were calculated (Table 5).
Basic ATP synthesis rate in nonischemic tissue was
found to be very slow (3.74 nmol/g wet weight per
TABLE 3
Nudeotides, Nudeosides, and Creatine Phosphate Levels after 45 Minutes of Iachemia and 3
Hours of Reperfusion with Different Substrate Infusion
Reperfusion
Control
45 Min
of
Ischemia
Saline
AICAR
ADP
(nm/g wet wt)
AMP
(nm/g wet wt)
IMP
(nm/g wet wt)
Adenosine
(nm/g wet wt)
Inosine
(nm/g wet wt)
Hypoxanthine
(nm/g wet wt)
AICAR
(nm/g wet wt)
AICAR-MP
(nm/g wet wt)
NAD
(nm/g wet wt)
1120 ± 6 1
980 ± 8 2
822 ± 81*
912 ± 57*
68.1 ±3.0
144.0 ±9.0*
41.0 ± 3.1*
42.3 ± 2.8*
54.8 ± 17.1
7.1 ±4.3
7.4 ±5.1
ND
67.0 ± 10.0*
8.8 ± 4.3
9.0 ±0.9
65.7±15.4f
8.1 ± 0.9
7.3 ± 1.7
174.1 ± 36.8f
9.2 ±3.5
1131±249f
5.2 ± 1.6
5.9 ±1.7
212±42.0f
ND
261 ± 24.1
ND
ND
55.1 ±9.9
ND
ND
ND
985 ± 266
ND
ND
ND
ND
572 ± 91
ND
691 ± 83
522 ± 71*
543 ± 43*
580 ± 25*
498 ± 72*
CP
(MM/g wet wt)
9.25 ± 0.73
2.75 ± 0.25f
8
8
Adenosine
748 ± 102*
12.26 ± 0.49* 12.94 ± 0.53* 10.52 ± 0.38
* P < 0.01; f P < 0.001 compared to control (paired (-test).
8
224
Circulation Research/Vol. 56, No. 2, February 1985
TABLE 4
TABLE 6
Glydne Levels and Glydne Specific Activity after 3 Hours of
"C-Glydne Intracoronary Infusion in Postischemic and
Nonischemlc Myocardial Tissue
Purine Nudeotide de Novo Synthesis and Accelerated
Synthesis Rates after 3 Hours of Intracoronary Substrate
Infusion in Previously Ischemic and Nonischemic
Myocardium*
Glycine level
(runol/g wet wt)
Specific activity
(counts/min per nmol)
Postischemic
Nonischemic
815.2 ±62.3
1041.5 ±83.5
de Novo
Ribose
AICAR
Adenosine
Postischemic
3.07
±0.26
15.06
±0.39
27.4
±3.3
268.5
±45.2
Nonischemic
1.50
±0.31
9.77
±0.49
28.5
±4.2
218.7
±36.0
3830.2 ± 262.5 3974.3 ± 296.3
Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017
3 hr). Within the first 3 hours of reperfusion of
previously ischemic tissue, the rate was doubled
(7.48 nmol/g wet weight per 3 hr) (Table 5). The
synthesis rates of adenine nucleotides were 3.07
nmol/g wet weight per hr in postischemic and 1.50
nmol/g wet weight per hr in nonischemic myocardium (Table 6). This slow synthesis rate would lead
only to nonmeasurable increases of ATP within 3
hours of reperfusion. Therefore, the ATP levels in
the control group with 45 minutes of ischemia and
3 hours of reperfusion remained depressed to 50%
of normal (Fig. 1). AMP, adenosine, and inosine,
and hypoxanthine levels returned to normal values.
Creatine phosphate concentrations showed a
marked increase compared to ischemic levels to a
value of 15% above normal ('overshoot') (Table 3).
Ribose as a Substrate for ATP Synthesis
The synthesis rate of adenine nucleotides (AN)
with ribose-infusion was determined in the same
way as the AN de novo synthesis, by infusing ribose
together with [14C]glycine. The synthesis rate was
found to be 15.1 nmol/g wet weight per hr in
postischemic and 9.8 nmol/g wet weight per hr in
nonischemic tissue (Table 6). This results in a 5- to
6-fold increase of AN de novo synthesis. This increase is far too low to be measured in overall tissue
ATP levels, and therefore no increase of ATP could
be shown within 3 hours of reperfusion (Fig. 1).
Creatine phosphate concentration showed the same
"overshoot' phenomenon as in the saline-treated
control group (control, 9.7 ± 0.6 ^mol/g wet weight;
* In nmol/g wet weight per hour.
180 minutes of reperfusion, 12.2 ± 1 . 7 ftmol/g wet
weight).
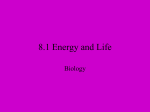
AICAR as a Substrate of ATP Synthesis
AICAR was taken up by the myocardial cell and
was phosphorylated to AICAR-monophosphate (AICAR-MP) (Fig. 2). At the same tissue AICAR concentration, the phosphorylation rate was higher in
previously ischemic compared to nonischemic myocardium. Since AICAR concentrations were twice as
high (previous ischemic areas) or 4-fold as high
(nonischemic areas) as AICAR-MP concentration,
phosphorylation seemed to be rate limiting. Areas
that received AICAR only via blood recirculation in
a 70-fold lower plasma concentration showed a 15fold lower AICAR tissue concentration and a lower
AICAR-MP concentration compared to infusion
areas. This demonstrates a dose-dependent AICAR
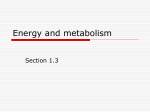
uptake and AICAR-MP formation (Fig. 2). Transformation of AICAR-MP to inosine monophosphate
(IMP) is shown by the 9-fold increase of IMP in the
tissue (Table 3) and the incorporation of 3H into
IMP in [3H]AICAR-treated dogs (Fig. 3a; Table 7).
This incorporation is dependent on the AICAR-MP
levels. Only 15% of the AICAR-MP activity was
found in IMP. A similar percentage was found in
the increase of tissue levels of AICAR-MP and IMP.
Further incorporation into the adenine nudeotide
pool is shown by 3H incorporation into ADP and
ATP (Table 7; Fig. 3, a and b). There are also linear
TABLE 5
Incorporation of Radioactivity into ATP and ADP within 3 Hours of "C-Glycine Intracoronary
Infusion with or without Addition of Ribose (3 mM/hr) and Calculated Synthesis Rates
[14C]Glycine
[uC]Glycine + ribose
Radioactivity
(counts/min
per g wet wt
X103)
Synthesis rate
(nM/g wet wt
per3hr)
Radioactivity
(counts/min
per g wet wt
x 103)
Synthesis rate
(nM/g wet wt
per3hr)
ATP
I
NI
28.6 ± 4.4
14.9 ±4.3
7.48 ±1.15
3.74 ± 1.08
122.9 ± 5.7
85.5 ± 6.7
32.09 ± 1.49
21.50 ±1.68
ADP
I
NI
6.7 ±1.3
3.0 ±1.3
1.74 ±0.33
0.76 ± 0.32
47.3 ± 8.6
31.1 ± 7.5
12.34 ± 2.31
7.82 ±1.89
I •=» previously ischemic myocardium; NI = nonischemic myocardium.
Mauser et al. /Acceleration of ATP Synthesis
n=7
225
n=7
5--
JL
_L
o
o
1
1
2+
Adenosine as a Substrate of ATP Synthesis
I
1-
C I R
Saline
C I R
Ribose
C I R
AICAR
0.15 and 0.3 fimol/g wet weight in the areas with
intracoronary AICAR infusion. Inosine and hypoxanthine tissue levels stayed within normal limits
during AICAR infusion (Table 3). Creatine phosphate showed the same postischemic overshoot as
the control group.
C I R
Adenosine
Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017
FIGURE 1. Tissue ATP levels before ischemia (C), after 45 minutes of
regional ischemia (I), and after 3 hours of reperfusion (R) with
intracoronary infusion of ribose, AICAR, or adenosine. A group with
saline infusion served as a control. Within 3 hours, only adenosine
infusion leads to a significant increase in tissue ATP levels.
correlations between the [3H]AICAR-MP levels and
radiolabel incorporation into ADP and ATP (Fig. 3,
a and b). The net ATP synthesis can be calculated
from the 3H incorporation into ATP and from the
known specific activity of infused AICAR. It results
in a rate of ATP synthesis of 19 nmol/g wet weight
per hr in areas of intracoronary AICAR infusion
(Table 7). This increase is too small to be detected
in overall tissue ATP-levels after 3 hours of reperfusion. Consequently, there was no difference between the endischemic ATP values and those, after
3 hours of reperfusion with AICAR (Fig. 1). A
marked percentage of the AICAR-MP activity was
found in AICAR triphosphate (AICAR-TP) which is
synthesized in preference to ATP with high AICAR
concentrations (Fig. 3b). Tissue AICAR-TP concentrations calculated from these data ranged between
After [3H]adenosine infusion, radioactivity was
found in AMP, ADP, and in large amounts in ATP,
resulting in an adenine nucleotide synthesis rate of
268 nmol/g wet weight per hr (Table 7). A similar
synthesis rate (323 nmol/g wet weight per hr) was
calculated from the directly measured increase in
tissue ATP concentrations (Fig. 1). Tissue adenosine
levels were higher during adenosine infusion compared to values at the end of ischemia, demonstrating that the infused adenosine is only partially
deaminated until it reaches the reperfused postischemic myocardium (Table 3).
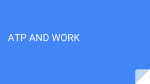
Catabolism of AICAR and Adenosine
With AICAR infusion, no rise in tissue inosine or
hypoxanthine concentrations was found (Table 3).
Plasma uric acid concentrations increased with time
with no difference between left atrial and vena cava
inferior blood (Fig. 4a). A marked difference in
AICAR levels between caval and left atrial blood
but no difference in uric acid levels indicates peripheral uptake of AICAR and renal elimination of nonmetabolized AICAR (Fig. 4b).
Adenosine infusion is followed by high tissue
inosine and hypoxanthine (Table 3) and high hypoxanthine levels in plasma (control, 0.18 ± 0.01
mg/liter; 3 hours of adenosine infusion, 1.21 ± 0.49
mg/liter), showing fast deamination of adenosine in
blood and tissue. No adenosine was found in vena
cava inferior blood. Uric acid levels were twice as
high as after AICAR infusion (11.32 ± 0.25 mg/
liter).
AICAR-MP
CNM/G WUD
1200
NO ISCHEMIA
o AICAR INFUSION
A AICAR RECIRCULATION
1000
ISCHEMIA
•AICAR INFUSION
800
o
600
o
o
400
200
500
1000
1500 2000 2500 3000 3500 4000
AICAR • CNM/G UU]
FIGURE 2. AICAR phosphorylation is shown by plotting
the content of AICAR vs. AICAR monophosphate of
single biopsies obtained from different sites of the heart.
Comparison of ischemic (closed circles) and nonischemic (open circles) intracoronary infusion areas demonstrates a higher phosphorylation rate in previously
ischemic areas, and comparison of infusion areas to
areas that received AICAR via recirculation shows a
dose-dependent build-up of AlCAR-monophosphate.
Circulation Research/Vol. 56, No. 2, February 1985
226
TABLE 7
Incorporation of [*H]AICAR or Adenwine into Nndeotides* and Calculated Nucleotide
Synthesis Ratest
[3H]Adenosine
['HJAICAR
IMP
AMP
ADP
ATP
AICAR-TP
I
Nl
I
Nl
I
Nl
I
Nl
I
Nl
Radioactivity
(counts/min
per g wet wt
XlO3)
Synthesis rate
(nmol/g wet
wt per 3 hr)
16.4 ± 4.5
16.2 ± 6.2
37.2 ± 9.6
36.8 ±12.1
11.2 ±2.9
11.2 ±5.2
24.8 ± 4.9
25.5 ± 5.4
81.8 ± 11.9
80.1 ± 13.4
25.5 ± 6.2
27.9 ± 8.4
56.7 ±11.5
57.3 ± 10.6
186.0 ± 22.6
178.5 ± 26.4
Radioactivity
(counts/min
per g wet wt
X 103)
Synthesis rate
(nmol/g wet
wt p w 3 hr)
8.5 ±1.7
6.7 ± 1.3
48.6 ± 5.2
39.4 ± 2.8
306.6 ±53.2
252.8 ± 39.7
18.94 ±3.1
14.72 ± 1.9
108.0 ±11.6
86.4 ± 19.6
678.3 ±115.3
554.7 ±91.5
Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017
I = previously ischemic myocardium; Nl = nonischemic myocardium.
• Within 3 hours of reperfusion.
f Specific activity of infused compounds: AICAR, 439.8 counts/min peT nmol; adenosine, 451.9
counts/min per nmol.
Discussion
The slow recovery of the depleted adenine nudeoa'de pool, especially of ATP, following a period
of potentially reversible ischemia is well recognized
(DeBoer et al., 1980; Reimer et al., 1981; Swain et
al., 1982b). Since the fall of ATP during ischemia is
not accompanied by a rise in ADP, we must conclude that ADP is quickly transformed to AMP,
which is found to be doubled after ischemia in our
experiments. The myokinase reaction and dephosphorylation of AMP by 5'-nucleotidase leads to
adenosine which is deaminated to inosine. Both
nucleosides can leave the cell. During reflow, the
nucleotide degradation products are washed out of
the interstitial space (Katori and Berne, 1966; Fox et
al., 1979) and are unavailable for the nucleotide
salvage pathways (Maguire et al., 1972; Parker et
al., 1976). The cell is now dependent on the very
slow and energy-consuming de novo synthesis. Our
experiments and those of Zimmer et al. (1973)
showed a doubling of the AN de novo synthesis
during recovery from oxygen deprivation, but, in
our dog experiments, the de novo synthesis rate was
only 38% (3 nmol/g wet weight per hr) compared
to the rate measured in rats. Therefore, it would
have taken about 14 days to synthesize 1.0 ^mol/g
wet weight of ATP. There are two reasons for this.
First, ribose-5-phosphate, the basic substrate of AN
de novo synthesis was shown to be in short supply
after ischemia (Zimmer et al., 1973). Second, the
energy-consuming assembly of the purine structure
by successive attachment of C-fragments to phosphoribosylpyrophosphate is slow in energy-depleted cells. It was already shown by Zimmer (1980)
that exogenous supply of ribose can speed up ATP
synthesis 3- to 4-fold in the rat heart. In our dog
model, ribose infusion leads to similar results by
accelerating AN de novo synthesis 4- to 6-fold. This
acceleration is far too slow to achieve a measurable
increase of ATP within 3 hours of reperfusion. These
results also show that the acceleration of AN synthesis by AICAR or adenosine cannot be due to a
splitting of the molecule and incorporation of the
ribose moiety of the molecule, because acceleration
rates of AN synthesis are higher with AICAR and
adenosine, as compared to ribose.
Studies with AICAR
A new approach bypassing several steps of the
AN de novo synthesis pathway was the infusion of
AICA-riboside (AICAR) as shown by Sabina et al.
(1982). AICAR is the dephosphorylated form of the
AN de novo synthesis intermediate, AICAR monophosphate (AICAR-MP). It enters the biosynthen'c
pathway distal to the major control points (Wyngarden and Ashton, 1959) and needs only one molecule
of ATP and GTP to form AMP. Swain et al. (1982a)
showed a 25% increase of ATP (from a postischemic
70-95% of normal) within 24 hours of AICAR infusion in the dog. In our study, with a more severe
ischemia and a reduction of ATP to 50% of normal,
we demonstrated incorporation of tritium-labeled
AICAR into ATP representing a 9-fold increase of
AN synthesis within the first 3 hours of reperfusion
compared to the de novo synthesis that was measured by [^CJglycine incorporation and a 20-fold
increase of AN synthesis in nonischemic tissue. This
acceleration is twice that for ribose, but is still too
small to be detected from overall tissue ATP levels
within 3 hours of reperfusion. There are two reasons
for the still insufficient acceleration of ATP synthesis
by AICAR. First, uptake, especially in postischemic
tissue, and phosphorylation of AICAR to AICAR
monophosphate by myocytes, is slow: AICAR con-
Mauser et al. /Acceleration of ATP Synthesis
227
IMP
r=0 98)
ADP
= 095)
5000
Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017
10000
15000
AICAR-MP
[cpm/IOOmgWW]
20000
AICAR-MP CONVERSION TO ATP AND AICAR-TP
12000-•
AICAR-TP
(r = 0 97)
9000- •
FIGURE 3. Panel a: AICAR-monophosphate is converted
to IMP and ADP, as shown by incorporation of
['HjAICAR. Radioactivity found in IMP and ADP in
intracoronary infusion areas (squares) and redrculation
areas (triangles) is linearly correlated to the content of
AICAR monophosphate. Panel b: incorporation of ['H]
AICAR into ATP and AICAR triphosphate (AICAR-TP) is
linearly correlated to the levels of AICAR monophosphate
(AICAR-MP) over a wide range of AICAR-MP concentration. With higher AICAR-MP concentrations, in areas of
intracoronary AICAR infusions (squares), AICAR-TP is
built up in preference to ATP. In areas that received
AICAR via redrculation (triangles) in much lower concentrations, incorporation into ATP and AICAR-TP is not
significantly different.
*
£
o
^8 6000-•
3000-
5000
10000
15000
AICAR-MP
[cpm/lOOmqWW]
centrations are twice as high as AICAR-MP concentrations in previously ischemic tissue, and four times
higher in nonischemic tissue. Second, with higher
AICAR monophosphate concentrations, the preferred metabolic pathway is the transformation of
AICAR-MP to AICAR triphosphate. AICAR triphosphate formation from AICAR has also been
shown by Zimmerman and Deeprose (1978) in
erythrocytes, by Bochner et al. (1982) in cells after
10-tetrahydrofolate deficiency, and in small
amounts by Sabina et al. (1982) in the heart after
intraatrial AICAR infusion. The AICAR triphosphate levels reported by Sabina are in the same
range as the levels we found in myocardial areas
that received AICAR via redrculation. In these areas,
AICAR triphosphate formation and ATP buildup is
equal. With higher AICAR-MP levels in areas that
received AICAR via intracoronary infusion, AICAR
20000
triphosphate formation becomes predominant and
leads to AICAR triphosphate levels of 0.15-0.3
jtmol/g wet weight within 3 hours of reperfusion. A
reported inhibition of the enzyme adenylosuccinate
lyase by AICAR-MP (Sabina et al., 1982), which
catalyses the transformation of IMP to AMP, could
not be observed in our study, since there was a
linear correlation between AICAR concentrations
and ATP built up over a 20-fold range encompassing
myocardial areas that received AICAR only via recirculation and myocardial areas that received AICAR via intracoronary infusion. From our data, we
cannot decide whether the metabolism of AICAR to
ATP is linear during the 3-hour infusion period.
However, the constant increase of uric acid in
plasma shows a linear catabolism of infused AICAR.
The slow time-dependent increase of uric acid in
plasma with no differences between left atrial and
228
Circulation Research/Vol. 56, No. 2, February 1985
CMG/L.:
•VENA CAVA INF.
•LEFT ATRIUM
6
5
A
n«4
0
|
30
60
120
AICAR ic INFUSION-
180
I
30
TIME
60
CMIN3
Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017
VENA CAVA I N F .
LEFT ATRIUM
30
60
120
AICAR ic INFUSION -
180
—I
30
TIME
venous concentrations over the whole infusion period is indicative of a slow catabolism of AICAR.
The very high plasma levels of AICAR are also a
parameter for the slow metabolism, and the great
difference between left atrial plasma levels and vena
cava inferior plasma levels under steady state conditions after 1 hour of AICAR infusion can be explained by uptake in peripheral tissue and renal
excretion of nonmetabolized AICAR. The time-dependent increase of plasma uric acid concentration
after AICAR infusion would suggest IMP formation.
Since IMP is a crossroad of three metabolic pathways (IMP to AMP, IMP to GTP, IMP to inosine),
we are not surprised to find a much lower radiolabel
incorporation into ATP as compared to adenosine:
most of the newly formed IMP is probably degraded
to uric acid. The complete absence of a rise in inosine
and hypoxanthine above normal levels in tissue and
plasma with AICAR infusions is, however, difficult
to explain, and would suggest the possibility of a
route from AICAR to uric acid not encompassing
IMP. It also shows that the AICAR dose used is
appropriate for investigation of the effects of AI-
FIGURE 4. Panel a: AICAR infusion leads to a slow
time-dependent increase of plasma uric acid levels
with no statistical difference in left atrial and vena
cava inferior levels. After stopping AICAR infusion,
uric acid is slowly eliminated. (Statistics: 10 minutes and 30 minutes of AICAR infusion, P < 0.002
compared to control; 60-180 minutes of AICAR
infusion, P < 0.001 compared to control.) Panel b:
with intracoronary AICAR infusion, plasma AICAR
levels rise within the first hour of infusion. A
marked difference between left atrial and vena cava
inferior AICAR concentrations under steady state
conditions with no difference in uric acid levels
suggests peripheral uptake and kidney elimination
of unmetabolized AICAR. Stopping AICAR infusion
leads to a sharp fall of plasma AICAR concentrations.
60
CMIN:
CAR. A further increase of AICAR-MP concentration with higher AICAR concentrations would lead
only to a minimal increase in ATP formation. A
decrease in AICAR concentration leads to a decrease
in ATP formation as shown.
Studies with Adenosine
An increase of ATP in postischemic myocardium
is reported with adenosine as a precursor (Reibel
and Rovetto, 1979; Isselhard et al., 1980; Foker et
al., 1980). Since most of these studies have been
done in isolated rat or guinea pig hearts, no addition
of an inhibitor of adenosine deaminase for preventing adenosine deamination in blood (van Belle 1969)
was necessary. In a whole animal preparation, acceleration of ATP synthesis was successful only
when intravenous adenosine was given together
with EHNA (erythro-g-(2-hydroxy-3-nonyl)-adenine, a potent adenosine deaminase blocker. As far
as we know, adenosine was therefore not used to
replenish decreased ATP pools rapidly in regionally
ischemic and reperfused myocardium in the dog
heart. Foker's study (Foker et al., 1980) was done in
Mauser et al. /Acceleration of ATP Synthesis
Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017
the totally and globally ischemic heart within the
context of a cardioplegic study. Isselhard et al.
(1970b, 1980) studied adenosine either in postasphyxic rabbit hearts or in normal dog hearts. The
intracoronary administration of adenosine has the
advantage of partially bypassing the adenosine
deamination by blood which is correlated with contact time (van Belle, 1969). It leads only to minimal
adenosine concentrations in the peripheral tissues
after passing through the lungs, i.e., it does not
recirculate. This allows high local adenosine concentrations with only minor peripheral hemodynamic
changes. It cannot be ruled out that these hemodynamic changes may influence ATP catabolism; however, Isselhard (1980, 1984, in press) has shown
recently that the hemodynamic changes produced
by adenosine do not affect ATP synthesis. Since
myocardial oxygen consumption increases slightly
after adenosine infusion, due to an increase of heart
rate, there is probably an increase in ATP turnover.
This may lead to a small underestimation of accelerated ATP synthesis by adenosine. High tissue
adenosine levels demonstrate the uptake of adenosine from the blood. Increased inosine and hypoxanthine tissue levels show that part of the adenosine
is rapidly deaminated. The 3H incorporation found
in ATP after infusion of [3H]adenosine, as well as
the increase of total ATP from 50% postischemic to
75% of normal within 3 hours of reperfusion results
in a 90-fold increase of ATP synthesis compared to
the de novo synthesis. These incorporation rates are
comparable to those reported in studies with isolated
perfused hearts (Reibel and Rovetto, 1979; Isselhard
et al., 1980). Adenosine transformation to AMP is
catalyzed by the enzyme adenosine kinase which is
not an enzyme of the purine de novo synthesis
pathway. Incorporation of both ribose and AICAR
is dependent on the pre-existent purine de novo
synthesis pathway. However, ribose enters this
pathway after being converted to ribose-5 -phosphate and phosphoribosylpyrophosphate, at the beginning, and AICAR enters after conversion to AICAR-MP, near the end, of this pathway.
There seemed to be several rate-limiting steps.
One is the availability of phosphoribosylpyrophosphate which can be overcome by the infusion of
ribose. However, this can speed up the synthesis
only by a factor of five to six, which is minimal
compared to adenosine incorporation. Because of
the big difference in the incorporation rate of AICAR
and adenosine, there must also be a rate-limiting
step in the conversion of AICAR-MP to AMP. Since
there is no increase of AICAR-MP after ribose infusion, the capacity of the conversion of ribose-5phosphate to AICAR-MP seems also to be limited.
The conversion of phosphoribosylpyrophosphate to
IMP is dependent on ATP, which is needed at
several steps of this pathway. This seems to be no
problem, not even for the ATP-depleted cell, because ribose incorporation is doubled in postischemic tissue with lower ATP levels and there is
229
no big difference in the incorporation of ribose and
AICAR, whereas AICAR enters this pathway distal
to the ATP-dependent steps.
Each of the three tested substrates is able to restore
postischemic reduced myocardial ATP levels significantly faster than ATP-de novo synthesis, but there
are big differences in the extent of incorporation of
these precursors into the adenine nucleotide pool.
Adenosine is rapidly incorporated and leads to a
fast increase of tissue ATP levels within hours.
Incorporation of ribose or AICAR is much slower,
and a measurable increase of ATP levels in dog
myocardium would only be expected after 1-2 days.
The ability of fast restoration of ATP levels leads
to two questions that have to be resolved in further
experiments, i.e., (1) will reduced contractile function improve with higher ATP levels? and (2) will
partially restored myocardial ATP levels protect the
heart against recurrent episodes of ischemia?
Address for reprints: Dr. Manfred Mauser, Max-Planck-Institutc
for Physiological and Clinical Research, Department of Experimental
Cardiology, Benekestrasse 2, D-6350 Bad Nauheim, Federal Republic
of Germany.
Received May 20, 1983; accepted for publication October 31, 1984.
References
Belle van H (1969) Uptake and deamination of adenosine by
blood: Species differences, effect of pH, ions, temperature, and
metabolic inhibition. Biochim Biophys Acta 192: 124-132
Berne RM (1963) Cardiac nudeotides in hypoxia: Possible role in
regulation of coronary flow. Am J Physiol 204: 317-322
Bochner B, Ames BN (1982) ZTP (5-amino-4-imidazole carboxamide riboside 5'-triphosphate): A proposed alarmone for 10formyl-tetrahydrofolate deficiency. Cell 29: 929-937
Bretschneider HJ, Cott LA, Hensel I, Kettler D, Martel J (1970)
Ein neuer komplexer haemodynamischer Parameter aus 5 additiven Gliedern zur Bestimmung des CVBedarfs des linken
Ventrikels. Pflugers Arch 319: 14
Burdette W] (1956) Adenosine nucleotide levels in cardiac arrest.
Am Heart J S i 193-197
Chang I (1938) Effect of asphyxia on the adenosinetriphosphate
content of the rabbit heart. Q J Exp Physiol 28: 3
Danforth WH, Naegele S, Bing RJ (1960) Effect of ischemia and
reoxygenation on glycolytic reactions and adenosinetriphosphate in heart muscle. Circ Res 7: 965-971
DeBoer LMV, Ingwall JS, Kloner RA, Braunwald E (1980) Prolonged derangements of canine myocardial purine metabolism
after a brief coronary artery occlusion not associated with
anatomic evidence of necrosis. Proc Natl Acad Sci USA 77:
5471-5474
Ellis RJ, Gardner C (1980) Determination of myocardial highenergy phosphate using bioluminiscence. Anal Biochem 105:
354-360
Hwyn DH, Launder WJ, Parikh HC, Wise Jr EM (1972) Roles of
plasma and erythrocytes in interorgan transport of amino acids
in dogs. Am J Physiol 222: 1333-1342
Foker JE, Einzig E, Wang T (1980) Adenosine metabolism and
myocardial preservation. J Thorac Cardiovasc Surg 80: 506516
Fox AC, Reed GE, Meilman H, Silk BB (1979) Release of nudeosides from canine and human hearts as an index of prior
ischemia. Am J Cardiol 43: 52
Gerlach E, Deuticke B, Dreisbach RH (1963) Der Nukleotidabbau
im Herzmuskel bei Sauerstoffmangel und seine mogliche Bedeutung fur die Coronardurchblutung. Naturwissenschaft 50:
228-234
230
Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017
Hunkapillar MW, Hood LE (1978) Direct microsequence analysis
of polypeptides using an improved sequenator, a nonprotein
carrier (polybren), and high pressure liquid chromatography.
Biochemistry 17: 2124-2133
Ibel H, Steinkoff G, Zimmer HG (1982) Comparative studies on
the myocardial hexose monophosphate shunt in different animal species (abstr). Pflugers Arch 394: R13
Isselhard W, Pohl W, Berghoff WJW, Schmerbauch D, Schuler
HW (1964) Versuche zur Verbesserung der Energiebereitstellung im kiinstlich stillgestellten Herzen und in der Erholung
bei Reperfusion. Verh Dtsch Ges Herz Kreislaufforsch 30: 216221
Isselhard W, Maurer W, Stremmel W, Krebs J, Schmitz H, Neuhof
H, Esser A (1970a) Stoffwechsel der Kaninchenherzen in situ
wahrend Asphyxie und in der postasphyxtischen Erholung.
Pflugers Arch 316: 164-193
Isselhard W, Hinzen D, Geppert E, Maurer W (1970b) Beeinflussung des post-asphyktischen Wiederaufbaus der Adeninnukleotide im Kaninchenherzen in vivo durch Substratangebot.
Pflugers Arch 320: 195-209
Isselhard W, Eitenmiiller J, Maurer W, DeVreese A, Reineke H,
Czerniak A, Sturz J, Herb HG (1980) Increase in myocardial
adenine nucleotides induced by adenosine: Dosage, mode of
application and duration, species differences. J Mol Cell Cardiol
12: 619-634
Isselhard W, Hamaji M, Maurer W, Erkens H, Walter H (in press)
Adenosine-induced increase in myocardial adenine nucleotides
without adenosine-induced systemic hypotension. Basic Res
Cardiol 6
Kammermeier H (1964) Verhalten von Adenin-Nukleotiden und
Kreatinphosphat im Herzmuskel bei funktioneller Erholung
nach langer dauernder Asphyxie. Verh Dtsch Ges Herz Kreislaufforsch 30: 206-211
Kammermeier H, Karitzky D (1963) Verhalten von ATP und
Kreatinphosphat bei der Wiederbelebung des Myokards nach
langer dauemder Asphyxie. Pflugers Arch 178: 101
Katori M, Berne RM (1966) Release of adenosine from anoxic
heart: Relationship to coronary flow. Circ Res 19: 420
Kloner RA, Lawrence W, DeBoer V, Darsee JR, Ingwall JS, Hale
S, Tumas J, Braunwald E (1981) Prolonged abnormalities of
myocardium salvaged by reperfusion. Am J Physiol 241: H591H599
Maguire MH, Lukas MC, Rettie JF (1972) Adenine nucleotide
salvage synthesis in the rat heart, pathways of adenosine
salvage. Biochim Biophys Acta 262: 108-115
Parker JC, Smith EE, Jones CE (1976) The role of nucleoside and
nucleobase metabolism in myocardial adenine nucleotide regeneration after cardiac arrest. Circ Shock 3: 11-20
Reibel DK, Rovetto MJ (1979) Myocardial adenosine salvage rates
Circulation Research/VoZ. 56, No. 2, February 1985
and restoration of ATP content following ischemia. Am ]
Physiol 237: H247-H252
Reimer KA, Hill ML, Jennings RB (1981) Prolonged depletion of
ATP and of the adenine nucleotide pool due to delayed resynthesis of adenine nucleotides following reversible myocardial
ischemic injury. J Mol Cell Cardiol 13: 229-239
Rentrop P, Blanke H, Karsch KR, Kaiser H, Koestering H, Leitz K
(1981) Selective intracoronary thrombolysis in acute myocardial
infarction and unstable angina pectoris. Circulation 63: 307317
Sabina RL, Kernstine KH, Boyd RL, Holmes EW, Swain JL (1982)
Metabolism of 5-amino-4-imidazole carboxamide riboside in
cardiac and skeletal muscle. J Biol Chem 257: 10178-10183
Schaper J, Mulch J, Winkler B, Schaper W (1979) Ultrastructural,
functional and biochemical criteria for estimation of reversibility of ischemic injury: A study on the effects of global ischemia
on the isolated dog heart. J Mol Cell Cardiol 11: 521-541
Schmutzler R, Heckner F, Koertge P, van de Loo J, Pezold FA,
Poliwoda H, Praetorius F, Zekoth D (1966) Zur thrombolytischen Therapie des frischen Herzinfarktes. Dtsch Med Wochenschr 91: 581-587
Swain JL, Hines JJ, Sabina RL, Holmes EW (1982a) Accelerated
repletion of ATP and GTP pools in postischemic canine myocardium using a precursor of purine de novo synthesis. Circ
Res 51: 102-105
Swain JL, Sabina RL, McHale PA, Greenfield JC, Holmes EW
(1982b) Prolonged myocardial nucleotide depletion after brief
ischemia in the open-chest dog. Am J Physiol 242: H818-H826
Wyngarden A, Ashton DM (1959) Regulation of activity of phosphoribosylpyrophosphate amido-transferase by purine ribonucleotides: Potential feedback control of purine biosynthesis.
J Biol Chem 234: 1492-1496
Zimmer HG (1980) Restitution of myocardial adenine nucleotides:
acceleration by administration of ribose. J Physiol (Paris) 76:
769-775
Zimmer HG, Gerlach E (1978) Stimulation of myocardial adenine
nucleotide biosynthesis by pentose and pentitols. Pflugers Arch
376: 223-227
Zimmer HG, Trendelenburg C, Kammermeier H (1973) De-novosynthesis of myocardial adenine-nucleotides in the rat. Acceleration during recovery from oxygen deficiency. Circ Res 32:
635-642
Zimmerman PT, Deeprose RD (1978) Metabolism of 5-amino-l/3-D-ribofuranosyl imidazole-4-carboxamide and related fivemembered heterocycles to 5-triphosphates in human blood and
L 5178 Y cells. Biochem Pharmacol 27: 709-716
INDEX TERMS: Adenosine • AICAR • Ribose • ATP • Reperfusion
Influence of ribose, adenosine, and "AICAR" on the rate of myocardial adenosine
triphosphate synthesis during reperfusion after coronary artery occlusion in the dog.
M Mauser, H M Hoffmeister, C Nienaber and W Schaper
Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017
Circ Res. 1985;56:220-230
doi: 10.1161/01.RES.56.2.220
Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1985 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7330. Online ISSN: 1524-4571
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://circres.ahajournals.org/content/56/2/220
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in
Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further information
about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation Research is online at:
http://circres.ahajournals.org//subscriptions/