Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
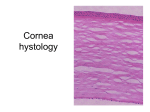
Melissa B Daluvoy MD, Neelofar Ghaznawi MD, Kristin M Hammersmith MD, Edwin S Chen MD, Christopher J Rapuano MD, Elisabeth J Cohen MD Cornea Service, Wills Eye Institute, Thomas Jefferson University Hospital, Philadelphia, Pennsylvania, USA The authors have no financial interest in the subject matter of this poster Epithelial basement membrane dystrophy (EBMD) is the most common anterior corneal dystrophy. Histopathologically , the epithelial basement membrane has poorly functioning adhesion complexes leading to a weak attachment of epithelium to Bowman’s membrane; making these corneas more susceptible to spontaneous or recurrent erosions 1 (RES) . Any break in the epithelium can predispose a cornea to microbial infection. One study of corneal infections (n=1786) reported 0.6% were secondary to 2 RES . In our experience EBMD is a small, but real, risk for infectious keratitis. Clinical photograph of a patient with epithelial basement dystrophy Courtesy of Edwin S. Chen, MD Histopathology of degenerated epithelial cells trapped in abnormal epithelium; presents clinically as a microcyst. Courtesy of Ralph Eagle, MD To describe infectious keratitis due to underlying hereditary EBMD and EBM changes from previous trauma. We performed a retrospective chart review of patients with infectious keratitis secondary to EBMD from 1/1/2007 to 9/30/2009 at a tertiary care center. Patients with recent trauma, bullous keratopathy, or contact lens wear were excluded. Laterality of EBMD changes, history of remote trauma, RES, and social, medical and ocular history were recorded. The active treatment for the keratitis, duration of follow-up and time to resolution, vision as well as culture results and complications were also noted. Thirteen patients were identified. All patients were referred for consultation after onset of infection and initiation of some form of treatment. Average age at onset of the infection was 61.6 +/-12.8 years; 61.5% were female. All cases had unilateral infections; 61.5% were of the right eye. 92.3% had EBMD in both eyes 23.1% had reported history of remote trauma in the affected eye 46.2% had reported history of RES in the affected eye. Clinical findings on presentation included infiltrate (100%), epithelial defect(85%), hypopyon(23%), and stromal edema(69%). All were treated with topical antibiotics 8 (61.5%) were cultured: 5 (62.5%) of those were positive st 6 (46.2%) patients were started on fortified antibiotics/antifungals on their 1 visit. Pathogens included S. aureus, S. epidermidis, P. aeruginosa, MRSA, and Candida. One patient was hospitalized and treated for corneal perforation. 5 Not cultured Tx= flouroquinolones Candida & haemophilus 3=No Growth 13 Patients Coag-neg Staph 8 Cultured 5=Positive Staph Aur. Pseudomonas MRSA Pt/ Sex Age EBMD Tr. Hx RES Culture Treatment/Course F/u VA on Final Present- VA 1/F 50 OU + + 2/F 66 OU - UK Not done polysporin oint; new hypopyon w/ d/c of moxiflozacin –restarted;Pred Ac. 1% added day 68 Gatifloxacin, ciprofloxacin oint 1 visit 3/F 92 OU - UK Not done Gatifloxacin, polysporin oint, BCL 6 days 20/200 20/40 4/F 56 OU - + Not done Bacitracin oint 1 visit 20/20 5/M 52 OU + + Candida & Topical F. gentamycin, F vancomycin, voriconazole, atropine, PO cefazolin, timolol, * 305 days 20/80 20/50 Day 4 perforation repaired with glue & BCL, PO voriconazole, brinonidine, hemophilis ation No Growth Topical Voriconazole, amphotericin, and moxifloxacin; oral voriconazole; atropine; dorzolamide, moxifloxacin, F. cefazolin, F. tobramycin, scopolamine 99 days 20/400 20/60 20/20 3 days 20/80 20/40 89 days CF UK Coag Neg Atropine, topical levofloxacin, erythromycin oint Staph UN Not done Topical levofloxacin, azithromycin ophthalmic solution 35 days 20/30 20/30 9/F 52 OS - - Not done Topical levofloxacin, polysporin oint 10 days 20/50 20/40 10/M 58 OU UK + S. Aureus F. cefazolin, F. tobramycin, cyclopentolate 1 visit CF 11/F 81 OU + 45 days HM 12/F 59 OU - UN Pseudomo Topical gatifloxacin, F. cefazolin, scopolamine, muro oint, ciprofloxacin oint, PO doxycycline, Day 31 Pred Ac 1% added nas UN No Growth Topical F. Vancomycin, F. gentamycin, scopolamine, polysporin oint, Day 22 13/M 50 OU UK + 107 days CF 6/F 65 OU - - 7/M 52 OU - + 8/M 68 OU No Growth MRSA loteprednol added Topical F. cefazolin, F. tobramycin, scopolamine, polysporin oint, moxifloxacin, Day 19 loteprednol added 20/40 20/20 0 53 days 20/70 20/30 20/25 3-8 # of patients 3 cultured; all were pos: Pseudomonas; S. aureus (2) McElvanney (1999) Tabery (1998) 2 cultured = all neg Ionides (1997) 11 cultured = S. aureus (2) 1 cultured = all neg Jaros (1986) 5 cultured = all neg Shoch (1985) 0 2 4 6 8 10 12 EBMD is known to cause considerable morbidity including ocular pain, RES and decreased 8 vision . Infectious keratitis is a vision threatening complication that can lead to scarring and perforation. Our series had a 62.5% culture positivity rate with a wide variety of organisms. Given the serious ocular morbidity associated with infectious keratitis we recommend intense antimicrobial treatment as first line therapy. When counseling patients regarding the prognosis and treatment of EBMD or faced with an ulcer of unknown etiology, ophthalmologists should consider the possibility of infectious complications caused by EBMD. 1. Anterior Segment The Requisits. Rapuano, Luchs, Kim. Mosby, 2000. 2. Ibrahim YW, Boase DL, Cree IA. Epidemiological characteristics, predisposing factors and 3. 4. 5. 6. 7. 8. 9. 10. microbial profiles of infectious corneal ulcers: the Portsmouth corneal ulcer study. Br J Ophthalmol. 2009;93:1319-1324. Schoch DE, Stock EL, Schwartz, AE. Stromal keratitis complicating anterior membrane dystrophy. Am J Ophthalmol. 1985;100:199-201. Jaros PA, DeLuise VP. Stromal keratitis with anterior membrane dystrophy. Ann Ophthalmol. 1986;18: 283-284. Ionides ACW, Tuft SJ, Ferguson VMG, Matheson MM, Hykin PG. Corneal infiltration after recurrent conreal epithelial erosion. Br. J Ophthalmol. 1997; 81:537-540. Tabery HM. Corneal stromal infiltrates in patients with recurrent erosions. Acta Ophthalmol. Scand. 1998;76:589-592. McElvanney AM. Hypopyon keratitis in corneal epithelial basement membrane dystrophy. Eye. 1999; 13:585-586. Trobe, JD, Laibson PR. Dystrophic changes in the anterior cornea. Arch Ophthal. 1972; 87:378382. Hykin PG, Foss AE, Pavesio C, Dart JK. The natural history and mangement of recurrent corneal erosion: a prospective randomised trial. Eye (London). 1994;8:35-40. Reidy JJ, Paulus MP, Gona S. Recurrent erosions of the cornea. Cornea. 2000;19(6):767-771.