Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
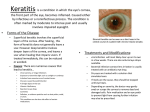
Cornea hystology Bacterial keratitis • • • • • • • • • • • • ETIOLOGY: Staphilococcus, Streptococcus, Pseudomonas, Klebssiela PREDISPOSING FACTORS: contact lens wear (Pseudomonas);ocular surface disease, trauma, dry eye;chronic dacryocystitis, administration of topical and systemic immunosupressive agents;keratorefractive incisional surgery. DIAGNOSIS: Acute hypopyon ulcer = severe bacterial inflamation of the cornea associated with pus in the anterior chamber (hypopyon) and a severe iridocyclitis; Streptococccus pneumonie is the usual cause;the corneal ulcer is a dirty gray color, with overhanging margins + thick mucopurulent exudate the infection may progress rapidly and result in corneal perforation Pseudomonas keratitis is more common in men;the ulcer begins usually centraly;it qiuckly broodens and deepens, and has a fulminating course the corneal stroma appears to disolve into a greewish-yellow mucous discharge;marked anterior chamber reaction and hypopyon 3. Enterobacteriaceae usually cause a shallow ulceration, grey-white pleomorphic suppuration + diffuse stromal opalescence; the endotoxins induce ring-shaped corneal infiltrate (“corneal rings”). Bacterial keratitis – Central ulcer with hypopion Treatment • • • • • • • • • • MANAGEMENT: first step is to collect material by scraping the ulcer with spatula, stained Gram and Giemsa for cytology and plated on the media corneal biopsy – when an infection fails to resolve in spite of antimicrobial treatment initial treatment with concentrated antibiotic eyedrops is based on the result of Gram stain; after the isolation of te causative organism may indicate specific therapy. Gram – organisms are treated with aminoglycosisdes(gentamicin, tobramicin);Gram + with Cefuroxime and ciprofloxacin; for this reason the initial treatment should be with a combination of a fortified aminoglycoside + ciprofloxacin; Subconjunctival injections – in severe infection, particularly when the visual axis is involved Sistemic antibiotics are not routinaly used. The initial antibiotics should be changed only if a resistant pathogen is grown and the ulcer is progressing. 1% atropine solution – 2 or 3 times daily to prevent the formation of posterior synechiae and reduce pain from ciliary spasm; corticosteroids therapy is controversial (only when cultures become sterile ). It is necessary to keep the dress on the eye; if there is a severe corneal necrosis a bandage contact lens may be used . Viral keratitis Herpes simplex keratitis • • • • • • • • • • • • • Is common in 90 % of the population HSV is subdivided into 2 types:HSV-1 cause facial, oral or ocular lesion; HSV-2 associated mainly with genital infections Primary ocular infections appears as a blepharocojunctivites and epithelial punctate keratitis; Epithelial infections: Dendritic ulceration (is cause by live virus): the disease begins with puncate epithelial opacites that becomes vesicular and coalesce in a branching linear pattern which staines with fluorescein; corneal sensitivity is diminished;stromal infiltrates appears under the ulcer; simptoms: foreign body sensation, lacrimation and decrease in VA Geographic ulceration : when the epithelium between the dendrites is lost results a sharply demarcated, irregularily shaped geographic ulcer; stromal interstitial keratitis – cause by active viral invasion and destruction; durring the attack stroma shows a cheesey necrotic appearance or a profound interstitial opacification;may associate anterior uveitis disciform keratitis – is cause by a reactivated viral infection or an exagerated hypersensitivity reaction to antigen.It consist of a disc-shaped, localized grayish area of stromal edema + localized keratic precipitates (the edema may involve the full thickness of the cornea); DENDRITIC ULCER DISCIFORM KERATITIS • • • • • • • • • • • • • Treatment Antiviral drugs: acycloguanosine – 5 times daily trifluorothymidine – every 2 hours during the day idoxuridine Initial treatment is drops or oiment, after healing has occurred, medication should be quickly tapered and discontinued by day 14. Debridement – after topical anesthesia, the cells are removed with moist cotton-tipped applicator or scalpel blade (the removal of the virus-containing cells protects adjacent healty cells from infection and eliminated the antigenic stimulul to stromal inflamation) Cycloplegic agents – Atropine, scopolamine, midryum Corticosteroids are indicated only in stromal keratitis (if the visual axis is involved, topical steroids + antiviral cover). Dendritic epithelial disease: topical antiviral + debridement; Stromal keratitis: topical antiviral + topical corticosteroids Postinfections ulcers: encouraging epithelial healing The role of sustained antiviral prophylaxis is not clear. HERPES ZOSTER KERATITIS Numular keratitis • • • • • • • • • • • • • Is caused by human herpes virus 3 Zoster mainly affects elderly patients and is rare in children; ussualy presents as a combination of 2 or more the following forms: conjunctivitis, episcleritis, scleritis, keratitis, iridocyclitis and glaucoma; Keratitis (occurs in about 40% of all patients), as a Fine punctate epithelial keratitis +/- stromal edema; Dendritic ulceration (can be mistaken with HSV); Numular keratitis (multiple fine granular deposits) Disciform keratitis. Treatment: Antiviral sistemic ACYCLOVIR (800mg 5 times daily for 10 days); FAMCICLOVIR, VALACICLOVIR - decrease the pain, stop visual progression and reduce incidence and severity of keratitis; Sistemic steroids – inhibit development of postherpetic neuralgia (must be limited to patients 50 years of age or older, in severe scleritis, uneitis and orbital inflamations); CIMETIDINE – 300mg p.o. qid if periocular edema and pruritus are excessive. Postherpetic neuralgia is treated with lidocaine gel, amynotripttyline (12,5-25mg). Topical ACYCLOVIR or trifluridine or topical steroids. FUNGAL KERATITIS • • • • • • • • • • • after topical administration of corticosteroids and antibiotics the most common fungi are : Aspergillus, Candida, Fusarium Clinic: ulcer appears as a greywish – white with a shallow crater, which is surrounded by a sharply demarcated halo that persist 4 month Less specific findings include satellite lesion Scrapping the base and edges of the ulcer is essential for the diagnosis; A culture result can be obtained within 48-72 hours Treatment: -topical 1% solutions of miconazole, clotrimazol or ketokonazol -sistemic itraconazol or ketokonazol may be helpful in severe cases -therapeutic penetrating keratoplasty may be required in unresponsive cases -corticosteroids is always contraindicated. COENEAL LACERATION