Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
Hematopoietic Growth Factor Expression and ATRA Sensitivity in Acute
Promyelocytic Blast Cells
By Carolline Dubois, Marie Helene Schlageter, Albane de Gentile, Fabien Guidez, Nicole Balitrand,
Marie Elisabeth Toubert, Irene Krawice, Pierre Fenaux, Sylvie Castaigne, Yves Najean, Laurent Degos,
and Christine Chornienne
Acute promyelocytic leukemia(APL) is a homogeneous subgroup of acute myeloid leukemias (AMLs) characterized by
the presence of the t(15.17) translocation and the resulting
promyelocytic myeloid leukemia/retinoic acid receptor a
(PML/RARa) fusion proteins. To date APL is the onlyAML
that issufficiently sensitivet o all-trans retinoic acid’s (ATRA)
differentiating effect. In vivo ATRA alone achieves complete
remission in mostAPL patients. However, failure or partial
responses are observed and the molecular basis of the absence of ATRA response in these patients has not been dedifferentiatermined. To gaininsights in the cell growth and
tion ofAPL cells,expression of hematopoietic growth factors
(HGF) shown t o be produced by leukemic cells (interleukinl p [IL-lp], IL-6, tumor necrosis factor a (TNFa), granulocyte
colony-stimulating factor [G-CSF], granulocyte-macrophage
colony-stimulating factor [GM-CSF], and IL-3) was studied
in 16 APL samples. Twelve APL cases expressed IL-lp, IL-6,
and TNFa, but not G-CSF,GM-CSF, and IL-3. These cases
achieved complete remission with ATRA therapy. The four
remaining patients (either TNFa negative or G-CSF, GM-CSF
or IL-3 positive) did not achieve complete remission with
ATRA. In all cases, in vivo response t o ATRA therapy was
correlated to the in vitro differentiation effect of all-trans
retinoic acid
mol/L. Thus,
ATRA differentiation induction was strongly correlated to the HGF expression ( P <
.0001). These results suggest that the presence or absence
t o t htherae
of HGF‘s expression by APL cells may contribute
peutic effect of ATRA in this disease.
0 1994 b y The American Society of Hematology.
A
phenotypic and genetic markers. The presence of the t( 15;17)
translocation and the identification of promyelocytic myeloid
leukemidretinoic acid receptor a (PMWRARcu) fusion transcripts in APL patients strongly support the hypothesis that
both the t( 15;17), and thus PMLRARcu, play a crucial role
in the leukemogenesis of this disease.’ Clinically, APL is
characterized by hemorrhagic episodes caused by disseminated intravascular coagulation (DIC) and primary fibrinolysis,“’ withan accumulation of hypergranular promyelocytes in the BM. Furthermore, APL cells are specifically
responsive to all-trans retinoic acid (ATRA) and this characteristic has allowed the first differentiation therapy with retinoic acid.”,” However, failure or partial responses are observed and, though this has most frequently been reported
in patients at second or third relapse,” the molecular basis
of the absence of ATRA response in these patients has not
been determined.
The present investigation was initiated to characterize the
expression andproduction of HGF byAPL cells togain
further insights into the leukemogenesis and RA sensitivity
of this leukemic subtype.
CUTE MYELOID LEUKEMIA (AML) is a malignant
process that results from the accumulation in the blood
and bone marrow(BM) of myeloid precursor cells characterized by abnormal growth and differentiation arrest. Both
autocrine and paracrine hypotheses have been brought forward to suggest possible mechanisms for the transformation
and invasive process. AML cells have been shown to express
the genes or produce a variety of hematopoietic growth factors (HGFs), including granulocyte colony-stimulating factor
(G-CSF), granulocyte-macrophage colony-stimulating factor
(GM-CSF),’ and cytokines such as interleukin-l (IL-l), IL6,2-5and tumor necrosis factor cu (TNFcu).’ Possible use of
these factors by the AML cells themselves (GM-CSF, GCSF, IL-6, IL-I) or by accessory cells (TNFcu, IL-l) may
be responsible for both the autocrine/paracrine growth stimulation of the AML cell^,'^*^^^^ and the induction of leukemic
cell differentiation.’
Little data concerning the expression and secretion pattern
of growth factors by acute promyelocytic leukemia (APL)
cells have been reported in the literature. APL, the AML3
French-American-British (FAB) classification subtype,Ris a
rare subgroup of AML (less than 10%) characterized by
From the Laboratoirede Biologie Cellulaire HematopoiZtique,
Institut d’Hkmatologie; Service de Mkdecine Nuclkaire; Service des
Maladies du Sang, Institut d’Himatologie, H6pital Saint Louis,
Paris, H6pita1, Claude Huriez, Lille, France.
Submitted October 23, 1993; accepted January I , 1994.
Supported in part by grants fromthe Ligue contre le Cancer, the
Association de la Recherche contre le Cancer and the Fondation de
la Recherche contre les Leuckmies.
Address reprint requests to C. Chomienne, MD, Laboratoire de
Biologie Cellulaire Hematopoi’ktique, Centre Hayem, Hbpital Saint
Louis, I ave Claude Vellefaux, 75010 Paris, France.
The publication costsof this article were defrayed in part by page
charge payment. This article must therefore be hereby marked
“advertisement” in accordance with 18 U.S.C. section 1734 solely to
indicate this fact.
0 1994 by The American Society of Hematology.
0006-4971/94/8311-0012$3.00/0
3264
MATERIALS AND METHODS
Patient samples andprimary culture. BM or blood samples from
24 consenting AML patients were collected in heparinized tubes
before any therapy. From these 24 patients, 16 were AML3 or APL.
and 8 other AML subtypes (3 AMLI, 3 AML2, I AML4, I AML5).
The diagnosis was established by morphologic, according to the
FAB criteria,’ and cytogenetic criteria. Hematologic characteristics
of the APL patients are summarized in Table 1.
The leukemic cells were isolated by Ficoll-Hypaque gradient (Eurobio, France; density: 1,078 g/dL) centrifugation and enriched after
monocyte adherence to plastic for 1 hour at 37°C. The AML blasts
were then immediately prepared for in vitro suspension culture, the
cells were incubated for up to 72 hours inRPM1 1640 medium
supplemented with 15% fetal calf serum (FCS), L-glutamin (2 m o l /
L), and antibiotics (GIBCO-BRL, France) at 37°C in humidified 5%
CO, atmosphere as previously de~cribed.’~
The initial cell concentration was IO6 cells/mL and cytospin slides stained by May-Griinwald
Giemsa technique and flow cytometry analysis after CD14 labeling
showed the population to contain less than 1% of normal mononuBlood, Vol 83, No 11 (June I ) , 1994: pp 3264-3270
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
HGF EXPRESSION AND ATRA SENSITIVITY IN APL
3265
Table 1. Hematoloaic Characteristicsof APL Patients at Presentation and Response to ATRA
ATRA Response
Patient No.
FAB
Genetic Analysis
Status
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
AML3
AMLB v
A M L3
AMLB
AML3
AML3
AML3 v
AMLB
AMLB
AML3
AMLB
AML3
A M L3
AML3 v
AML3 v
AML3
t(15;17)
t(15;17)
t(15;17)
t(15;17)
t(15;17)
t(15;17)
t(15;17)
t(11;17)
t(15;17)
t(15;17)
t(15;17)
t(15;17)
t(15;17)
t(15;17)
t(15;17)
t(15;17)
De novo
1st Relapse
De novo
2nd Relapse
De novo
Coagulopathy
1st Relapse
2nd Relapse
1st Relapse
1st Relapse
1st Relapse
1st Relapse
De novo
2nd Relapse
De novo
1st Relapse
De novo
+
+
+
-
+
+
-
+
+
+
-
+
+
+
+
+
% BM Blasts
WBC Count
In Vitro
In Vivo
50
90
92
100
95
18,000
87,000
42,000
4,300
80,000
2,000
33,000
4,540
4,200
25,000
3,000
69,000
3,000
17,500
10,400
1,300
100
49
96
99
98
CR
F
CR
CR
CR
34
93
40
79
91
100
99
0
a2
92
90
F
CR
PR
CR
CR
90
95
88
100
82
40
89
80
96
90
65
CR
CR
F
CR
CR
CR
Abbreviations: FAB, French-American-British morphological classification*; AML3 v. AML3 variant; t(15;17), translocation (15;17); t(11;17),
translocation (11;17)13; WBC, white blood cell; ATRA Response In Vitro, percent of NBT positive cells after 5 days of incubation with all-trans
retinoic acid lo-' mol/L; ATRA Response In Vivo: CR. complete remission; PR, partial remission; F, failure after 90 days of therapy with all-trans
retinoic acid 45 mg/m2/d.
clear cells. After incubation, cell aliquots were taken for cell viability, RNA extraction, and detection of CSF, and cytokine production
was performed in the supernatants. For each sample, differentiation
with ATRA was assessed at day 5 of culture by morphology, and
the generation of superoxide anion 0'- production was visualized
by the nitroblue tetrazolium reduction assay as already de~cribed.'~
Cell viability was assessed by the trypan blue exclusion dye test.
Proliferation curves were established for each case and an index
ratio (viable cell count after 72 hours versus cell count at hour 0)
was calc~lated.'~
Culture of control hematopoietic cells and cell lines. Normal
peripheral blood lymphomononuclear cells were isolated from heparinized normal blood samples after Ficoll-Hypaque gradient. Then,
thepurified cells were stimulated with phorbol 12-myristate 13acetate 10"' mol/L (PMA) and phytohemagglutinin 2 pg/mL (PHA)
for 6 hours, in the same medium used for AML cell culture. The
promyelocytic cell line NB4 (a gift from M. Lanotte, Paris, France)
was grown inRPM1 1640 medium supplemented with15% FCS
and the 5637 human bladder carcinoma cell line was grown in RPM1
1640 with 5% FCS.
Biologic assay for G-CSF. G-CSF levels in supernatants collected from the leukemic cell culture after 72 hours were estimated
by monitoring the proliferation of NFS-60 cells. The leukemic cell
culture supernatants were concentrated (10- to 40-fold) by ultrafiltration with a Centriprep concentrator 10 (Amicon, Danvers, MA)
to increase the detectable level of G-CSF. NFS-60 cells (2 X lo4)
together with 25 pL of concentrated supernatants were cultured in
each well of a microtiter plate at 37°C for 48 hours in humidified 5%
CO2.Then 10 pL of M l T (3[4,5-dimethyl-2-thiazolyl-2,5-diphenyl2Hltetrazolium bromide) were added. The plate was incubated for
5 hours at 37°C. Dimethylsulfoxide (125 pL) was added and the
optic density was measured at 550 nm. Thus, samples to be. tested
were titrated and related to an internal standard preparation. The
sensitivity of this G-CSF assay was shown to be 10 pg/mL. The
interassay coefficient of variation at level of 100 pg/mL was less
than 10 (n = 6). As positive controls, cell culture mediums from
lymphomononuclear cells stimulated by PMA and PHA and 5637
cell line were collected and tested.
GM-CSF, IL-3, IL-IP, TNFa and IL-6 enzyme-linked immunosorbent assay (ELISA). GM-CSF levels in the leukemic cell culture
supernatants were estimated by an ELISA kit from Endogen (Boston,
MA), and IL-3 levels by an ELISA kit from Amersham (Buckinghamshire, UK). For IL-l@, TNFa, and IL-6 levels, we have used
ELISA kits from British Biotechnology (Oxford, England). GMCSF, IL-3, IL-ID, and IL-6 ELISA were sensitive down to a concentration of 3 pg/mL and for TNFa ELISA, sensitivity was shown to
be 12 pg/mL. For a secretion level of 100 pg/mL, the interassay
coefficient of variation was less than 10 (n = 6). As positive controls,
culture mediums from lymphomononuclear cells stimulated by PMA
and PHA and 5637 cell line were collected and tested. Concentrated
leukemic cell culture supernatants were used for GM-CSF and IL3 detection. The results were expressed in pg/mL and in pg/106cells,
but no difference between these expressions were observed.
Northern blot analysis. Total cellular RNA from AML blasts
was prepared by the guanidium isothiocyanate/cesium chloride cenBriefly, 20 or 30
trifugation method as described by Davis et
pg ofRNA were size fractionated by agarose gel electrophoresis
after denaturation in formamide loading buffer and transferred onto
nitrocellulose membranes. These filters were prehybridized and hybridized at 65°C overnight in buffers containing 6X sodium chloride/
sodium citrate (SSC), 0.2% sodium dodecyl sulfate (SDS), and lox
Denhart's solution. DNA probes were ['*P]-labeled by the multirandom priming method. After hybridization, the filters were washed
under stringent conditions in 2X SSC, 0.1% SDS for 10 minutes
twice at room temperature and then in 0.1X SSC, 0.1% SDS at 65°C
for 10 minutes. The filters were autoradiographed at -80°Cwith
intensifying screens for 2 days. As positive control for screening
test, RNA from PMA- and PHA-stimulated lymphomononuclear
cells and from the 5637 cell line were used.
DNA probes. cDNA probes for G-CSF and GM-CSF were
kindly provided by Glaxo Laboratories (Lausanne, Switzerland).
cDNA probes for IL-lP, TNFa,and IL-6 were obtained from British
Biotechnology. A rat glyceraldehyde-3-phosphate dehydrogenase
(GAPDH) probe was used to rehybridize the filters and normalize
RNA expression.
Reverse transcription polymerase chain reaction (RT-PCR).
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
DUBOIS ET AL
3266
APL
APL
Onemicrogram of total cellular RNA wasreversetranscribed to
cDNA byan incubation of 45 minutes at37°Cand 5 minutes at
99°C in a total volume of 20 pL containing I x RT buffer (50 mmoll
L TRIS HCIpH 8.3, 6 mmol/L MgCL, 40 mmol/L KCI, 10 mmoll
L dithiothreitol), 1 mmol/L each deoxynucleotide triphosphate(Pharmacia.Piscataway,NJ).12.5
U ofAvian
myeloblastosisvirus
(AMV) reverse transcriptase (Boehringer, Indianapolis, IN) and 2.5
pnol/L of randomhexamers (Pharmacia). ThecDNAfragments
were amplified by using 2.5 U of Thermus aquaticus (Taq) polymerase (Perkin Elmer-Cetus, Norwalk. CT) and 30 pmol of each specific
primer for one cytokine in a total volume of 50 pL containing 1X
PCR buffer (10 mmol/L TRIS HCI, 50 mmol/L KCI). Reaction times
consisted of 30 cycles ( 1 minute at 94°C. 2 minutes at 60°Cor 55°C.
3 minutes at 72°C) andat the end 7 minutes at 72°C. Ten microliters
of the amplified products was electrophoresed on 2% agarose gel
stained with ethidium bromide.
The gels were transferred onto a nylon filter and hybridized to 5'
end-labeled oligonucleotides with 32Pusingpolynucleotidekinase
for 30 minutes. Then the filters were washed and exposed to Kodak
X-OMAT film (Eastman-Kodak, Rochester, NY) at -80°C with intensifying screens for a specific number of hours. Contamination
was avoided by stricttechnicalmethods. In all experiments,two
negative controls were carried through all the steps with the other
samples. Confirmationof the results was assessed by performing the
RT-PCR at least twice for each primer pair.
Primers used for the PCR were as follows: G-CSF, 5' CCCCCTGGGCCCTGCCAGC 3', 5' CTGCCAGATGGTGGTGGCA 3';
GM-CSF. 5' AGAGACACTGCTGCTGAGA 3'. 5' ATAATCTGGGTTGCACAGG 3'; IL-3, IL-ID, TNFcu,and IL-6primerswere
purchased from Clontech Laboratories (Palo Alto, CA). Oligonucleotide probes were as follows: G-CSF, 5' GTGAGGAAGATCCAGGGCGA 3'; GM-CSF, 5' ACCTGCCTACAGACCCGCCT3';
IL-3. 5' CAAGACATTCTGATGGAAAA3'; IL-ID, 5' CCATATGAACTGAAAGCTCT 3'; TNFcY, 5' CTGCACTTTGGAGTGATCGG 3'; IL-6, GCCAGAGCTGTGCAGATGAGTAC 5'.
Immunoenzymaric staining of TNFcu. Cytocentrifuged APL cell
NON-APL
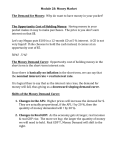
Fig 1. HGF production and in
vitro characteristics of APL and
non-APLcells
G, G-CSF; GM,
GM-CSF; ATRA response
in
vitro, percentof NBT positive
cells after 5 days of incubation
with all-trans retinoic acid
mol/L; in vitro growth, 72 hours
index ratio: viable cell count ratio at 72 hours versus day 0 of
cell culture in the presenceof
15% fetal calf serum alone. Asterisk indicates cases for which
cytokine secretion analysis was
made.
preparations were fixed in acetone, air dried, and stocked at -20°C
until use. lmmunostaining was performed by the alkaline phosphatase antialkaline phosphatase (APAAP) procedure as previously described.'" The TNFcr antibodies werepurchasedfromGenzyme
(Cambridge, MA).
RESULTS
In vivo and in vitro charncteristics of ~ k APL
e
CUSES sludied. (Table l). Sixteen APL cases were studied (patients I
through 16). All patients were cytologically defined as APL
leukemia; one case presented with a t( 11;17) translocation."
Nine cases showed increased white blood cell (WBC) counts
at presentation. All patients were treated with all-trans retinoic acid according to the previously published protocols."."
Only four cases (patients 2, 6, 8, 13) did not achieve complete remission withATRAtherapy alone. Leukemic cell
suspension culture was performed in all cases at diagnosis.
Four samples (patients 2, 6, 8, 13) showed poor to no differentiation (49%, 34%, 40%, 0% of nitroblue tetrazolium
(NBT) positive cells respectively) in the presence of ATRA
IO-(' mol/L, corroborating the absence of in vivo ATRA
efficacy. Ten cases showed spontaneous increase of viable
cells in vitro (index ratio 21.2) (Fig l ) . Four of these cases
(patients 1, 7, 9, 16) hadanindex ratio greater than 1.4.
However, increased WBC at diagnosis was not correlated to
the spontaneous increase of cell number in the suspension
culture.
Secretion of HGF (IL-I@,TNFa, IL-6, G-CSF, GM-CSF,
and IL-3) by APL cells. Secretion of HGF was studied in
culture supernatants of highly enriched blast cell populations
of seven APL patients (patients 1 through 4 and 14 through
16). All of these seven cases secreted IL-I@ (median level,
1 1 pg/mL), TNFa (median level, 25 pg/mL). and IL-6 (me-
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
HGF EXPRESSION AND ATRASENSITIVITY
3267
IN APL
m
D
m
* -.
API?
m
H
I-csi
II
D
m
t
-1.4
T N F a IL-6 G-CSF CY-CSi
NON APL
IL3 1
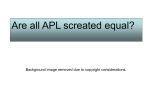
Fig 2. Secretion levels of IL-lp, TNFa, IL-6, and CSFs (G-CSF, GMCSF, IL-3) by APLcells and non-APL cells. APL*, ATRA-responsive
APL (patients 1, 3, 4, and 14 to 16). Secretion analysis was made
after 72 hours of cell culture, by ELlSA kits for IL-lp, TNFa, IL-6, IL3, and GM-CSF, and by biologic assay for G-CSF. Values represent
means of triplicate wells.
dian level, 66 pg/mL) (Fig 2). Out of these seven cases, one
case secreted IL-3 and GM-CSF (patient 2), and no cases
secreted G-CSF. Case 2 did not respond to ATRA in vitro
and in vivo. When kinetic studies (day 0 to day 6) were
performed, secretion of IL-lp, IL-6, and TNFa was shown to
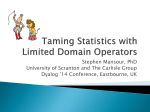
be stable and not induced by the culture. Immunoenzymatic
staining with TNFa antibodies in APL cells confirmed that
APL cells are in fact responsible for the TNFa secretion
detected (Fig 3). Study of the NB4 promyelocytic cell line
supernatant detected IL-lp, TNFa,and IL-6, but no G-CSF,
GM-CSF, and IL-3 (data not shown).
Expression of HGF (IL-ID, TNFa, IL-6, G-CSF, GMCSF,and IL-3) by APL cells. To further characterise the
presence or absence of HGF by APL cells, mRNA expression studies were performed. L - l p , TNFa, and IL-6 RNA
levels were detectable by RT-PCR (Fig 4B) and Northern
blotting analysis (Fig 4A), the latter confirming the normal
size of the transcripts. Expression of IL-lp, TNFa, and IL6 gene was analyzed in 13 APL cases (patients 1 through
13). IL-lP and IL-6 were detected in all APL cases, and
TNFa in 11. Gene expression analysis of these HGFs in
cells freshly isolated showed that APL cells spontaneously
expressed IL-lp, TNFa, and IL-6 (data not shown). Compared with the positive controls (the 5637 cell line and
lymphomononuclear cells stimulated by PMA and PHA), no
G-CSF and GM-CSF mRNA expression could be detected
by Northern blotting analysis in APL cells (Fig 4A).
To increase RNA sensitivity detection, RT-PCR was performed (Fig 4B). G-CSF mRNA was detected in only one
case of the 13 samples studied (patient 6), GM-CSF mRNA
in another case (patient 2 ) and IL-3 mRNA in 3 cases (patients 2, 6, and 13).
In summary, of the 16 APL cases tested for expression
andor secretion of HGF, 12 cases (80%) coexpressed or
cosecreted IL-lp, TNFa, and IL-6, but not G-CSF, GMCSF, and IL-3. Furthermore, when expression and secretion
could be performed in the same sample, presence or absence
of gene expression was always associated with the release
or absence of the corresponding protein.
Expression and secretion of HGF by non-APL cells. In
eight non-APL samples tested, CSF expression was detected
in four cases (one case, G-CSF; one case, GM-CSF; one
case, G-CSF + GM-CSF; and one case, G-CSF + GM-CSF
+ IL-3) (data not shown). All cases expressed IL-1p and
IL-6 genes, butonly four cases the TNFa gene (Fig 4).
Higher levels of CSFs and cytokines were observed in these
non-APL cases as compared with APL cases (Fig 2). Only
one case (AML2) expressed IL-lp, TNFa, IL-6, butno
CSFs. Leukemic cell infiltration and leukemic cell purification were the same in this non-APL population as for the
APL samples, implying that random contamination by normal HGF-secreting cells cannot explain the difference between APL and non-APL samples.
HGFproduction by AML cells and in vitro characteristics.
(Fig 1) In vitro cell growth and viability of AML cells was
studied in a suspension culture system with standard condition medium by comparing viable cell counts at different
time intervals with the number of seeded cells at day 0 of
culture. Compared with non-APL cases, APL cells showed
a better survivaUgrowth in suspension culture. Only 3 APL
cases had an index ratio less than 1 (patients 2, 8, 13).
Among the 10 cases thatshowed in vitro leukemic cell
growth (patients 1, 3 through 7, 9, 10, 12, 16), 9 cases
expressed IL-lp, TNFa, and IL-6, but not CSFs.
ATRA sensitivity was also analyzed. Induction of differentiation was assessed by morphologic and functional criteria (NBT
test). Twelve of the 16 APL cases studied (patients 1,3 through
5, 7, 9 through 12, 14 through16)achieveddifferentiationin
vitrointhepresenceofATRA
m o m (meanof 94 2 6%
NBT positive cells) and complete remission with ATRA therapy
invivo. Thesecases all coexpressedorcoproduced
Lip,
TNFa, and L-6, but not CSFs. The 4 APL cases that failed to
respond significantly to ATRAtherapyneverexceededmore
than 50% of differentiation and either expressed CSFs or did
notproduce TNFa. Non-APLcasesdidnotshowsignificant
induction of differentiation by ATRA (varied from 0% to 20%
with a meanof 5.5%) invitro.Thus,ATRAdifferentiation
induction was strongly correlated to the pattern of HGF expression ( P = .OOO1 Fisher test).
DISCUSSION
This is the first study describing the coexpression of HGF
in the APL subgroup of AML. We observed that of the 16
APL cases surveyed in this study, all but 4 cases were (IL-
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
DUBOIS ET AL
3268
Fig 3. Expression of TNFa in
APL cells. TNFa was detected in
the cells byimmunoenzymatic
staining (APAAP procedure). (A)
shows the procedure was made
with TNFa antibodies.(B) shows
the
procedure
made
without
TNFa antibodies.
l p , IL-6, TNFa)positive and (G-CSF, GM-CSF, IL-3) negative. These results are corroborated by the presence of TNFa
in the APL cells by immunostaining, and by preliminary
studies from our laboratory and other published data hinting
at the absence of detectable G-CSF and GM-CSF levels and
increased L - 6 levelsr7in the serum of APL patients. This
pattern was specifically correlated to ATRA sensitivity in
vitro and in vivo. Interestingly, the four patients whose leukemic cells did not express TNFa or did express CSFs,
did not achieve complete remission withATRA therapy.
Likewise non-APL cases that do not respond to ATRA, did
not show the HGF expression pattern. Thus, part of the effect
of ATRA's efficacy may be the result of the growth factor
pattern spontaneously expressed by APL cells. Differentiation of leukemic cells (cell lines and fresh blast in primary
culture) can be induced by CSFs, TNFa, and interferons
in association with all-trans retinoic acid (ATRA).'8-20The
presence of these HGF expressions by APL cells may be
involved in the in vitro sensitivity of APL cells to differentiate in the presence of ATRA. To evaluate the potential role
of any of these growth factors, we have initiated in vitro
assays using antibodies and antisense oligonucleotide probes
to suppress each growth factor individually. In fact, the two
patients whose cells did not express TNFa did not respond
in vivo to ATRA therapy. A further question asked by the
results presented here is whether the expression of HGF by
APL cells has a relevance to these cells' proliferation or
survival features in vitro. APL cells are noted to have a low
doubling time:' and absence of autonomous growth.22These
characteristics may be related to previously reported high
levels of transforming growth facto? and to TNFa production and absence of IL-3, GM-CSF, and G-CSF secretion
shown in this study. Nevertheless, in the presenceofadded
CSFs such as GM-CSF, APL cells are able to produce colonyforming unit-leukemia coloniesz4 and to show increased cell
growth.'4 This growth induction in the presence of GM-CSF
is not surprising because we have shown APL cells to express
high atkity GM-CSF receptors.z In addition, the secretionof
IL-lp and IL-6 by APL cells may, alone or in cooperation
with the CSFs present inthe culture medium, explainthe good
survival of APL cells in suspension culture.26
Clinically, APL is characterized by the presence of blood
coagulation disorders and hyperleukocytosis at onset, mainly
in the AML3 variant subtype." IL-10 has been reported to
be linked to DIC in AML patient^.'^ The constant presence
of IL-lp in APL cells may explain the predisposition of
APL patients to present altered blood coagulation parameters. Contrary to what mayhave been expected, the cytokine/
CSF production did not correlate with high WBC count at
presentation. This suggests that other factors determinant for
leukemic cell proliferation, such as egress from the BM,
adhesion, and migration are probably involved. One of
ATRA therapy's main side effects is the induced ATRA
syndrome (pulmonary infiltrates, respiratory distress)28and
the increase of peripheral blast cells. The fact that APL cells
express HGFs ( L - l p , TNFa, and E-6) that are involved
in leukocyte activationz9"'may propose that an abnormal
modulation of these factors by retinoic acid may provoke
these side effects. The data presented here offer a model to
study the mechanisms of induction of these side effects and
identify potential preventive or curative therapies.
Thus, the secretion or absence of secretion of HGF by
APL cells may be determinant for the survival, multiplication, and differentiation capacity of these cells. We suggest
that the resulting expression of growth factors by APL cells
may contribute to the clinical and biologic features of the
disease and that the cause of this expression may be related
to the molecular characteristics of APL. Answering these
questions will be of utmost clinical and scientilic relevance.
ACKNOWLEDGMENT
Wethankthephysiciansparticipatinginthestudy
of all-trans
retinoic acid therapy in M3 patients who sent patient samples to the
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
HGF
3269
EXPRESSION AND ATRA SENSITIVITY IN APL
A
1 2
3 4 1'2'3'
i )@
@-
11-18
1 2 3 4
- -vm
'- -
5
6 7 9
-0rrrw"rm-r
lNFU
l01112 2
5' 7 8 '
11-6
6
2
11-3
813
-nw
1 2 3 4
2 6 813
c
a
GM-CSF
--*m
G-CSF
- - m
2 0813
c
Fig 4. mRNA expression of HGF in APL and non-APL patients. (A) Northern blotting analysis is shown. The size of the transcripts are
normal. Blots were rehybridized with a GAPDH probe for RNA expression normalization. (B) RT-PCR analysis is shown. For IL-10: ethidium
bromide staining of the gel with IL-lp-amplified cDNA. For TNFP, IL-6, 11-3, GM-CSF, and G-CSF Southern blot hybridization with a specific
oligonucleotide probe. Patients 1 to 13, APL patients; patients l ' to 8', non-APL patients. Cases 2,6, 8, and 13 showed partial or no response
to all-trans retinoic acid.
lahoratory for i n vitro differentiation assay: Drs S. Castaigne (Service d'Htmatologie. HKpital Saint-Louis, Paris, France), P. Fenaux
(HApital Claude Huriez, Lille, France). H. Domhret (HBpital SaintLouis, Paris, France), J.M. MiclCa (HBpital Saint-Louis, Paris.
France), A. Delmer (HBpital de I'Hotel-Dieu. Paris, France). F. Duguet (HApital de Purpan, Toulouse, France), J.L. Michaux (Clinique
Saint Luc, Brussels, Belgium). G. Auzanneau(HKpitaldu Val de
Grace. Paris, France), and F. Teillet (HBpital Louis Mourier. Paris.
France). WethankDrs
M. Guenounou andP. Cornillet (HBpital
Rigional et Universitaire, Reims. France) for their collaboration.
REFERENCES
1 . YoungDC,GriffinJD:
Autocrine secretion of GM-CSF in
acute myelohlastic leukemia. Blood 68: I 178. 1986
2. Oster W, Cicco NA, Klein H. Hirano T, Kishimoto T, Lindermann A. Mertelsmann RH, Herrmann F Participation of the cytokines interleukin 6 . tumor necrosis factor alpha, and interleukin-l
beta secreted by acute myelogenous leukemia hlasts in autocrine
and paracrine leukemia growth control. J Clin Invest 84:451. 1989
3. Lopez M,Maroc N. Kerangueven F,Bardin F, Courcoul M,
LavezziC.Birg F. Mannoni P: Coexpression ofthe genes for interleukin-6 and its receptor without apparent involvement in the
proliferation of acute myeloid leukemia cells. Exp Hematol 19:797,
1991
4. Griffin JD, Ramhaldi A, Vellenga E, Young DC, Ostapovicz,
Cannistra SA: Secretion of interleukin-l hy acute myeloblastic leu-
kemia cells in vitro induces endothelial cells to secrete colony stimulating factors. Blood 70: 1218, 1987
S. Ferrari S, Grande A, Manfredini R, Tagliafico E, Zucchini.
Torelli G, Torrelli U: Expression of interleukins I , 3, 6 , stem cell
factor and their receptors in acute leukemia blast cells and in normal
peripheral lymphocytes and monocytes. Eur J Haematol SO: 141,
I993
6 . Russell NH: Autocrine growth factors and leukaemic haemopoiesis. Blood Rev 6149. 1992
7. Geissler K, Tricot G, Leemhuis T, Walker E. Broxmeyer E.
Differentiation-inducing effect of recombinant tumor necrosis factor
a and y-interferon in vitro on blast cells from patients with acute
myeloid leukemia and myeloid blast crisis of chronic myeloid leukemia. Cancer Res 493057. 1989
8. Bennett JM, Catovsky D, Daniel MT. Flandrin G, Galdon
DAG, Gralnick HR. Sultan C: Proposed revised criteria for the classification of the acute myeloid leukemia. A reportofthe FrenchAmerican-British Cooperative Group. Ann Intern Med 103:626,
I976
9. de The H. Lavau C, Marchio A. Chomienne C.Degos L.
Dejean A: The PML-RARa fusion mRNA generated by the t( 15.17)
translocation in acute promyelocytic leukemia encodes a functionally
altered RAR. Cell 66:675. 1991
IO. Dombret H, Scrohohaci ML, Ghorra P, Zini JM, Daniel MT.
Castaigne S, Degos L: Coagulation disorders associated with acute
promyelocytic leukemia: Corrective effect of all-trans retinoic acid
treatment. Leukemia 7:2, 1993
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
3270
I I . Castaigne S, Chomienne C, Daniel MT, Berger R, Fenaux P,
Degos L: All-trans retinoic acid as a differentiation therapy for acute
promyelocytic leukemia. I. Clinical results. Blood 76:1704, 1990
12. Warrell RP, Frankel SR, Miller WH, Scheinberg DA, Itri
LM, Hittelman WN, Vyas R, Andreeff M, Tafuri A, Jakubowski A,
Grabrilove J, Gordon MS, Dmitrovsky E: Differentiation therapy of
acute promyelocytic leukemia with tretinoin (all-trans-retinoic acid).
N Engl J Med 324:1385, 1991
13. Chen Z, Brand NJ, Chen A, Chen SJ, Tong JH, Wang ZY,
Waxman S, Zelent A: Fusion between a novel Kriippel-like zinc
finger gene and the retinoic acid receptor-a locus due to a variant
t( 1 I ;17) translocation associated with acute promyelocytic leukaemia. EMBO J 12:1161, 1993
14. Chomienne C, Ballerini P, Balitrand N, Daniel MT, Fenaux P,
Castaigne S, Degos L: All-trans retinoic acid in acute promyelocytic
leukemias. 11. In vitro studies: Structure function relationship. Blood
76:1710, 1990
IS. Davis LG, Dibner MD, Battey FJ: Guanidine isothiocyanate
preparation of total RNA, in: Basic Methods in Molecular Biology.
New York, NY, Elsevier, 1986. p 130
16. Cordell JL, Falini B, Erber WN, Ghosh AK, Abdulaziz Z,
MacDonald S, Pulford KAF, Stein H, Mason DY: Immunoenzymatic
labeling of monoclonal antibodies using immune complexes of alkaline phosphatase and monoclonal anti-alkaline phosphatase (APAAP
complexes). J Histochem Cytochem 32:219, 1984
17. Stasi R, Venditti A, del Poeta G, Tribalto M, Coppetelli U,
Zaccari G, Papa G. High interleukin-6 plasma levels in acute promyelocytic leukemia. Ann Hematol 64:303, 1992
18. Peck R, Bollag W: Potentiation of retinoid-induced differentiation of HL-60 and U937 cell lines by cytokines. Eur J Cancer 27:53,
1991
19. Santini V, Colombat PH, Delwel R, van Gurp R, Touw I,
Lowenberg B: Induction of granulocytic maturation in acute myeloid
leukemia by G-CSF and retinoic acid. Leuk Res 15:341, 1991
20. Ferrero D, Carless0 N, Pregno P, Gallo E, Pireli A: Selfrenewal inhibition of acute myeloid leukemia clonogenic cells by
biological inducers of differentiation. Leukemia 6: 100, 1992
21. Raza A, Preisler HD, Day R, Yasin Z, Withe M, Lykins J,
Kukla C, Barcos M, Bennett J, Browman G, Goldberg J, Grundwald
H, Larson R, Vardiman J, Vogler R: Direct relationship between
remission duration in acute myeloid leukemia and cell cycle kinetics:
A leukemia intergroup study. Blood 76:2191, 1990
DUBOIS ET AL
22. Bradbury D, Rogers S, Reilly IAG, Kozlowski R, Russell
NH: Role of autocrine and paracrine production of granulocytemacrophage colony-stimulating factor and interleukin-l,B in the autonomous growth of acute myeloblastic leukaemia cells-Studies
using purified CD34-positive cells. Leukemia 6562, 1993
23. Raza A, Yousuf N, Abbas A, Umerani A, Mehdi A, Bokhari
SAJ, Sheikh Y, Qadir K, Freeman J, Masterson M, Miller MA,
Lampkin B, Browman G, Bennett J, Goldberg J , Grunwald H. Larson
R, Vogler R, Preisler H: High expression of transforming growth
factor ,B long cell cycle times and a unique clustering of S-phase
cells in patients with acute promyelocytic leukemia. Blood 79: 1037,
1992
24. Griffin J , Young DC, Herrmann F, Wiper D, Wagner K.
Sabbath KD: Effects of recombinant human GM-CSF on proliferationof
clonogenic cells in acute myeloblastic leukemia. Blood
67: 1448, 1986
25. de Gentille Alban, Schlageter MH, Krawice I, Dombret H,
Najean Y, Chomienne C, Toubert ME: Donntes actuelles sur les
rtcepteurs du G-CSF dans les leuctmiesaiguts myeloides. Bull
Cancer 79: 123, 1992
26. Lotem J, Sachs L: Hematopoietic cytokines inhibit apoptose
induced by transforming growth factor b 1 and cancer chemotherapy
compounds in myeloid leukemic cells. Blood 80:1750, 1992
27. Cozzolino F, Torcia M, Miliani A, Carossino AM, Giordani
R, Cinotti S, Filimberti E, Saccardi R, Bernabei P, Guidi G , Di
Guglielmo R, Pistoia V, Ferrarini M, Nawroth PP, Stem D: Potential
role of interleukin- 1 as the trigger for diffuse intravascular coagulation in acute nonlymphoblastic leukemia. Am J Med 84:240.
1988
28. Frankel S, Weiss M, Warrel RP: A retinoic acid syndrome
in acute promyelocytic leukemia: Reversal by corticosteroids. Blood
78:380a, 1991 (abstr)
29. Sisson SD, Dinarello CA: Interleukin-l, in Zembala M, Asherson GL (eds): Human Monocytes. London, UK, Academic, 1989,
p 183
30. Wong GHW, Goeddel GV: Tumor necrosis factor, in Zembala
M, Asherson GL (eds): Human Monocytes. London, UK, Academic,
1989, p 195
3 1, Hirano T, JSishimoto T: Interleukin-6, in Zembala M, Asherson GL (eds): Human Monocytes. London, UK, Academic, 1989, p
217
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
1994 83: 3264-3270
Hematopoietic growth factor expression and ATRA sensitivity in
acute promyelocytic blast cells
C Dubois, MH Schlageter, A de Gentile, F Guidez, N Balitrand, ME Toubert, I Krawice, P Fenaux,
S Castaigne and Y Najean
Updated information and services can be found at:
http://www.bloodjournal.org/content/83/11/3264.full.html
Articles on similar topics can be found in the following Blood collections
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American
Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.