Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
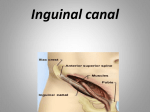
Inguinal canal It is an obligue passage through the lower part of the anterior abdominal wall and is present in both sexes. It transmits the ilioinguinal nerve in both sexes In female it transmits the round ligament from the uterus to the labia majora. In male, It allows structures to pass to and from the testis to the abdomen. It is about 1.5 inch ( 4cm ) long in the adult and extends from the deep inguinal ring downward & medially to the superficial inguinal ring. It lies parallel to and immediately above the inguinal ligament. The deep inguinal ring, is an opening (a hole ) in the fascia transversalis. It lies about 0.5 inch (1.3 cm ) above the inguinal ligament midway between the anterior superior iliac spine & the symphysis pubis. Related to it medially are the inferior epigastric vessels, which pass upward from the external iliac artery. The margins of the ring give attachment to the internal spermatic fascia or the internal covering of the round ligament of the uterus. In the newborn child, the deep ring lies directly posterior to the superficial ring. So it is shorter at this age and as the result of growth it moves laterally. The superficial inguinal ring is a triangular shaped defect in the aponeurosis of the external oblique muscle. it lies immediately above & medial to the pubic tubercle. The margins of the ring called the crura & give attachment to the external spermatic fascia. Walls of the Inguinal Canal Anterior wall is formed along its entire length by the aponeurosis of the external oblique muscle. It is reinforsed in its lateral third by the origin of the internal obligue from the inguinal ligament. This wall is strong. It lies opposite the weakest part of the posterior abdominal wall (deep inguinal ring ). Posterior wall is formed along its entire length by the fascia transversalis. It is reinforsed in its medial third by the conjoint tendon ( common tendon of insertion of the internal oblique & transversus which is attached to pubic crest. & petineal line ). This wall is strong. it lies opposite the weakest part of the anterior wall, the superficial inguinal ring. The inferior wall or floor of the canal is formed by the rolled –under inferior edge of the aponeurosis of the external oblique muscle, namely, the inguinal ligament & at its medial end , the lacunar ligament. The superior wall or roof of the canal is formed by the arching lowest fibers of the internal oblique & transversus abdominis muscles. Function of the inguinal canal It allows structures of the spermatic cord to pass to & from the testis to the abdomen in the male. In the female, the canal is smaller than male it permits the passage of the round ligament of the uterus from the uterus to the labia majora. In both sexes, the canal permits the passage of the ilioinguinal nerve. Mechanism of inguinal canal 1- It is an oblique canal with weak superficial & deep rings. 2- The anterior wall is reinforced by the fibers of the internal oblique muscle immediately in front of the deep ring. 3- The posterior wall of the canal is reinforced by the strong conjoint tendon immediately behind the superficial ring. 4- On coughing; straining; the arching lowest fibers of the internal obligue & transversus abdominis muscles flattening out the arched roof . So, the roof compress the contents of the canal against the floor, so, the canal is closed. 5- In defecation & parturition ( great straining ) the person must tend to squatting position, the hip joint is flexed & the anterior surfaces of the thigh are brought up against the anterior abdominal wall. So the anterior abdominal wall is protected by the thighs. The testis descends behind the peritoneum, dragging its blood ; nerve supply and lymphatic drainage after it. Before the descent of the testis and ovary from the level of L1 a peritoneal diverticulum called the processus vaginalis is formed. During its passage in the deep inguinal ring it traverses the fascia transversalis and acquires a tubular covering ( internal spermatic fascia ). A band of mesenchyme extending from the lower pole of the developing gonad through the inguinal canal to the labioscrotal swelling has condensed to form the gubernaculum. From the internal oblique it takes the cremaster muscle. It passes under the arching of the transversus abdominis so, it does not acquire a covering from it. On reaching external oblique, it invaginates it to form the superficial inguinal ring and acquires the external spermatic fascia. N.B. In the female the term spermatic fascia is replaced by the covering of the round ligament of the uterus Abdominal Herniae The hernial sac is a pouch ( diverticulum ) of the peritoneum and has a neck and body The hernial contents may consists of any structure found within the abdominal cavity and may be a small piece of omentum to a viscus like kidney. The hernial coverings are formed from the layers of the abdominal wall . Indirect Inguinal Hernia It is believed to be congenital. It is common. The hernial sac is the remains of the processus vaginalis ( an outpouching of peritoneum that in the fetus is responsible for the formation of the inguinal canal The Sac enters the deep inguinal ring lateral to the inferior epigastric vessels. On reaching the hernial sac to the superficial inguinal ring, the neck will lay in the deep inguinal ring. The neck is narrow The hernial sac may extend down into the scrotum or labia majora. It is more common than a direct inguinal hernia. It is more common in male than female ( 20 times ). It is more common on the right side ( the right testis descends later than the left ) It is more common in young adults and children. Nearly one third are bilateral The hernial sac may extend through the superficial inguinal ring above and medial to the pubic tubercle. Direct Inguinal Hernia It makes up 15% of all inguinal hernia. The sac bulges directly anteriorly through the posterior wall of the inguinal canal medial to the inferior epigastric vessels. The neck of it is wide because it is nothing more than a generalized bulge. It is rare in women and most are bilateral. It is a disease of old men with weak abdominal muscles. Spermatic Cord It is a collection of structures that pass through the inguinal canal to and from the testis. It is covered by 3 concentric layers of fascia derived from the layers of the anterior abdominal wall. It begins at the deep inguinal ring lateral to the inferior epigastric artery&ends at the testis Structures of the Spermatic Cord 1.Vas deferens 2 . Testicular artery .1 3.Testicular veins ( pampiniform plexus ) 4.Testicular lymph vessels 5.Autonomic nerves, sympathetic fibers ( run with the testicular artery) from the renal or aortic sympathetic plexuses. Afferent sensory nerves accompany the efferent sympathetic fibers. 6.cremasteric artery is a branch of the inferior epigastric artery. 7. Remains of processus vaginalis 8. Artery of vas deferens, is a branch of inferior vesical artery. 9. Genital branch of the genitofemoral nerve supplies cremaster muscle. Vas deferens, is a cordlike structure that can be palpated between finger & thumb in the upper part of the scrotum. It is a thick walled muscular duct that transport spermatozoa from epididymis to the urethra. Testicular Artery, is a branch of the abdominal aorta at the level of the 2nd lumbar vertebra. It is long & slender and descends on the posterior abdominal wall. It traverses the inguinal canal & supplies the testis & epididymis. Testicular Veins, The pampiniform plexus is an extensive venous plexus which leaves the posterior border of the testis. As it ascends, it become reduced in size so that at about the level of the deep inguinal ring, a single testicular vein is formed. This vein runs up on the posterior abdominal wall & drains into the left renal vein on the left side & into the inferior vena cava on the right side. Covering of the spermatic cord 1- External spermatic fascia is derived from the external oblique aponeurosis and attached to the margins of the superficial inguinal ring. 2- Cremasteric fascia is derived from the internal oblique muscle. 3- Internal spermatic fascia is derived from the fascia transversalis and is attached to the margins of the deep inguinal ring. Scrotum It is outpouching of the lower part of the anterior abdominal wall. It contains the testes, epididymis & the lower end of the spermatic cords. Its wall has the following layers: 1. skin 2. superficial fascia 3. dartos muscle( smooth m. ) replacing fatty layer. 4. external spermatic fascia 5. cremasteric fascia 6. internal spermatic f. 7. tunica vaginalis which is a closed sac invaginated from behind by the testis. It lies within the spermatic fasciae and covers the anterior, medial & lateral surfaces of the testis. Skin It is thin, wrinkled, pigmented and forms a single pouch. Superficial fascia It is continuous with the fatty & membranous layers of the anterior abdominal wall. The fat is replaced by smooth muscle called dardos muscle which is innervated by sympathetic nerve fibers & is responsible for wrinkling of the overlying skin. The membranous layer ( Colles’ fascia ) is continuous in front with the membranous layer of the anterior abdominal wall ( Scarpa’s fascia ) & behind it is attached to the perineal body & the posterior edge of the perineal membrane. At the sides it is attached to the ischiopubic rami. Both layers of the superficial fascia contribute to a median partition that crosses the scrotum and separates the testes from each other. Spermatic fasciae They lie beneath the superficial fascia & are derived from the 3 layers of the anterior abdominal wall on each side. Cremasteric muscle It can be made to contact by stroking the skin on the medial aspect of the thigh. This called cremasteric reflex . The afferent fibers of this reflex arc travel in the femoral branch of the genitofemoral nerve ( L 1 &2 ) & the efferent motor fibers travel in the genital of the genitofemoral nerve. The function of this reflex is to raise the testis & scrotum upward for warmth and for protection against injury. Testis It a firm, mobile organ lying within the scrotum. The left testis lies at a lower level than the right.The upper pole of the gland is tilted forward. Each testis is surrounded by a tough fibrous capsule ( tunica albuginea ). Extending from the inner surface of the capsule is a series of fibrous septa that divide the interior of the organ into lobules. Lying within each lobule are 1 to 3 coiled seminiferous tubules. The tubules open into a network of channels called the rete testis. Efferent ductules connect the rete testis to the upper end of the epididymis. Normal spermatogenesis can occur only if the testes are at a temperature lower than that of the ْabdominal cavity ( 3 C lower than the abdominal temperature ) . Epididymis It is a firm structure lying posterior to the testis with the vas deferens lying on its medial side. It has an expanded upper end, the head, a body and a pointed tail inferiorly. Laterally a distinct groove lies between the testis and the epididymis which is lined with the inner visceral layer of the tunica vaginalis and is called the sinus of the epididymis . It is a coiled tube 6 m ( 20 ft ) long and embedded in connective tissue. The tube emerges from the tail of the epididymis as the vas deferens which enters the spermatic cord. The long length of it , allows the storage & maturation of the sperm . A main function of it, is the absorption of fluid & the addition of substances to the seminal fluid to nourish the maturing sperm Blood supply of testes & Epididymis The testicular artery is a branch of the abdominal aorta. The testicular veins emerges from the testis & the epididymis as a venous net ( the pampiniform plexus ) . This plexus becomes reduced to a single vein as it ascends through the inguinal canal. The right testicular vein drains into the inferior vena cava . The left testicular vein joins the left renal vein. Lymph Vessels 1- Spermatic cord The testicular lymph vessels ascend through the inguinal canal & pass up over the posterior abdominal wall to reach the lumbar ( para- aortic ) lymph nodes on the side of the aorta at the level of the 1st lumbar vertebra. 2- Scrotum lymph from the skin & fascia including the tunica vaginalis drains into the superficial inguinal lymph nodes. 3- Testis & Epididymis The lymph vessels ascend in the spermatic cord & end in the lymph nodes on the side of the aorta, para- aortic or lumbar nodes at the level of the 1st lumbar vertebra. Tapping a hydrocele Processus Vaginalis Normally, its upper part becomes obliterated just before birth and the lower part remains as the tunica vaginalis. - It may persist as a preformed hernial sac for an indirect inguinal hernia. - Its lumen remains in communication with the abdominal cavity. Peritoneal fluid accumulates in it, forming a congenital hydrocele. - The upper & lower ends are oblitrated leaving intermediate encysted hydrocele of the cord. - Inflammation of the testis cause an accumulation of the fluid within the tunica vaginalis. Most hydroceles are idiopathic. Varicocele The veins of the pampiniform plexus are elongated and dilated. It is common in adolescents and young adults. It is more of the left side. This is due to, the left testicular vein joins the left renal vein in which the venous pressure is higher. Rarely, malignant disease of the left kidney extends along the renal vein and blocks the exit of the testicular vein. So, a rapidly developing left- sided varicocele should therefore always lead one to examine the left kidney. Malignant Tumor of the Testis It spreads up via the lymph vessels to the para- aortic ( lumbar ) lymph nodes at the level of L1 vertebra. When the tumor spreads locally to involve the tissues and skin of the scrotum, the superficial inguinal lymph nodes are involved. Torsion of the Testis It is a rotation of the testis around the spermatic cord within the scrotum. It is often associated with an excessively large tunica vaginalis. It common occurs in active young men and children. It is accompanied by severe pain. If not treated quickly, the testicular artery may be occluded followed by necrosis of the testis.