Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Television standards conversion wikipedia , lookup
Charge-coupled device wikipedia , lookup
Mechanical television wikipedia , lookup
Oscilloscope types wikipedia , lookup
Battle of the Beams wikipedia , lookup
Oscilloscope history wikipedia , lookup
Analog-to-digital converter wikipedia , lookup
Analog television wikipedia , lookup
Index of electronics articles wikipedia , lookup
Video camera tube wikipedia , lookup
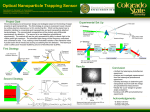
Computed Radiography: Acceptance Testing and Quality Control Introduction CR is the primary means to capture 2D images in a PACS environment • Acceptance testing validates performance • Quality control verifies optimal operation J. Anthony Seibert, Ph.D. University of California Davis Department of Radiology Sacramento, California Considerations: • Knowledge of CR attributes and operation • Understanding the tests • Determining appropriate results Presentation Outline Computed Radiography (CR) ...is the generic term applied to an imaging system comprised of: Overview of CR How does it work? What are the issues? Photostimulable Storage Phosphor to acquire the xx-ray projection image Acceptance test procedures What tests? Why? Quality control When ? CR Reader How? to extract the electronic latent image Digital electronics to convert the signals to digital form What? How often? CR Image Acquisition 1. X-ray Exposure Patient 5. unexposed 2. Image Reader X-ray system 2. Display 3. Image Scaling Computed Radiograph 1. Acquisition Digital to Analog Conversion Transmitted xx-rays through patient Digital processing 4. Image Record Analog to Digital Conversion exposed Phosphor plate Digital Pixel Matrix Charge collection device X-ray converter x-rays → electrons 3. Archiving Computed Radiography: Acceptance Testing and Quality Control -- J.A. Seibert, Ph.D. 1 CR Networking Film laser printer CR Reader • PACS and DICOM – Digital Imaging COmmunications in Medicine – Provides standard for modality interfaces, storage/retrieval, and print • Modality Worklist Input (from RIS via HLHL-7) DICOM • Technologist QC Workstation – Image manipulation and processing – Processed / Unprocessed images CR - QC Workstation • DICOM image output PACS SoftSoft-copy review Stimulation and Emission Spectra CR: How does it work? Photostimulated Luminescence t recombination 4f 6 5d F/F+ PSL 3.0 eV t e- Laser stimulation Energy Band BaFBr 8.3 eV 2.0 eV Eu Emission Optical Barrier Conduction band tunneling Relative intensity t phonon BaFBr: Eu2+ Stimulation 1.0 0.5 Diode 680 nm 4f 7 Eu 3+ / Eu 2+ Incident x-rays e Valence band PSLC complexes (F centers) are created in numbers proportional to incident xx-ray intensity 0.0 800 1.5 PSL Signal PMT Exposed Imaging Plate Light Scattering Photostimulated Luminescence Protective Layer 2 f-θ lens Laser Source Polygonal Mirror Laser beam: Scan direction Phosphor Layer Laser Light Spread "Effective" readout diameter 1.75 Reference detector Light guide 600 500 2.5 400 300 3 4 λ (nm) Energy (eV) CR: Latent Image Readout Photostimulated Luminescence Incident Laser Beam 700 Base Support Cylindrical mirror Light channeling guide Output Signal PMT ADC ADC x= 1279 To1333 image y= processor z= 500 Plate translation: SubSub-scan direction Computed Radiography: Acceptance Testing and Quality Control -- J.A. Seibert, Ph.D. 2 Phosphor Plate Cycle PSP SubSub-scan Direction Typical CR resolution: Base support x-ray exposure Plate translation reuse 35 x 43 cm -- 2.5 lp/mm (200 µm) 24 x 30 cm -- 3.3 lp/mm (150 µm) 18 x 24 cm -- 5.0 lp/mm (100 µm) plate exposure: create latent image laser beam scan plate readout: extract latent image light erasure Screen/film resolution: Laser beam deflection plate erasure: remove residuals 7-10 lp/mm (80 µm - 25 µm) Computed Radiography • Acquisition, Display and Archive are separate functions • Variable speed detector – 20 to 2000 speed • Wide dynamic range – 0.01 to 100 mR Exposure Latitude: Dynamic Range Film Signal output Scan Direction CR 100:1 10000:1 • Image processing is a crucial requirement Log relative exposure Raw image Processing the Image • Image prepre-processing • Inherent subject contrast displayed – Find pertinent image information (histogram analysis) – Scale data to an appropriate range • Contrast inverted (to screenscreen-film) • Contrast enhancement • PSL signal amplitude log amplified • Spatial frequency enhancement – Anatomy specific grayscale manipulation Computed Radiography: Acceptance Testing and Quality Control -- J.A. Seibert, Ph.D. 3 Histogram analysis Finding the Image Location • Frequency distribution of pixel values within a defined area in the image • Image recognition phase – Collimation (Agfa) – EDR, automatic mode (Fuji) • Shape is anatomy specific – Segmentation (Kodak) • Sets minimum and maximum “useful” pixel values • Finding collimation borders and edges Histogram: Frequency 1 4 4 4 1 4 2 2 2 4 4 2 3 2 4 4 2 2 2 4 1 4 4 4 1 Frequency Histogram Distribution frequency distribution of pixel values in an image 16 14 12 10 8 6 4 2 0 0 1 2 Value Pixel value Useful signal The shape is dependent on radiographic study, positioning and technique 1023 Frequency of Digital Number Direct x-ray area Frequency Anatomy 5 Histogram Distribution Histogram Distribution Collimated area 3 4 Value Q2 Digital value 511 S1 0.01mR 0.1mR SK 1mR Q1 0 S2 10mR 100mR Latitude (L) 20000 2000 200 20 2 Sensitivity (S) Computed Radiography: Acceptance Testing and Quality Control -- J.A. Seibert, Ph.D. 4 Data conversion Input to output digital number 1,000 102 101 100 10-1 511 1023 10-1 100 101 102 103 0 Raw Digital Output Exposure input min 600 400 200 0 600 400 200 200 600 1,000 Input digital number 0 0 max 1. Find the signal 2. Scale to 3. Create film range to 8323 to 9368 800 800 Frequency Output digital number Relative PSL Exposure into digital number Histogram Histogram: pediatric image Grayscale transformation 200 400 600 800 1000 Digital value Useful image range for anatomy looklook-alike Data conversion for overexposure Exposure into digital number Relative PSL Reduce overall gain 102 101 100 10-1 Exposure input PrePre-processed “raw” image Scaled and inverted: “unprocessed” image 10-1 100 101 102 0 511 1023 Raw Digital Output overexposure Screen-Film Underexposed 103 min max (scaled and log amplified) Computed Radiography Overexposed Underexposed Overexposed Computed Radiography: Acceptance Testing and Quality Control -- J.A. Seibert, Ph.D. 5 Data conversion for wide latitude ScreenScreen-Film 80 kVp, 18 mAs Exposure into digital number CR 80 kVp, 64 mAs 80 kVp, 18 mAs Change gradient (auto mode) Relative PSL 102 101 100 10-1 Exposure input 10-1 100 101 102 103 low kVp (wide range) 0 511 1023 Raw Digital Output (scaled and log amplified) min 400 speed screen - film max L=4, wide latitude LookLook-upup-table transformation Contrast Enhancement 1,000 Output digital number • Optimize image contrast via nonnon-linear transformation curves • Unprocessed images display linear “subject contrast” – “Gradation processing” (Fuji) – “Tone scaling” (Kodak) – “MUSICA” (Agfa) M E L A 800 600 GT Gradient Type Fuji System Example LUTs 400 200 0 0 200 400 600 800 1,000 Input digital number Spatial Frequency Processing “Edge Enhancement” Response Solid: Original originalMTF response Edge Enhanced: Difference: Dash: low pass filtered Difference Original Original - + filtered Raw Unprocessed Contrast Enhanced Sum low low low Original Blurred high high high Spatial frequency Difference Edge enhanced Computed Radiography: Acceptance Testing and Quality Control -- J.A. Seibert, Ph.D. 6 Fuji CR Parameter Settings LUT shape parameters Anatomy Anatomical region General chest (LAT) General chest (PA) Port Chest GRID Port Chest NO GRID Peds chest NICU/PICU Finger Wrist Forearm Plaster cast (arm) Elbow* Upper Ribs* Pelvis* Pelvis portable Tib/Fib Tib/Fib Foot Foot* Os Calcis Foot cast C-spine T-spine Swimmers Lumbar spine Breast specimen GA 1.0 0.6 0.8 1.0 1.1 0.9 0.8 0.8 0.8 0.8 0.8 0.9 0.9 0.9 0.8 1.2 0.8 0.8 1.1 0.8 1.2 1.0 2.5 GT B D F D D O O O O O O O O N O N O O F F J N D GC 1.6 1.6 1.8 1.6 1.6 0.6 0.6 0.6 0.6 0.6 1.6 0.6 0.6 0.6 0.6 0.6 0.6 0.6 0.6 1.8 0.9 0.9 0.6 Frequency enhancement parameters GS -0.2 -0.5 -0.05 -0.15 -0.2 0.3 0.2 0.3 0.4 0.4 0.0 0.2 0.2 0.25 0.3 -0.05 0.4 0.5 0.5 -0.05 0.3 0.4 0.35 RN 4.0 4.0 4.0 4.0 3.0 5.0 5.0 5.0 5.0 7.0 5.0 6.0 4.0 5.0 5.0 7.0 5.0 5.0 5.0 4.0 5.0 5.0 9.0 RT R R T R R T T T T T R T T F T T F F P T T T P Recommended Acceptance Tests • Physical Inspection– Inspection–Inventory– Inventory–PACS Interfaces RE 0.2 0.2 0.2 0.5 0.5 0.5 0.5 0.5 0.5 1.0 1.0 1.0 0.5 0.5 0.5 0.5 1.0 0.5 0.5 0.2 0.5 1.0 1.0 Acceptance Test / QC considerations • Image acquisition • ElectroElectro-Mechanical readout • Image processing • PACS / RIS interfaces • Image handling Recommended Acceptance Tests • Noise / LowLow-Contrast Response • Imaging Plate Uniformity and Dark Noise • Distortion • Signal Response: Linearity and Slope • Erasure Thoroughness • Signal Response: Exposure calibration and beam quality • Artifact Analysis: Hardware/Software • Laser Beam Function • Positioning and collimation robustness • High Contrast Resolution • Imaging Plate Throughput Acceptance test tools required CR: Spatial Resolution • Phosphor plate sizes: impact on resolution • Exposure meter/dosimeter • Spatial resolution phantom • Low contrast phantom • Vendor QC phantom (periodic tests) • SMPTE test pattern • Anthropomorphic phantom • Documentation log / spreadsheet / instructions 35x43 (14x17) 24x30 (10x12) 18x24 (8x10) 0.2 mm pixels 0.14 mm pixels 0.1 mm pixels Computed Radiography: Acceptance Testing and Quality Control -- J.A. Seibert, Ph.D. 7 High Contrast (Spatial) Resolution 18 x 24 cm MTF Curves 35 x 43 cm 1 MTF 0.8 PrePre-sampled MTF ScreenScreen-film 0.6 Scan Subscan 0.4 Sampled MTF: Standard CR 0.2 2K x 2K matrix 35 x 43 cm 0 Photon absorption fraction 0 2 4 6 8 10 Spatial Frequency (lp/mm) Low Contrast Response: Leeds TOTO-16 X-ray Absorption Efficiency 1 Hi res CR Standard CR BaFBr, 100 mg/cm² 0.8 Gd2O2S, 120 mg/cm2 0.6 0.4 0.2 BaFBr, 50 mg/cm² 0 0 20 40 60 80 100 120 140 Energy (keV) 3.5 mR 70 kVp 0.5 mR Uniformity 498 508 537 490 497 10 mAs 480 513 505 544 487 20 mAs Computed Radiography: Acceptance Testing and Quality Control -- J.A. Seibert, Ph.D. 8 Radiation Dose for CR Sensitivity number, S • Variable Speed Detector • Estimate of the incident exposure on the IP • Optimal dose (UC Davis) – Adult chest image: – Neonates/pediatrics: – Extremities: • Comparable to screenscreen-film “speed” S=200S=200-300 S=400S=400-600 S= 7575-100 • Amplification required to map median value of histogram to 511 (0 to 1023 grayscale) – Lower detection efficiency, luminance and readout noise • Dependent on histogram shape and examination selected • AntiAnti-scatter grids needed Date: 7/10/98 Date: 7/10/98 Medical Medical Physicist: Physicist: Anthony Anthony Seibert, Seibert, Ph.D. Ph.D. Location: Location: System System Identification: Identification: UCDMC, UCDMC, ACC, ACC, 33 CR CR unit unit 33 Guidelines for QC based on Exposure UC UC Davis Davis Medical Medical Center Center CR CR Reader Reader and and Screens Screens Signal Signal Response: Response: Calibration Calibration and and Beam Beam Quality Quality Sensitivity number Note: Note: Use Use mAs mAs values values to to provide provide an an approximate approximate exposure exposure of of 11 mR mR to to the the IP. IP. Menu Menu == TEST TEST IP ST14x17 14x17 IP Type: Type: ST IP IP SN: SN: Exposure Exposure Conditions Conditions SubMenu SubMenu==Ave Ave2.0 2.0 Focal Focalspot spot Time Timedelay delay SID SID(cm) (cm) SMD SMD(cm) (cm) LL == 2, 2, EDR EDR == semi semi 1.2 1.2 mm mm ~2 ~2 min min 140 140 130 130 kVp kVp Dependency Dependency kVp kVp Filtration Filtration m mAs As m mR-m R-meter eter 60 60 80 80 115 115 11 Al/0.5 Al/0.5 Cu Cu 11 Al/0.5 Al/0.5 Cu Cu 11 Al/0.5 Al/0.5 Cu Cu 15.00 15.00 4.5 4.5 1.13 1.13 1.06 1.06 1.06 1.06 1.14 1.14 Filtration Filtration m mAs As m mR-m R-meter eter 80 80 80 80 80 80 none none 11 Al/0.5 Al/0.5 Cu Cu 1Al/2.5Cu 1Al/2.5Cu 0.50 0.50 4.50 4.50 60.00 60.00 0.96 0.96 1.06 1.06 0.99 0.99 <0.2 mR • Underexposed: repeat 0.30.3-0.2 mR • Underexposed: QC exception OD OD 1.41 1.41 1.38 1.38 1.45 1.45 0.07 0.07 NA NA NA NA NA NA NA NA • 300 - 600 1.01.0-0.3 mR • Underexposed: QC review SS SS (1mR) (1mR) 0.83 187.00 154.79 0.83 187.00 154.79 0.91 108.00 98.71 0.91 108.00 98.71 0.85 124.00 105.85 0.85 124.00 105.85 Maximum Maximum Difference: Difference: 56.08 56.08 OD OD 1.40 1.40 1.38 1.38 1.40 1.40 0.02 0.02 NA NA NA NA NA NA NA NA NA NA • 150 - 300 1.31.3-1.0 mR • Acceptable range • 75 -150 1.31.3-2.7 mR • Overexposed: QC review • 50 - 74 4.04.0-2.7 mR • Overexposed: QC exception • <50 >4.0 mR • Overexposed: repeat m mR-IP R-IP NA NA 180.00 180.00 160.00 160.00 120.00 120.00 100.00 100.00 140.00 140.00 120.00 120.00 Response sponse Re Response Response 80.00 80.00 100.00 100.00 80.00 80.00 60.00 60.00 40.00 40.00 60.00 60.00 40.00 40.00 20.00 20.00 0.00 0.00 50 50 • >1000 • 600 – 1000 SS SS (1mR) (1mR) 0.91 121.00 110.59 0.91 121.00 110.59 0.91 108.00 98.71 0.91 108.00 98.71 0.98 115.00 113.04 0.98 115.00 113.04 Maximum Difference: 14.33 Maximum Difference: 14.33 m mR-IP R-IP Filtration Filtration Dependency Dependency kVp kVp Indication SS(1mR) (1mR) 70 70 90 90 kVp kVp 110 110 130 130 20.00 20.00 0.00 0.00 none none SS(1mR) (1mR) 11 Al/0.5 Al/0.5 Cu Cu Filtrati Filtration on 1Al/2.5Cu 1Al/2.5Cu Sensitivity number, S • Imaging plate (HR vs. ST) differences • Examination specific histogram shapes – S number varies with examination type • EDR mode effects – Automatic (determines S1 and S2 values on histogram) – SemiSemi-automatic (average value within ROI) – Fixed (system acts like screenscreen-film detector) • X-ray beam spectrum effects What S value is appropriate? • Determined by examination – Adult exams (CXR, abdomen, etc) – Extremities (ST plates) – Pediatrics UCDMC targets 150 – 300 75 – 150 300 – 600 • CR’s variable speed should be used to advantage • Anatomical information can be lost with too high or too low exposure – S number varies with beam hardness (calibration required) Computed Radiography: Acceptance Testing and Quality Control -- J.A. Seibert, Ph.D. 9 Adult portable chest calculated exposures First half, 1994, 4572 exams 38.3% 600 53.9% 7.8% Adult portable chest calculated exposures Second half, 1994, 4661 exams Target exposure range 600 500 3.4% Q3 300 Q4 Target exposure range Low High Low Incident Exposure Other 12% “Exposure Creep” 180 180 160 160 140 140 120 120 100 100 80 80 60 60 40 40 20 20 0 0 <50 System speed (S #) Incident Exposure April 1 - 17, 1996 Adult Portable Chest 100 <50 100 200 300 0 400 100 0 200 200 100 300 200 400 400 Q2 500 300 #exams Q1 System speed (S #) Grid technique without a grid >>1 100 000 6600 00-6699 99 5500 00554 99 4400 00-4444 99 3355 0-3 74 7 4 3300 00-3322 44 2255 002277 44 2200 00-222 1155 244 00-1177 44 1100 0-1 2244 5500 --77 44 Number of examinations 73.5% 500 400 500 #exams 23.1% Sensitivity number Radiation Dose for CR • Variable Speed Detector • Optimal dose for typical adult chest image is 2X higher than 400 speed screen/film – Lower absorption efficiency – Quantum and electronic noise – Readout inefficiencies of latent image • AntiAnti-scatter grids necessary for most procedures Wrong exam 5% High Repeated Examinations with CR Motion 6% Positioning 46% Reprinting 9% Underexposure 10% Overexposure 12% Total # repeats = 1043 from Willis, RSNA 1996 AEC adjustment procedures • A 200200-speed equivalent exposure is desirable • Empirically determine AEC setting(s) with simple uniform phantoms • UCDMC technique: use “fixed” mode (S=200) and sensitivity test menu; adjust AEC response according to changes in film optical density • Verify settings with semisemi-auto mode • Verify patient exposure “S” number; recheck often Computed Radiography: Acceptance Testing and Quality Control -- J.A. Seibert, Ph.D. 10 Date: 7/10/98 Date: 7/10/98 Medical Medical Physicist: Physicist: Anthony Anthony Seibert, Seibert, Ph.D. Ph.D. Location: Location: System System Identification: Identification: UCDMC, UCDMC, ACC, ACC, 33 CR CR unit unit 33 Problem areas UC Davis Medical Center CR CR Reader Reader and and Screens Screens Inspection Results Summary • FilmFilm-based performance measurements Acceptab Acceptable le 1. 1. Physical Physical Inspection Inspection -- Inventory Inventory 2. 2. Imaging Imaging Plate Plate Uniformity Uniformity and and Dark Dark Noise Noise 3. 3. Signal Signal Response: Response: Linearity Linearity and and Slope Slope 4. 4. Signal Signal Response: Response: Calibration Calibration and and Beam Beam Quality Quality 5. 5. Laser Laser Beam Beam Function Function 6. 6. High-Contrast High-Contrast Resolution Resolution 7. 7. Noise/Low-Contrast Noise/Low-Contrast Response Response 8. 8. Distortion Distortion 9. 9. Erasure Erasure Thoroughness Thoroughness 10. 10. Anti-Aliasing Anti-Aliasing 11. 11. Positioning Positioning and and Collimation Collimation Errors Errors 12. 12. Throughput Throughput Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes* Yes* Yes Yes Yes Yes Yes Yes • Digital image analysis tools and evaluation methods not readily available • Low contrast resolution measurements • Lack of a standardized QC phantom Comments: Comments: Quality Control Three levels of system performance quality control 1. Routine: Technologist level - no radiation measurements 2. Full inspection: Physicist level Periodic Quality Control • Daily (technologist) – Inspect CR system and status. – Interfaces: PACS broker, ID terminal, QC workstation - radiation measurements and nonnon-invasive adjustments 3. System adjustment: Vendor service level – Erase image receptors (if status unknown). - hardware and software maintenance Periodic Quality Control • Weekly / Biweekly (technologist) – Calibrate review workstation monitors (SMPTE). – Acquire QC phantom test images. Verify performance. – Check filters / vents and clean as necessary. Periodic Quality Control • Quarterly (Technologist) – Inspect cassettes. Clean with recommended agents. – Review image retake rate and exposure trends. – Update QC log. Review outout-ofof-tolerance issues. – Clean screens with recommended agents. Computed Radiography: Acceptance Testing and Quality Control -- J.A. Seibert, Ph.D. 11 Periodic Quality Control • Annually (Physicist) What is needed? • Computer friendly phantoms – Perform linearity / sensitivity / uniformity tests – Inspect / evaluate image quality • Objective quantitative analysis methods • System performance tracking and database logs – ReRe-establish baseline values (Acceptance Tests) • Exposure monitoring tools and database tracking – Review retakes, exposures, service records. Fuji Agfa Line pair phantoms (contrast transfer tests) Lumisys Home built Diagonal bar (laser jitter test) 40 line/cm grid (visual aliasing) Fiducial Markers (distance accuracy) Lead attenuator (dynamic range) Resolution Bar Pattern (qualitative) Notches (geometric accuracy tests) Step wedge (signal, signal to noise and linearity response tests) Open area (scan uniformity test) Copper step wedge (dynamic range, linearity, SNR) Edge for Presampled MTF Single exposure, qualitative and quantitative Additional Information / Help • AAPM Task Group #10 document: • Email: jaseibert@ jaseibert@ucdavis. ucdavis.edu • Dr. Ehsan Samei spreadsheets – http://deckard .mc.duke.edu edu/~ /~samei samei/downloads /downloads http://deckard.mc.duke. • Vendor efforts for QC phantom development and analysis Summary • CR is the mainstay for direct digital acquisition of projection radiographs • CR acceptance testing and QC are essential for optimal operation • A TEAM approach is necessary – Technologists, Radiologists, Physicists, – Clinical Engineering, Information System Group Computed Radiography: Acceptance Testing and Quality Control -- J.A. Seibert, Ph.D. 12