Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
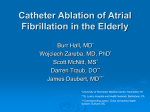
Chronic Atrial Fibrillation Is a Biatrial Arrhythmia Data from Catheter Ablation of Chronic Atrial Fibrillation Aiming Arrhythmia Termination Using a Sequential Ablation Approach Thomas Rostock, MD; Daniel Steven, MD; Boris Hoffmann, MD; Helge Servatius, MD; Imke Drewitz, MD; Karsten Sydow, MD; Kai Müllerleile, MD; Rodolfo Ventura, MD; Karl Wegscheider, PhD; Thomas Meinertz, MD; Stephan Willems, MD Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 Background—Termination of chronic atrial fibrillation (CAF) can be achieved by catheter ablation using a stepwise approach. However, there are limited data on the contribution of the right atrium to the CAF process. Furthermore, the prognostic value of CAF termination remains unclear. Methods and Results—Eighty-eight patients (61⫾10 years of age) underwent de novo ablation of CAF in 2006 at our institution. The ablation procedure was performed sequentially in the following order: pulmonary vein isolation, defragmentation of the left atrium, coronary sinus, and right atrium. Attempted procedural end point was termination of CAF. Consecutive arrhythmias occurring after AF termination were mapped, and ablation was attempted. AF termination was achieved in 68 (77%) patients: in 37 (55%) patients it occurred in the left atrium, in 18 (26%) patients in the right atrium, and in 13 (19%) patients in the coronary sinus. In 54 patients, at least one redo was performed (total number of procedures: 154). After the first redo, another 30 patients were in sinus rhythm (total 63), 8 patients were in atrial tachycardia (AT), and 17 patients were in AF. Another 11 patients underwent a second redo. After a mean follow-up of 20⫾4 months, 71 (81%) patients were in sinus rhythm, 1 (1%) patient was in AT, and 16 (18%) patients were in AF. Patients with CAF termination had predominantly ATs as recurrent arrhythmias (83%), whereas those without mainly presented with recurrent CAF (85%). The overall success rate in patients with CAF termination was 95% compared with 5% of patients without CAF termination in 2 procedures (n⫽12). In almost all redo procedures attributable to AT, at least 1 AT during redo was documented previously. Conclusions—AF termination is a prognostic important end point of catheter ablation for CAF. Termination of AF was achieved in both atria and the coronary sinus, suggesting a biatrial substrate of CAF. Subsequent arrhythmias often recur during follow-up and, therefore, should be targeted for ablation. (Circ Arrhythmia Electrophysiol. 2008;1:344-353.) Key Words: ablation 䡲 catheter ablation 䡲 atrial fibrillation 䡲 atrial tachycardia 䡲 mechanisms P aroxysmal atrial fibrillation (AF) is predominantly caused by electric discharges arising from the pulmonary veins (PVs).1 It is therefore the current consensus that catheter ablation procedures for paroxysmal AF targeting the PVs should aim for complete electric isolation,2 which is associated with success rates of about 80%.3 In contrast, the mechanisms of chronic AF (CAF) are less comprehensively elaborated. Even though the PVs remain a central target of the majority of catheter ablation approaches for CAF,4 –7 PV isolation alone may not be sufficient for a favorable outcome.8 Thus, a variety of lesion sets have been evaluated to enhance the clinical success rates of catheter ablation procedures for CAF.6,8 –12 However, the procedural end points did not predict the clinical outcome, and the majority of patients had to be cardioverted at the end of the procedure. The first study reporting on a predictive procedural end point was described by Haissaguerre et al.4,5 The aim of this stepwise ablation approach was to terminate chronic AF by ablation to either sinus rhythm (SR) or atrial tachycardia (AT), which was Editorial see p 324 Clinical Perspective see p 353 associated with a so-far unreported high success rate of 95% of patients being in SR after 1 year. Nevertheless, there are only limited data on clinical and electrophysiological follow-up of ⬎1 year. Thus, the aim of the present study was to evaluate acute success rates of termination of CAF using a sequential ablation approach, with special regard to the distribution of critical structures for termination in both the Received February 11, 2008; accepted September 15, 2008. From the Departments of Cardiology (T.R., D.S., B.H., H.S., I.D., K.S., K.M., R.V., T.M., S.W.), and Medical Biometry and Epidemiology (K.W.), University Hospital Eppendorf, Hamburg, Germany. Correspondence to Thomas Rostock, MD, Department of Cardiology, University Hospital Eppendorf, Martinistr. 52, D-20246 Hamburg, Germany. E-mail [email protected] © 2008 American Heart Association, Inc. Circ Arrhythmia Electrophysiol is available at http://circep.ahajournals.org 344 DOI: 10.1161/CIRCEP.108.772392 Rostock et al Biatrial Substrate of CAF 345 left and right atrium (RA) and to assess the prognostic value of CAF termination for the long-term follow-up. Methods Study Population Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 This study comprised 88 consecutive patients (mean age, 61⫾10 years; 11 women) with CAF who underwent an index procedure between January and December 2006. All patients were in AF for at least 3 months before the index procedure and presented with an AF cycle length (AFCL) ⱕ155 ms. The median duration of chronic AF before the procedure was 12 months (range, 3 to 264 months). Twenty-four (27%) patients had a history of at least 1 unsuccessful attempt at electric cardioversion. The mean left atrial (LA) diameter was 50⫾7 mm, and the mean left ventricular ejection fraction was 57⫾13%. Structural heart disease was present in almost two thirds (n⫽56; 64%) of the patients, consisting of hypertensive heart disease in 37 (42%) patients, which was associated with a coronary artery disease in 18 (20%) patients, valvular heart disease in 8 (9%) patients, of whom 4 patients had previously undergone surgical valve replacement (1 aortic valve, 3 mitral valve) without intraoperative ablation, and 11 (13%) patients with impaired left ventricular function (dilative cardiomyopathy in 6) and a left ventricular ejection fraction ⱕ50%. A total of 36 (41%) patients were on amiodarone. Twenty-one (24%) patients were treated with -blocker, and no patient was on any class-I-antiarrhythmic drug or on sotalol. All patients gave written informed consent. Antiarrhythmic drugs, with the exception of amiodarone, were ceased at least 5 half-lives before the procedure. PV isolation was the first step in all procedures and was performed as described previously.8 In brief, the posterior wall of the ipsilateral veins was initially targeted and an ablation line was deployed in a distance of 1 to 1.5 cm proximal from the PV ostium, which has been labeled by the Lasso catheter. Ablation started at the superior aspect of the LA posterior wall, and the line was continued around the entire vein including the anterior aspect as required to achieve complete electric disconnection. The PVs were isolated individually or as ipsilateral pairs. PV isolation was defined by elimination or dissociation of all PV potentials recorded by the Lasso catheter. Electrophysiological Study LA Defragmentation All patients underwent transesophageal echocardiography within 48 hours before the procedure to exclude atrial thrombi. The procedure was performed under sedation with propofol and under continuous monitoring of blood pressure and saturation. Surface electrocardiograms and bipolar endocardial electrograms were continuously monitored and stored on a computer-based digital amplifier/recorder system (Bard Electrophysiology). The following catheters were introduced via a femoral vein access: (1) a steerable decapolar catheter (Inquiry, IBI, Irvine Biomedical Inc) was positioned within the coronary sinus (CS); (2) a decapolar diagnostic catheter for circumferential mapping of the PVs (Lasso, Biosense-Webster); (3) a nonsteerable quadripolar diagnostic catheter (Inquiry, IBI, Irvine Biomedical Inc) was placed in the right atrial appendage; and (4) a 3.5-mm externally irrigated-tip ablation catheter (Biosense-Webster) was used for mapping and ablation. The Lasso and ablation catheter were stabilized with long sheaths (SL0, Daig, Inc, St. Jude Medical) continuously flushed with heparinized saline solution. Access to LA was achieved by a single transseptal puncture with the 2 catheters placed into the left atrium via the same puncture. A single bolus of 50 IU/kg body weight heparin was administered after transseptal puncture. As the second step, characteristic electrograms and electrogram behaviors considered to be involved in the electrophysiological processes of chronic AF were targeted in the LA. These targets were characterized as follows4,12: Radiofrequency Ablation The ablation procedure was performed using a sequential ablation approach by means of a modified stepwise ablation as described by Haissaguerre et al.4,5,12 The following steps were carried out in a fixed order unless the patient converted from AF to either SR or AT before finalizing all ablation steps (Figure 1). RF current was applied with a maximum power output of 30 W using an irrigation rate of 10 to 30 mL/min (0.9% saline infused with the Cool Flow Pump, Biosense Webster) for the PVs, 35 W and an irrigation rate between 30 and 60 mL/min in the LA, and up to 30 W in the RA. Ablation within the CS was performed with a maximum of 25 W, and the irrigation rate was manually adjusted to keep the tip-temperature below 42°C. In case of high impedances, the power setting was reduced to 20 W. Figure 1. Study protocol and subsequent ablation steps. PV Isolation ● ● ● ● ● Continuous electric activity without an interspersing isoelectric line High-frequency complex fractionated activity (multiple, highfrequency deflections of a single electrogram) Locally short AFCL or intermittent local burst activity Activation gradient between the electrogram recorded by the distal bipole in relation to the proximal bipole of the ablation catheter Local spreading of centrifugal activation Before ablation for LA defragmentation, the individual AF behavior in terms of AFCL and fractionation had been roughly evaluated at the LA appendage (LAA), the LA posterior wall, the lateral LA, and the LA septum to get an expeditious overview of the patient’s specific AF process. Defragmentation was defined as the conversion of complex, fractionated, or continuous electrograms into more discrete, regular, and synchronous activation.4,12 All regions of the LA were considered to harbor potential substrates critical for AF perpetuation. Because the AFCL after PV isolation often remains short,12 mapping of specific targets as described above is rather challenging because of contingently occurring passively activated fractionation potentially caused by a short local AFCL.13 Hence, the first step of LA defragmentation was uniquely performed by completely looping the ablation catheter within the LA such that the distal tip was placed at the LA roof by the site of the superior aspect of the previously applied RF lesions for left PV disconnection. Then, the catheter was dragged back toward the right superior PV while the local roof electrograms were mapped and ablated accordingly. Mapping and ablation was then continued at the LA septum by continuously dragging back the catheter. After elimination of fractionation or slowing of local AFCL at the LA septum, the endocardial aspect of the CS at the inferior LA was mapped. Ablation of the inferior LA was started medially at the septum with the ablation catheter facing the CS ostium endocardially and continued toward 346 Circ Arrhythmia Electrophysiol December 2008 the lateral endocardial aspect vis-à-vis the distal CS. Using this single maneuver, a relatively large area potentially involved in the individual chronic AF processes (roof, LA septum, inferior, and lateral LA, respectively) can be mapped and ablated. When the AFCL was prolonged, sites with specific electrogram characteristics, as described earlier, were targeted in virtually all areas of the LA. Defragmentation of the LA was finished when the described electrogram characteristics were no longer found at any LA site or when the AFCL in the LA was longer than the one in the CS or the RA. Table. Procedure-Related Data Index Procedure No. Redo Procedure P 88 66 293 (120–440) 210 (60–360) ⬍0.001 Fluoroscopy time, min 75 (22–138) 47 (7–95) ⬍0.001 No. of RF applications 62 (22–122) 29 (4–78) ⬍0.001 Procedure duration, min Defragmentation/Electric Isolation of the CS When AF did not terminate during LA ablation, defragmentation was performed within the CS. The ablation was started in the distal CS and the ablation catheter was continuously withdrawn toward the CS ostium. End points of CS ablation were elimination of complex fractionation, slowing of the local AFCL, or electric isolation. Electric isolation was defined as either complete disappearance of all atrial signals in the CS or occurrence of a dissociated activity. When the AF activity in the CS itself was converted into discrete synchronous electrograms with a significant prolongation of the AFCL, no further attempt was made to isolate the CS completely. Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 Right Atrial Defragmentation Right atrial ablation was performed as the final step in all patients without prior AF termination during LA or CS ablation. Targets and end points of RA ablation were similar to those described for defragmentation of the LA. The superior vena cava (SVC) was mapped in all cases. A SVC driver was defined as a specific sequence with the earliest activation within the SVC (activation of the RA from the SVC) or as the presence of a shorter AFCL in the SVC when compared with the RA. Procedural End Points The attempted procedural end point was termination of AF and, whenever possible, termination of subsequent ATs with the achievement of SR by ablation only. When AF termination had not been achieved, the procedure was stopped after a maximum of 6 hours or if a maximum of 5 L of fluid had been administered to the patient via the catheter irrigation. The patient was then externally cardioverted. If AF was terminated by ablation and converted to AT, conventional techniques were used to identify the underlying mechanism and subsequent ablation was commenced. Conversion from AF to AT was defined as the occurrence of an organized atrial rhythm with a consistent atrial activation sequence (assessed by the CS, HRA, and mapping catheter) and by a monomorphic P-wave morphology. Follow-Up All patients were regularly seen every 3 months in our outpatient clinic. Before these visits, the patients received at least 2 Holter ECGs. Furthermore, detailed evaluation of the patients’ symptoms suggestive for potential AF recurrences was performed. In case of arrhythmia recurrences within the initial 3 months after the index procedure, irrespective of the arrhythmia mechanism (AF or AT), the patients were cardioverted. All recurrent arrhythmias occurring during the follow-up were documented by a 12-lead ECG and compared with the arrhythmias mapped and ablated during the procedures. An interval of at least 3 months was required between 2 procedures. Antiarrhythmic drug treatment, including amiodarone, was discontinued after the index procedure in all patients. Patients with recurrence of CAF within the initial 3 months after the index procedure were cardioverted and treated with amiodarone. These patients were scheduled for a redo procedure 3 months after the index procedure and amiodarone was discontinued afterward. Patients with recurrences after the initial 3 months underwent primary reablation. Statistical Analysis Continuous data are given as median and range or mean⫾SD. Comparison between groups (ie, AF termination versus no AF termination, index versus redo procedure) was carried out using either the Student t test or the Wilcoxon rank-sum test when appropriate. A 2-tailed probability value of ⬍0.05 was considered to be statistically significant. The 95% confidence intervals are given for the success rates after each procedure and for the total result. The authors had full access to and take full responsibility for the integrity of the data. All authors have read and agree to the manuscript as written. Results Procedural Data A total of 154 ablation procedures were performed in the 88 study patients. Of these, 33 patients underwent a single ablation procedure, whereas 54 patients had at least one redo procedure (median number of procedures per patient with at least one redo 2 [range, 2 to 4]). The procedure-related data of index and redo procedures are shown in the Table. Thus, the mean procedure duration and fluoroscopy time were significantly shorter and less RF applications were necessary for the redo compared with the index procedures. Termination of AF during Ablation During the index procedure, termination of AF was achieved in 68 (77%) patients (Figure 2). Of these, termination occurred in 37 (54%) patients in the LA (Figure 3, top), in the CS in 13 (20%) patients (Figure 3, bottom), and in the RA in 18 (26%) patients. The baseline AFCL of the LAA and RAA did not differ significantly between patients with AF termination in the LA and RA. However, in patients with AF termination in the RA after PV isolation, the AFCL of the RAA was significantly shorter than the one in the LAA (148 ms [143 to 158 ms] versus 162 ms [153 to 164 ms]; P⫽0.01). No significant AFCL gradient between LAA and RAA was observed after PV isolation in patients with AF termination in the LA or CS (159 ms [152 to 166 ms] versus 156 ms [148 to 162 ms]; P⫽0.20). Direct conversion to SR was observed in 8 patients (5 during PV isolation, 1 RA septum, 1 RA lateral, and 1 LA lateral), whereas in 60 patients, AF was converted to AT. During the index procedure, AF was not terminated in 20 (23%) patients. Of these, the procedure was stopped prematurely in 13 patients because of a fluid administration ⱖ5 L via the externally irrigated tip ablation catheter (after a mean procedure duration of 298⫾29 minutes), and in 7 patients after reaching a procedure duration of ⱖ6 hours. These end points exclusively occurred during the final step of RA ablation. Patients with a CAF duration ⬍6 months had significantly shorter procedure durations (248 minutes [120 to 420 minutes] versus 338 minutes [190 to 440 minutes]; P⬍0.001), and required a lower number of RF applications (52 [22 to Rostock et al Biatrial Substrate of CAF 347 Figure 2. Distribution of termination sites of chronic AF. An outer ring labels sites of termination at the posterior LA. (LA: LAA⫽10, PVs⫽8, inferior⫽6, septum⫽5, roof⫽3, lateral⫽2, posterior⫽2, anterior⫽1; CS: ostium⫽6, proximal⫽5, distal⫽2; RA: anterior⫽10, septum⫽6, lateral⫽2). Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 111] versus 69 [36 to 122]; P⫽0.001) when compared with patients with CAF lasting ⬎6 months before the procedure. Twenty-three of 54 patients presented with recurrence of CAF after the first procedure (1 patient refused redo). Of these 22 patients, AF was terminated in 7 (32%) patients. AF termination occurred in 4 patients in the LA, in 1 patient in the CS, and 2 patients in the RA. In 12 (55%) patients, no AF termination was achieved in 2 ablation procedures. Further- Figure 3. Top, Termination of AF directly to SR. The ablation catheter is positioned at the LA roof, which displays a rapid and high-fractionated electric activity (A). RF delivery at that site initially organized fractionation to discrete potentials (B) and finally terminated AF to SR (C). Of note, complete roof-line block occurred during ablation indicated by the occurrence of clearly separated double potentials during SR (arrows), suggesting a close relation of the interatrial connection (Bachmann’s bundle) to the roof-line. Bottom, Focal AF within the proximal CS (Map), which was conducted to the atria in a relative regular fashion mimicking atrial tachycardia (HRA), whereas the distal CS was isolated indicated by a dissociated rhythm (CS 3/4). Ablation at that site resulted in AF termination and conversion to atrial tachycardia. 348 Circ Arrhythmia Electrophysiol December 2008 Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 Figure 4. A, Flowchart of the patient flow with regard to arrhythmia termination during each procedure and outcome in terms of an arrhythmia-free follow-up (SR) or arrhythmia recurrences (No SR). The arrows indicate how many patients are in SR after each procedure (left panel), how many patients have undergone a redo procedure, and how many patients finished the study without the achievement of SR. B, The histogram demonstrates the arrhythmia outcomes after each procedure with regard to SR, AF, and AT, respectively, and with 95% confidence intervals shown in brackets. more, in 3 patients with AF termination during the index procedure and AF recurrences, AF was not terminated during the redo procedure (Figure 4). Characterization of Subsequent Arrhythmias During the index procedure, subsequent ATs occurred after AF termination in 60 patients (Figure 5). A total number of 98 different ATs were found in those 60 patients, with a median number of 1 [1 to 4] AT per patient. These ATs were characterized as focal in 31 and reentry in 67 cases. Focal ATs were observed at the LA septum (n⫽9), LA anterior wall (n⫽4), RA anterior wall (n⫽4), proximal CS (n⫽4), RA lateral wall (n⫽3), LA inferior (n⫽3), RA septum (n⫽2), and LAA (n⫽2). Macroreentrant ATs consisted of perimitral flutter (n⫽24), LA roof-dependent flutter (n⫽17), cavotricuspid isthmus flutter (n⫽12), and CS ostium reentry (n⫽10). Of note, microreentrant circuits were demonstrated at the LAA ridge in 3 patients and at the LA septum in 1 patient. These microreentrant ATs were characterized by consistent entrainment with the shortest postpacing interval (ⱕ⫹20 ms of AT cycle length) at the site where ⱖ80% of the AT cycle length was displayed by the 2 bipoles of the ablation catheter (Figure 6). These ATs were eliminated by focal ablation in all cases. A total of 28 (32%) patients required linear ablation (mitral isthmus: n⫽10, roof line: n⫽9, both lines: n⫽17) either for AF termination or ablation of subsequent macroreentrant tachycardias during the index procedure. Mitral isthmus block was achieved in 21 patients (78%) and roof line block in 23 patients (88%). Only 4 of 18 patients (22%) with AF termination required linear ablation. Termination of AT with conversion to SR was not achieved in 22 patients because of exceeding procedure durations of 6 hours (n⫽13), fluid administration of ⱖ5 L (n⫽8), and occurrence of tamponade (n⫽1). In 5 of these patients, AT was terminated to SR by overdrive pacing, whereas the remaining patients required external cardioversion. Rostock et al Biatrial Substrate of CAF 349 Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 Figure 5. Termination of AF and consecutive arrhythmias that occurred before obtaining SR. CTI – Flutter⫽common type atrial flutter. Follow-Up and Recurrent Arrhythmias The mean follow-up was 20⫾4 months. Among the 88 study patients, 33 (38%) patients were free of any recurrent arrhythmia after a single procedure, including 1 patient without AF termination during ablation. At least one redo procedure was performed in 54 patients at a mean of 8⫾4 months. The most favorable outcome was observed in patients with AF termination during the index procedure. Approximately one half of these had arrhythmia recurrences. However, only 6 patients presented with AF, whereas the majority (n⫽30) had ATs and no further episodes of AF. On the other hand, in 12 patients without AF termination during either index or redo procedure, AF recurred and persisted. These patients were not scheduled for a second redo procedure. After the first redo procedure, a total of 63 (72%) patients were arrhythmia-free during follow-up. Another 11 patients required a second redo procedure of whom 1 patient underwent a third redo procedure. Finally, a total of 71 (81%) patients were free of any recurrent arrhythmias, whereas 16 patients had recurrence of AF (2 with paroxysmal AF) and 1 patient had AT (Figure 4). Four patients with recurrences (2 AT, 2 PAF) were taking amiodarone during follow-up. All but 5 patients demonstrated electric reconduction of at least 1 PV (1.5⫾0.9 PVs per patient). During redo procedures, patients with AT presented with a mean of 1.9⫾0.9 tachycardias (75 reentry, 18 focal), consisting of perimitral flutter (n⫽27), LA roof-dependent flutter (n⫽19), cavotricuspid isthmus flutter (n⫽16), and CS ostium reentry (n⫽7). Microreentrant circuits were found at the LAA ridge in 3 patients and at the anterior wall in another 3 patients (Figure 5). Focal ATs were observed in the proximal CS (n⫽4), at the LA roof (n⫽4), at the LAA (n⫽3), RA septum (n⫽3), PV ostium (n⫽2), RA posterior (n⫽1), and LA inferior (n⫽1). Interestingly, in 30 patients, at least 1 AT observed during the redo procedure had been documented previously either during an earlier ablation procedure or during the initial 3 months of follow-up. Characteristics of Patients not Benefiting From Ablation A strong procedural predictor for recurrence of chronic AF was the failure to terminate AF by ablation during the 2 procedures. All 12 patients in whom AF was not terminated during the index and redo procedure demonstrated recurrence of CAF. Epidemiologically, these patients were characterized by larger LA diameter (54⫾5 mm versus 48⫾7 mm; P⫽0.005), an impaired left ventricular function (50⫾14% versus 58⫾12%; P⫽0.048), and a longer duration of CAF (44⫾49 months versus 17⫾21 months; P⫽0.001). Of note, patients without AF termination in 2 ablation procedures and with CAF recurrence had significantly shorter baseline AFCL than patients with AF termination (124⫾4 ms versus 146⫾4 ms; P⫽0.001; Figure 7). Furthermore, all but one of these patients had a structural heart disease (dilative cardiomyopathy in 4 patients, congestive heart failure in 2 patients, coronary artery disease in 3 patients, and hypertensive heart disease in 2 patients). Adverse Events During a total of 154 procedures, 2 patients developed pericardial tamponade (1 during left lateral defragmentation and 1 during ablation at the RA anterior wall), which were successfully managed by pericardiocentesis. In another patient, a transient ischemic attack occurred 1 day after the procedure that completely recovered. A transient dissociation between the RA and LA was observed in 1 patient (without any electric activity in the RA and an AT in the LA), which recovered within 1 hour after its occurrence. An electric isolation of the LAA with slow dissociated activity was observed in 1 patient. Because ablation was immediately interrupted, the LAA conduction recovered within 15 minutes. There were no phrenic nerve injuries. Discussion This study demonstrates that termination of CAF by ablation can be achieved in a substantial number of patients using a 350 Circ Arrhythmia Electrophysiol December 2008 Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 Figure 6. AT with a cycle length of 230 ms, which occurred after termination of AF during the index procedure. The ablation catheter is positioned at the anterior ridge of the LAA. Of note, the distal and proximal bipole of the ablation catheter (Map) cover almost the entire tachycardia cycle length. This tachycardia was characterized by consistent concealed entrainment with a postpacing interval of ⫹10 ms, indicating a microreentry at the anterior LAA ridge. Focal ablation with a single RF application at that spot led to AT termination and conversion to a different AT. sequential ablation approach. Our study provides evidence that AF termination is associated with a high-success rate during the long-term follow-up, revealing termination of AF as an important procedural end point. However, a considerable number of patients required ablation in the RA and the CS to achieve AF termination, indicating a biatrial substrate of CAF. Of note, CAF typically converts to clinically relevant ATs demonstrated by its reoccurrence during follow-up. This is particularly the case after unsuccessful ablation or when electric recovery of the critical substrate occurs. Finally, this study identified patient characteristics associated with low procedural and clinical success rates of ablation, ie, longstanding CAF, short AFCL, and structural heart diseases with concomitantly impaired cardiac function. Mechanistic Insights From Ablation (Termination) of Chronic AF Different approaches for catheter ablation of AF have been described mainly focusing on electrophysiological end points of the arrhythmia substrate (eg, PV isolation, voltage reduction) rather than on the arrhythmia itself. Only 2 studies used AF termination by ablation as the procedural end point.4,5,11 Haissaguerre et al4,5 were the first to describe an approach with ablation of the AF substrate validated by electrophysi- ological criteria, thereby progressively increasing the AFCL and finally aiming to terminate the arrhythmia. Although other studies, which had not sought to influence or terminate the arrhythmia by ablation, reported an incidental termination rate of ⬍30% by LA ablation,6,10,14,15 termination of CAF was achieved in 87% of patients using the stepwise ablation approach.4,5 Unlike in patients with paroxysmal AF, where the arrhythmia processes are predominantly confined to the PVs and its junction to the LA, the multiple mechanisms of CAF require an individually tailored approach.16 Nademanee et al11 first described the ablation of complex fractionated atrial electrograms (CFAE) with promising results in terms of AF termination and long-term outcome. However, this procedure merely targeted CFAE defined as fractionated electrograms composed of 2 or more deflections or continuous deflections of a prolonged activation complex with a cycle length ⱕ120 ms. In the study by Haissaguerre et al,4,5 4 different targets for AF substrate ablation were distinguished: (1) areas of continuous electric activity (closest to the definition of CFAE), (2) temporal activation gradient between proximal and distal ablation bipoles, (3) spatial centrifugal activation, and (4) areas of short cycle length activity. The suspected mechanisms behind these electrogram characteristics consist of Rostock et al Biatrial Substrate of CAF 351 Figure 7. Progression of the mean AFCL during ablation in comparison of patients with CAF termination in LA, CS, RA, and those without termination. The mean baseline AFCL was significantly shorter in patients without termination when compared with patients with AF termination. DC indicates external cardioversion. Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 slow conduction, eg, when a wavelet traverses through a critical isthmus (1), microreentrant sources (rotors) or sites of “pivot-pointing” around a cornerstone of a functional line of block (2), and focal electric activity (3 and 4). When starting a CAF ablation procedure, the initial AFCL used to be short, indicating a complex interaction of multiple and simultaneously operating AF processes. Thus, accurate identification of areas that contribute actively to CAF often remains challenging, particularly considering the cycle length dependency of CFAE.13 Therefore, it is a reasonable approach to start the procedure by targeting the sites with the greatest impact on AFCL prolongation, ie, the PVs, LAA, and inferior LA, and thereby facilitating a conceivable mapping of CAF.4,17 Swartz et al18 were the first to report on CAF termination by ablation. In their series, biatrial linear lesions were created in an attempt to replicate the Maze procedure, which resulted in a remarkable success rate of up to 90%. In the study by Nademanee et al,11 although achievement of AF termination occurred in a relatively high number of patients, no data were provided on the association between AF termination and clinical outcome. Thus, it has remained unclear whether there is a direct prognostic relation between AF termination by ablation or, in other words, whether failure to terminate CAF is associated with a worse long-term outcome. In their subsequent series of patients treated for CAF using the stepwise ablation approach, Haissaguerre and colleagues19 reported that patients with CAF termination rarely presented with AF recurrences during the follow-up, whereas the predominant recurrent arrhythmia in those patients was AT. In addition to these findings, our study demonstrates a direct relationship between failure to terminate CAF (in 2 procedures) and an unfavorable clinical outcome. Thus, the concept of AF termination by ablation emerges as a reasonable procedural end point with a high prognostic value for the clinical outcome. Biatrial Substrate of Chronic AF Historically, initial attempts of ablation procedures to treat AF have been performed in the RA. Nevertheless, right atrial linear ablation merely resulted in a modest reduction of AF recurrences.20,21 Because the PVs were recognized as a crucial substrate harboring AF sources,1 ablation procedures with the intention to cure AF predominantly concentrated on the LA and its adjacent great thoracic veins. This concept was further corroborated by the observation of an activation gradient from the left atrium to the RA,22 which is characteristically observed in patients with paroxysmal AF.23,24 However, this activation gradient was not demonstrated in patients with long-standing AF,19 indicating the involvement of both atria in the CAF process. Furthermore, data from biatrial multielectrode mapping derived from electrophysiological investigations and epicardial mapping performed at the time of cardiac surgery suggested the presence of AF sources in both atria.25,26 Although these data indicate a contribution of the RA to the CAF process, only a limited number of studies have investigated the impact of right atrial ablation on either the long-term outcome or termination rate of CAF. Nademanee16 reported in their subsequent series of patients treated by electrogram-guided ablation that 15% of the patients did require ablation in the RA. Similarly, the stepwise ablation approach necessitated RA ablation in 20% of patients to terminate CAF.21 Thus, previous data from observational studies underline the contribution of RA substrates in the pathophysiology of CAF. Furthermore, the demonstration of AF termination by catheter ablation clearly indicates the presence of localized right atrial arrhythmogenic sources driving AF. Those data are therefore strikingly in line with the results of our present study, revealing that AF termination occurred in one fourth of patients during ablation in the RA, and thus providing an accumulating body of evidence for the concept of “chronic AF is a biatrial arrhythmia.” Mechanisms and Clinical Relevance of Subsequent ATs Mechanisms of recurrent arrhythmias after PV isolation (both AF and AT) have been described to be predominantly related to the PVs themselves, comprising gap-related PV tachycardias and macroreentry around ipsilateral PVs.27–29 However, the clinical 352 Circ Arrhythmia Electrophysiol December 2008 Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 significance of subsequent arrhythmias documented after termination of AF at the index procedure or during follow-up has remained unclear. The occurrence of ATs after extensive AF ablation has generally been recognized as a procedure-related proarrhythmogenic side effect. Those ATs can be localized at virtually all sites of the atria and their adjacent thoracic veins and consist of macroreentry, microreentry, and focal tachycardia, whereas the discrimination of the latter 2 is often challenging.30 Jais et al31 described ATs with a small circuit localized to the anterior LA in patients who had undergone previous AF ablation but without prior ablation at the anterior LA. Thus, a potential mechanism of these ATs— other than being proarrhythmic because of RF-induced slow conduction or incomplete/recovered lesions—might be an “organization” of the arrhythmia from AF to AT by diminishing the capability to fibrillatory conduction of the substrate and thereby facilitating AF driving circuits to become apparent. Using the stepwise ablation approach, it has been described that patients with AF termination and conversion to AT commonly present with ATs as recurrent arrhythmias, which demonstrated a similar distribution to those contributing initially to the maintenance of AF.5 This finding is supported by the results of the present study. The majority of ATs ablated during redo procedures were previously observed during an earlier procedure, particularly when those ATs were not targeted for ablation (because of a long-procedure duration), were unsuccessfully ablated or when recovery of the critical substrate occurred, indicating their clinical significance and the need of ablation treatment, subsequently. Study Limitations In the present study, no quantitative analysis of complex fractionation has been performed. Thus, no information can be provided with regard to the impact of each ablation step on the distribution on electrogram fractionation. All procedures were performed without using a 3-dimensional mapping system. Therefore, we did not assess the scar burden during redo procedures. However, considering a similar ablation approach used in the present study compared with that described by Haissaguerre et al,4,5 a comparable scar burden as described by Takahashi et al32 can be assumed. In 13 patients, the procedure was stopped prematurely because of an extensive fluid administration. The use of a 3-dimensional mapping system in conjunction with an (nonirrigated) 8-mm catheter tip might have prevented reaching this end point. Because the baseline AFCL was ⱕ155 ms in all patients, a relatively large portion of the LA displayed CFAE. Therefore, it cannot be excluded that areas with CFAE caused by a short AFCL (and thereby, passively activated and not actively involved in the AF process13) have been ablated. Pretreatment with amiodarone before ablation may prolong the baseline AFCL and consequently reduce the amount of passive fractionation. An extensive ablation procedure as described in this study may have the potential to create conditions critical for the development of (new) ATs, particularly macroreentrant and microreentrant tachycardias and, thereby, might be in part proarrhythmogenic. The follow-up consisted of symptom-based and conventional 24-hour or 48-hour Holter monitoring for the assessment of AF recurrences. Although the majority of patients were in persistent AF when presenting with AF as their recurrent arrhythmia, asymptomatic recurrences might be missed during follow-up. Conclusions Termination of AF by ablation is an important prognostic end point of catheter ablation for CAF. AF termination can be achieved using a sequential ablation approach in both atria and the CS, indicating a biatrial substrate of CAF. Subsequent arrhythmias do often occur and successive ablation of those arrhythmias is mandatory to achieve an arrhythmia-free follow-up. Epidemiological and electrophysiological parameters, ie, exceedingly long-standing chronic AF, short AFCL, and concomitant structural heart diseases with impaired cardiac function, may help to identify patients with a potentially unfavorable outcome of CAF ablation. Disclosures None. References 1. Haissaguerre M, Jais P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Metayer P, Clementy J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339:659 – 666. 2. Calkins H, Brugada J, Packer DL, Cappato R, Chan SA, Crijns HJ, Damiano RJ Jr, Davies DW, Haines DE, Haissaguerre M, Iesaka Y, Jackman W, Jais P, Kottkamp H, Kuck KH, Lindsay BD, Marchlinski FE, McCarthy PM, Mont JL, Morady F, Nademanee K, Natale A, Pappone C, Prystowsky E, Raviele A, Ruskin JN, Shemin RJ. Heart Rhythm Society; European Heart Rhythm Association; European Cardiac Arrhythmia Society; American College of Cardiology; American Heart Association; Society of Thoracic Surgeons. HRS/EHRA/ECAS expert consensus statement on catheter ablation and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up. Europace. 2007;9:335–379. 3. Steven D, Rostock T, Lutomsky B, Klemm H, Servatius H, Drewitz I, Friedrichs K, Ventura R, Meinertz T, Willems S. What is the real AF burden after catheter ablation of atrial fibrillation? A prospective rhythm analysis in pacemaker patients with continuous atrial monitoring. Eur Heart J. 2008;29:1037–1042. 4. Haissaguerre M, Sanders P, Hocini M, Takahashi Y, Rotter M, Sacher F, Rostock T, Hsu LF, Bordachar P, Reuter S, Roudaut R, Clementy J, Jais P. Catheter ablation of long-lasting persistent atrial fibrillation: critical structures for termination. J Cardiovasc Electrophysiol. 2005;16:1125–1137. 5. Haissaguerre M, Hocini M, Sanders P, Sacher F, Rotter M, Takahashi Y, Rostock T, Hsu LF, Bordachar P, Reuter S, Roudaut R, Clementy J, Jais P. Catheter ablation of long-lasting persistent atrial fibrillation: clinical outcome and mechanisms of subsequent arrhythmias. J Cardiovasc Electrophysiol. 2005;16:1138 –1147. 6. Oral H, Pappone C, Chugh A, Good E, Bogun F, Pelosi F Jr, Bates ER, Lehmann MH, Vicedomini G, Augello G, Sala S, Santinelli V, Morady F. Circumferential pulmonary-vein ablation for chronic atrial fibrillation. N Engl J Med. 2006;354:934 –941. 7. Sanders P, Hocini M, Jais P, Sacher F, Hsu LF, Takahashi Y, Rotter M, Rostock T, Nalliah CJ, Clementy J, Haissaguerre M. Complete isolation of the pulmonary veins and posterior left atrium in chronic atrial fibrillation. Long-term clinical outcome. Eur Heart J. 2007;28:1862–1871. 8. Willems S, Klemm H, Rostock T, Brandstrup B, Ventura R, Steven D, Risius T, Lutomsky B, Meinertz T. Substrate modification combined with pulmonary vein isolation improves outcome of catheter ablation in patients with persistent atrial fibrillation: a prospective randomized comparison. Eur Heart J. 2006;27:2871–2878. 9. Hsu LF, Jais P, Sanders P, Garrigue S, Hocini M, Sacher F, Takahashi Y, Rotter M, Pasquie JL, Scavee C, Bordachar P, Clementy J, Haissaguerre M. Catheter ablation for atrial fibrillation in congestive heart failure. N Engl J Med. 2004;351:2373–2383. 10. Ouyang F, Ernst S, Chun J, Bänsch D, Li Y, Schaumann A, Mavrakis H, Liu X, Deger FT, Schmidt B, Xue Y, Cao J, Hennig D, Huang H, Kuck Rostock et al 11. 12. 13. 14. 15. Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 16. 17. 18. 19. 20. 21. KH, Antz M. Electrophysiological findings during ablation of persistent atrial fibrillation with the electroanatomic mapping and double Lasso catheter technique. Circulation. 2005;112:3038 –3048. Nademanee K, McKenzie J, Kosar E, Schwab M, Sunsaneewitayakul B, Vasavakul T, Khunnawat C, Ngarmukos T. A new approach for catheter ablation of atrial fibrillation: mapping of the electrophysiologic substrate. J Am Coll Cardiol. 2004;43:2044 –2053. O’Neill MD, Jais P, Takahashi Y, Jönssen A, Sacher F, Hocini M, Sanders P, Rostock T, Rotter M, Pernat A, Clementy J, Haissaguerre M. The stepwise ablation approach for chronic atrial fibrillation—evidence for a cumulative effect. J Interv Cardiac Electrophysiol. 2006;16:153–167. Rostock T, Rotter M, Sanders P, Takahashi Y, Jais P, Hocini M, Hsu LF, Sacher F, Clementy J, Haissaguerre M. High-density activation mapping of fractionated electrograms in the atria of patients with paroxysmal atrial fibrillation. Heart Rhythm. 2006;3:27–34. Oral H, Chugh A, Good E, Igic P, Elmouchi D, Tschopp DR, Reich SS, Bogun F, Pelosi F Jr, Morady F. Randomized comparison of encircling and nonencircling left atrial ablation for chronic atrial fibrillation. Heart Rhythm. 2005;2:1165–1172. Calo L, Lamberti F, Loricchio ML, De Ruvo E, Colivicchi F, Bianconi L, Pandozi C, Santini M. Left atrial ablation versus biatrial ablation for persistent and permanent atrial fibrillation: a prospective and randomized study. J Am Coll Cardiol. 2006;47:2504 –2512. Nademanee K. Trials and travails of electrogram-guided ablation of chronic atrial fibrillation. Circulation. 2007;115:2592–2594. Haissaguerre M, Hocini M, Sanders P, Takahashi Y, Rotter M, Sacher F, Rostock T, Hsu LF, Jonsson A, O’Neill MD, Bordachar P, Reuter S, Roudaut R, Clementy J, Jais P. Localized sources maintaining atrial fibrillation organized by prior ablation. Circulation. 2006;113:616–625. Swartz JF, Pellersels G, Silvers L, Patten L, Cervantez D. A catheter-based curative approach to atrial fibrillation in humans. Circulation. 1994;90: I-335. Matsuo S, Lim KT, Haissaguerre M. Ablation of chronic atrial fibrillation. Heart Rhythm. 2007;4:1461–1463. Haissaguerre M, Jais P, Shah DC, Gencel L, Pradeau V, Garrigues S, Chouairi S, Hocini M, Le Metayer P, Roudaut R, Clementy J. Right and left atrial radiofrequency catheter therapy of paroxysmal atrial fibrillation. J Cardiovasc Electrophysiol. 1996;7:1132–1144. Garg A, Finneran W, Mollerus M, Birgersdotter-Green U, Fujimura O, Tone L, Feld GK. Right atrial compartmentalization using radiofrequency 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. Biatrial Substrate of CAF 353 catheter ablation for management of patients with refractory atrial fibrillation. J Cardiovasc Electropysiol. 1999;10:763–771. Mansour M, Mandapati R, Berenfeld O, Chen J, Samie FH, Jalife J. Left-to-right gradient of atrial frequencies during acute atrial fibrillation in the isolated sheep heart. Circulation. 2001;103:2631–2636. Lazar S, Dixit S, Marchlinski FE, Callans DJ, Gerstenfeld EP. Presence of left-to-right atrial frequency gradient in paroxysmal but not persistent atrial fibrillation in humans. Circulation. 2004;110:3181–3186. Lazar S, Dixit S, Callans DJ, Lin D, Marchlinski FE, Gerstenfeld EP. Effect of pulmonary vein isolation on the left-to-right atrial dominant frequency gradient in human atrial fibrillation. Heart Rhythm. 2006;3:889–895. Saksena S, Skadsberg ND, Rao HB, Filipecki A. Biatrial and three-dimensional mapping of spontaneous atrial arrhythmias in patients with refractory atrial fibrillation. J Cardiovasc Electrophysiol. 2005;16:494–504. Nitta T, Ishii Y, Miyagi Y, Ohmori H, Sakamoto S, Tanaka S. Concurrent multiple left atrial focal activations with fibrillatory conduction and right atrial focal or reentrant activation as the mechanism in atrial fibrillation. J Thorac Cardiovasc Surg. 2003;126:254 –262. Cummings JE, Schweikert R, Saliba W, Hao S, Martin DO, Marrouche NF, Burkhardt JD, Kilicaslan F, Verma A, Beheiry S, Belden W, Natale A. Left atrial flutter following pulmonary vein antrum isolation with radiofrequency energy: linear lesions or repeat isolation. J Cardiovasc Electrophysiol. 2005;16:293–297. Gerstenfeld EP, Callans DJ, Dixit S, Russo AM, Nayak H, Lin D, Pulliam W, Siddique S, Marchlinski FE. Mechanisms of organized left atrial tachycardias occurring after pulmonary vein isolation. Circulation. 2004;110:1351–1357. Jais P, Hocini H, Hsu LF, Sanders P, Scavee C, Weerasooriya R, Macle L, Raybaud F, Garrigue S, Shah DC, Le Metayer P, Clementy J, Haissaguerre M. Technique and results of linear ablation at the linear mitral isthmus. Circulation. 2004;110:2996 –3002. Merino JL. Slow conduction and flutter following atrial fibrillation ablation: proarrhythmia or unmasking effect of radiofrequency application? J Cardiovasc Electrophysiol. 2006;17:516 –519. Jais P, Sanders P, Hsu LF, Hocini M, Sacher F, Takahashi Y, Rotter M, Rostock T, Bordachar P, Reuter S, Laborderie J, Clementy J, Haissaguerre M. Flutter localized to the anterior left atrium after catheter ablation of atrial fibrillation. J Cardiovasc Electrophysiol. 2006;17:279–285. Takahashi Y, O’Neill MD, Hocini M, Reant P, Jonsson A, Jais P, Sanders P, Rostock T, Rotter M, Sacher F, Laffite S, Roudaut R, Clementy J, Haissaguerre M. Effects of stepwise ablation of chronic atrial fibrillation on atrial electrical and mechanical properties. J Am Coll Cardiol. 2007;49:1306–1314. CLINICAL PERSPECTIVE Chronic atrial fibrillation (CAF) is a complex arrhythmia with the involvement of multiple atrial substrates, including the great thoracic veins. The contribution of the right atrium to the CAF process has remained unclear, thus far. Considering that termination of CAF by ablation is a result of the elimination of all arrhythmogenic substrates critical for arrhythmia perpetuation, atrial fibrillation (AF) termination occurring in the right atrium may be an indicator for participation of the right atrium in the fibrillatory process. In the present study, we performed a modified sequential ablation approach consisting of pulmonary vein isolation and defragmentation of the left atrium, coronary sinus, and the right atrium in a predefined order. CAF termination was achieved in 77% of patients. Interestingly, AF terminated in almost one half of the patients during ablation outside the left atrium (26% in the right atrium and 19% in the coronary sinus). Patients with AF termination predominantly presented with atrial tachycardia as the recurrent arrhythmia. After a follow-up of 20⫾4 months, 95% of patients with CAF termination were in sinus rhythm. However, almost all patients without CAF termination in two procedures had AF recurrence and remained in CAF. These data indicate that “CAF is a biatrial arrhythmia.” Furthermore, AF termination has emerged as an important prognostic end point of catheter ablation for CAF. Chronic Atrial Fibrillation Is a Biatrial Arrhythmia: Data from Catheter Ablation of Chronic Atrial Fibrillation Aiming Arrhythmia Termination Using a Sequential Ablation Approach Thomas Rostock, Daniel Steven, Boris Hoffmann, Helge Servatius, Imke Drewitz, Karsten Sydow, Kai Müllerleile, Rodolfo Ventura, Karl Wegscheider, Thomas Meinertz and Stephan Willems Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 Circ Arrhythm Electrophysiol. 2008;1:344-353; originally published online December 2, 2008; doi: 10.1161/CIRCEP.108.772392 Circulation: Arrhythmia and Electrophysiology is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2008 American Heart Association, Inc. All rights reserved. Print ISSN: 1941-3149. Online ISSN: 1941-3084 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circep.ahajournals.org/content/1/5/344 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Arrhythmia and Electrophysiology can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation: Arrhythmia and Electrophysiology is online at: http://circep.ahajournals.org//subscriptions/