Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
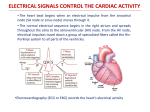
Chapter 23 Cardiac Rhythm Learning Objectives 1. What is the greatest extent of depolarization in the SA node? What are the three stages of the SA nodal cycle? -60 mV, at which point the phases begin, starting with… Phase 4: slow ramping up of depolarization; “inward current” (If) and outward K+ current (IK1) Phase 0: rapid depolarization mediated by voltage-gated Ca++ channels, and some Na+ too Phase 3: repolarization due to opening of K+ channels 2. What are the five phases of ventricular myocyte current? Phase 4: resting just above -94 mV Phase 0: INa Phase 1: early repolarization; opening of K+ channels (Ito) Phase 2: plateau; balance between Ca++ currents (ICa.T & ICa.L) and K+ currents (IK, IK1, Ito) Phase 3: late repolarization;decrease in Ca+ current and increase in K+ current 3. What determines the myocyte refractory period? The time it takes for Na+ channels to reset 4. Phase 2 Ca++ channels are sensitive to block by dihydropyridines, benzothiazepines, and phenylalkylamines 5. What is “afterdepolarization?” What drugs trigger early afterdepolarizations? What can these lead to? When a normal action potential triggers extra abnormal depolarizations—due to abnormal Ca++ current in the plateau phase (2) or Na+ current in phase 3 i. Delayed repolarization occurs just after completion of repolarization Drugs that prolong the QT interval, like class IA and III antiarrhythmics Torsades de pointes, an emergency which can end in fibrillation and death 6. What are the results of an accessory tract pathway? Wider QRS complex, early ventricular upstroke, re-entrant loops and tachyarrhymthias 7. What does state-dependent ion channel block mean? Na+ channel blockers (class I) tend to associate with channels during the open and inactive states, not with the resting/closed state This allows drugs to preferentialy act on ischemic/irritable tissue preferentially and block a arrhythmogenic focus at its source 8. 9. What ion channel or receptor does each of the four classes of antiarrhythmics block? I = Na+ II = β-adrenergic III = K+ IV = Ca++ [Nancy βakes Killer Cakes] What do Class I antiarrhythmics do? What are two general concerns you should have? Decrease automaticity in SA nodal cells by shifting threshold potential positively and reducing slope of (atrial!) phase 4 (depolarization) Decrease heart rate; Greater voltage needed for defibrillaors Also increase refractory period and slow conduction velocity in ventricles 10. What extra activity do type IA antiarrhythmics have? What are the three drugs? K+ blocking in ventricles => slow repolarization and longer plateau Quinidine, procainamide, and disopyramide [QUeeN DISO’s PYRAMID of coCAINe] 11. What is special about quinidine, or rather, especially bad (4 things)? How can this be partially fixed with other drugs? Anticholinergic effect=> increased conduction through AV node=> ventricular fibrillation in people with atrial fibrillation; 1:1 A:V firing ratio is established in contrast to former 2:1 or 4:1 Use β-adrenergic antagonists or verapamil Other side effects are torsades de pointes, powerful diarrhea, nausea, headache, and dizziness, the last four make it hard for patients to take long term Increases blood levels of digoxin 12. What are the adverse effects of procainamide? Eventually produces a Lupus-like syndrome, and has active metabolite NAPA with class III effects: prolongs QT interval and refractory period 13. What is the major drawback of disopyramide? When should it be avoided? Special app? Even worse anticholinergic effects than quinidine: do not administer to those with obstructive uropathy, glaucoma, conduction block, sinus node dysfunction, or decompensated HF hypertrophic obstructive cardiomyopathy, we dunno why 14. What is the added effect of IB antiarrhythmics? What is another useful feature? 3 drugs? shorten repolarization Use-dependent block; greatest effect on cells firing more frequently, little effect on normal cardiac tissue Lidocaine, mexiletine, and phenytoin [LIDdy’s PHamous MEXIcan] 15. When is lidocaine used? When should you adjust the dose? Main location of adverse effects? Ventricular arrhythmias in emergencies Give less to patients with poor liver flow or inhibited P450 enzymes CNS effects: confusion, dizziness, and seizures i. notably free of long QT syndrome 16. What drugs is mexiletine usually combined with (3)? When is phenytoin used? Amiodarone, in patients with implantable cardioverter-defibrillators (pacemakers) and Vtach Quinidine or sotalol to increase efficacy and reduce adverse effects Phenytoin is great for children with ventricular arrhythmias, esp. prolonged QT and after congenital heart surgery 17. How do class IC drugs change the action potential? 3 drugs? Markedly decrease the rate of phase 0 upstroke of ventricular cells i. Suppresing ventricular contractions, plus supraventricular contractions Flecainide, encainide, and moricizine [MORtuary FLECks ENCased, all have a “c”] 18. What are class IC drugs’ major drawbacks? When may they be used? Sinus node dyfunction, decreased conduction velocity, and conduction blcok Approved only when other measures fail, in life-threatening situations 19. How do β1 antagonists affect the action potentials of SA and AV nodes? What receptor subtypes does propanolol work on? How about labetalol and carvedilol? What are class II adverse effects? Lengthens SA nodal depolarization (phase 4); Lengthens AV nodal repolarization (phase 3) [LAVeNdeR & SAND at the βeach] Nospecific antagonist for β1 or β2 β1 antagonists, α antagonists too i. most others are just β1 antagonists β2-antagonist-induced vasospasm: cold extremities, impotence; “overdose:” negative inotropy, heart block; CNS penetration: insomnia, depression 20. What are the big positive and negative of class III antiarrhymics? What’s another general negative? K+ blocking prolongs repolarization and plateau: i. Increases refractory period, and decreasing re-entry ii. Increases likelihood of afterdepolarizations and so torsades de pointes All except amiodarone show reverse use-dependency 21. When is ibutilide used? What is its serious adverse effect? Terminate atrial fib and flutter Torsades de pointes, like all drugs with class III activity 22. Dofetilide: Oral only; only used for highly symptomatic atrial fib and flutter because of its potential to cause arrhythmias 23. What class is sotalol? Uses? Mixed II and III Ventricular arrhythmia, atrial fluter and fibrillation 24. How do you classify bretylium? What drug and intervention should you try first? Class III and antihypertensive agent Only used after lidocaine and defibrillation have failed to treat V tach or fibrillation 25. Which drug has activity akin to all classes of antiarrhytmics? What are its 2 uses? Major side effects? What is its shady friend? Amiodarone; alters the lipid membrane Preventing ventricular arrhymias in patients with HF or MI, preventing paroxysmal atrial fibrillation or flutter Pneumonitis=> pulmonary fibrosis; hyper/hypothyroidism; α-antagonist=> hypotension Dronedarone, mostly untrustworthy 26. What is the major therapeutic action of class IV drugs? Which have greater activity in vascular smooth muscle, and which in the atria? They slow conduction through the AV node Dihydropyridines like nifedipine Verapamil and diltiazem treat Afib and SVT i. Note that these guys are also sometimes used in V tach 27. What drug opens G protein-coupled K+ channels, limits conduction, and treats paroxysmal supraventricular tachycardia as a first line agent? adenosine 28. What’s a great drug for chronic refractory angina pectoris? Ranolazine Biochem 47 crossover: inhibits partial fatty acid oxidation (pFOX) after an ischemic episode and prevents buildup of lactic acid This isn’t relaly necessary now Afib quinidine, disopyramide, encainide2, flecainide2, moricizine2, ibutilide, dofetilide, amiodarone, dronedarone, verapamil, diltiazem SVT quinidine, disopyramide, encainide2, flecainide2, moricizine2, amiodarone, adenosine, verapamil, diltiazem PACs quinidine PVCs quinidine, procainamide, disopyramide, lidocaine? phenytoin? sotalol? Bretylium? VT procainamide, disopyramide, encainide, flecainide, moricizine, amiodarone, lidocaine Vfib lidocaine? phenytoin? sotalol? amiodarone Hypertension, angina, & HF B-blockers, diltiazem, verapamil Quinidine moricizine flecainamide ibutilide dronedarone lidocaine procainamide disopyramide bretylium amiodarone mexiletine encainamide phenytoin dofetilide sotalol all drugs in the IC class have one “c”