Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Research Design &
EBM
Ravi Kant
MS, DNB, FAMS, FRCS (Edin), FRCS (Glasg), FRCS
(Engl.), FRCS (Irel.), FACS, FICS, FAIS
Professor of Surgery
1
Science
Intelligent Hypothesis
Experiments & analysis of results prove
that hypothesis is correct.
Replicable universally= Most Important
2
Evidence based medicine:
what it is and what it isn't
Integrating individual clinical
expertise and the best external
evidence
BMJ 1996;312:71-72 (13 January)
Editorial
3
4
Evidence-based health care?
= best evidence
5
Evidence-based health care?
decision-making
6
Type of study
Definition
Observational
Evaluating results of condition or treatment in a defined
population
Retrospective: analyzing past events
Prospective: collecting data contemporaneously
Case-control
Series of patients with a particular disease or condition contrasted
with matched control patients
Cross-sectional
Measurements mode on a single occasion, not looking at whole
population but selecting small similar group & expanding results
Longitudinal
Measurements are taken over a period of time, not looking at
whole population but selecting small similar group & expanding
results
Experimental
Two or more treatments are compared. Allocation to treatment
groups is under the control of the researcher
Randomized
Two randomly allocated treatments
Randomized controlled
Includes control group with no treatment
7
Observational study
Evaluating results of condition or
treatment in a defined population
8
Retrospective:
analyzing past events
9
Prospective:
collecting data
contemporaneously
10
Case-control
Series of patients with a
particular disease or condition
contrasted with matched
control patients
11
Cross-sectional
Measurements mode on a
single occasion, not looking at
whole population but selecting
small similar group &
expanding results
12
Longitudinal
Measurements are taken over a
period of time, not looking at
whole population but selecting
small similar group &
expanding results
13
Experimental
Two or more treatments are
compared. Allocation to
treatment groups is under the
control of the researcher
14
Randomized
Two randomly allocated
treatments
15
Prospective Randomized
controlled
Includes control group with no
treatment
=
GOLD STANDARD
16
Confidence Interval
To p or not to p
17
RR
Relative Risk
18
Hazard ratio/ Odds ratio
19
Systemic Review
reliable
systematic
predefined, explicit methodology
minimize bias
Systemic review+ Statistics= metaanalysis
20
Systemic Review
=?
21
22
Levels of evidence
1= Meta-analyses of Prospective Double
blind randomized controlled trials
2=Prospective Randomized Controlled study/
Meta-analyses of retrospective studies
3= Case series/ Cohort study
4= Case report/ observational
5= Expert opinion
23
Evidence grade: I
I (High): the described effect is
plausible, precisely quantified and not
vulnerable to bias
24
Evidence grade: I
II (Intermediate): the described effect is
plausible but is not quantified precisely or
may be vulnerable to bias
25
Evidence grade : III
III (Low): concerns about plausibility or
vulnerability to bias severely limit the value
of the effect being described and
quantified
26
Strength of recommendation
Definition A
A=Recommendation based on consistent
and good quality patient-oriented evidence
27
Strength of recommendation
Definition B
B=Recommendation based on inconsistent
or limited quality patient-oriented evidence
28
Strength of recommendation
Definition C
C=Recommendation based on consensus,
usual practice, opinion, disease-oriented
evidence or case series for studies of
diagnosis, treatment, prevention, or
screening.
29
Recommendation grade: A
A (Recommendation): there is robust
evidence to recommend a pattern of care
30
Recommendation grade : B
B (Provisional recommendation): on
balance of evidence, a pattern of care is
recommended with caution
31
Recommendation grade : C
C (Consensus opinion): evidence being
inadequate, a pattern of care is
recommended by consensus
32
US Government Agency for
Health Care Policy and Research
(AHCPR):A
A: requires at least one randomized
controlled trial as part of the body of
evidence.
33
US Government Agency for
Health Care Policy and Research
(AHCPR):B
B: requires availability of wellconducted clinical studies but no
randomized controlled trials in the body
of evidence.
34
US Government Agency for
Health Care Policy and Research
(AHCPR):C
C: requires evidence from expert
committee reports or opinions and/ or
clinical experience of respected
authorities. Indicates absence of
directly applicable studies of good
quality
35
36
Grading of evidence
Ia: Systematic review or meta-analysis of
randomized controlled trials
Ib: at least one randomized controlled trial
IIa: at least one well-designed controlled study
without randomization
IIb: at least one well-designed quasi-experimental
study, such as a cohort study
III: well-designed non-experimental descriptive
studies, such as comparative studies, correlation
studies, case–control studies and case series
IV: expert committee reports, opinions and/or
clinical experience of respected authorities
37
Grading of
recommendations
A: based on hierarchy I evidence
B: based on hierarchy II evidence or
extrapolated from hierarchy I evidence
C: based on hierarchy III evidence or
extrapolated from hierarchy I or II evidence
D: directly based on hierarchy IV evidence or
extrapolated from hierarchy I, II or III
evidence
38
39
Research can be Quantitative:
A medical condition is analyzed
systematically using hard, objective end
point such as death or amputation.
40
Research can be Qualitative
Data come from patient narratives, and
the psychosocial impact of the disease
and its treatment are analyzed, for
example narratives of breast cancer.
41
Project design include:
Sample size.
Eliminating bias.
Study protocol.
Ethics.
42
Sample size
An incorrect sample size is probably the
most frequent reason for research to be
invalid.
Never forget that more patients will
need to be randomized than the final
sample size to take into account
patients who die, drop out or are lost to
follow up.
43
Sample size
nX[r(100-r)+s(100-s)]/(r-s)2
44
Type I error
Benefit is perceived when
really there is none (false
positive)
45
Type II error
Benefit is missed because the
study has small numbers (false
negative)
46
Eliminating bias: Single blind
The observers or recorders who do not
know which treatment has been used.
47
Eliminating bias: Double blind
Neither patient nor researcher is aware of
which therapy has been used until after
study has finished, & these are the best
randomized studies.
48
The Cochrane Collaboration
Best evidence
an international not-for-profit and independent
organization,
It produces and disseminates systematic
reviews of healthcare interventions and
promotes the search for evidence in the form
of clinical trials and other studies of
interventions.
The Cochrane Collaboration was founded in
1993 and named after the British
epidemiologist, Archie Cochrane.
49
Current reliable evidencebased medicine resources for
the busy clinician -1
American College of Physicians Journal Club
http://www.acpj.org
American Family Physician
http://www.aafp.org/afp
Bandolier http://www.rj2.ox.ac.uk/bandolie
Clinical Evidence
http://www.clinicalevidence.com
50
Current reliable evidencebased medicine resources for
the busy clinician -2
Cochrane Database of Systematic Reviews
http://www.cochrane.org/reviews/en/
Database of Abstracts of Reviews of Effects (DARE)
http://www.york.ac.uk/inst/crd/crddatabases.htm
Dr. Alper's Useful Links
http://www.myhq.com/public/a/l/alperDynaMed http:
//www.dynamicmedical.com
Family Practitioners Inquiries Network (FPIN) Clinical
Inquiries http://www.fpin.org
FIRSTConsult http://www.firstconsult.comInfoPOEMs
– The Clinical Awareness
Systemhttp://www.infopoems.com
51
Current reliable evidencebased medicine resources for
the busy clinician -3
Institute for Clinical Systems Improvement
(ISCI) http://www.icsi.org/knowledge
Journal of Family Practice
http://www.jfponline.org
SUM Search http://sumsearch.uthscsa.edu
TRIP Database
http://www.tripdatabase.comUpToDate http://
www.uptodate.com
52
Current reliable evidencebased medicine resources for
the busy clinician -4
US National Guideline Clearinghouse
http://www.guidelines.gov
U.S. Preventive Services Task Force (USPSTF)
Recommendations
http://www.ahrq.gov/clinic/uspstfix.htm
53
Current reliable evidencebased medicine resources for
the busy clinician -5
Bandolier
Cochrane Library Database of Systematic Reviews
Completed and on-going health technology assessments from around the world
NHS Economic Evaluation Database (NHS EED)
Critical appraisal of systematic reviews published in the medical literature.
Health Technology Assessment Database (HTA)
Full text systematic reviews of health care interventions, prepared by The Cochrane
Collaboration.
The Database of Abstracts of Reviews of Effects (DARE)
Evidence based thinking about healthcare
Reliable information about the costs as well as the effects of drugs, treatments and
procedures, to inform decisions.
UK Database of Uncertainties about the Effects of Treatments
Publishes those patients' and clinicians' questions about the effects of treatments
which cannot currently be answered reliably by referring to up-to-date systematic
reviews of existing research.
54
Web search-6
Clinical evidence.com
Cochrane.org
Consolidated Standards of Reporting
trials= consort-statement.htm
National Institute for Health & Clinical
excellence (NICE.org.uk
Scottish Intercollegiate Guideline
Network (SIGN) www.sign.ac.uk
55
56
57
Cochrane
58
Bandolier
59
DARE= data base of abstracts
of reviews of effects
60
61
62
Web-based evidencebased medicine courses-1
• http://www.poems.msu.edu/infomastery:
• http://www.hsl.unc.edu/services/tutorials/
ebm/welcome.htm:
• http://www.uic.edu/depts/lib/lhsp/resourc
es/ebm.shtml:.
• http://library.ncahec.net/ebm/pages/index
.htm:
63
Web-based evidencebased medicine courses-2
http://www.urmc.rochester.edu/hslt/miner/re
sources/evidence_based/index.cfm:
http://library.downstate.edu/EBM2/contents.
htm:
http://www.healthsystem.virginia.edu/interne
t/library/collections/ebm/index.cfm:
http://www.cebm.net/:
http://www.sheffield.ac.uk/∼scharr/ir/netting
/:
64
POEMS
Journals with highest frequency of
patient
oriented evidence
that matters (POEMs)
articles that contain
65
Impact factor
average number of citations
to those papers that were
published during the two
preceding years.
=
66
Impact factor
For example, the 2008 impact factor of a
journal would be calculated as follows:
A = the number of times articles published in
2006 and 2007 were cited by indexed journals
during 2008
B = the total number of "citable items" published
in 2006 and 2007. ("Citable items" are usually
articles, reviews, proceedings, or notes; not
editorials or Letters-to-the-Editor.)
2008 impact factor = A/B
67
High-impact journals (those
cited most frequently by others)
Annals of Internal Medicine
British Medical Journal
Journal of the American Medical
Association
Lancet
New England Journal of Medicine
68
A new drug project
69
Preclinical studies
Even animal studies need ethical
clearance in Europe
Efficacy, toxicity and pharmacokinetic
data
70
Phase 0
Human microdosing
Distinctive features of Phase 0 trials include
the administration of single subtherapeutic
doses of the study drug to a small number of
subjects (10 to 15) to gather preliminary data
on the agent's pharmacokinetics (how the
body processes the drug)
and pharmacodynamics (how the drug works
in the body)
71
Phase 1 trial
Dose escalation =Dose ranging
Pharmacovigilance
72
SAD
MAD
Single Ascending Dose studies
Multiple Ascending Dose studies
Crossover study
A short trial designed to investigate any differences in
absorption of the drug by the body, caused by eating before
the drug is given. These studies are usually run as
a crossover study, with volunteers being given two identical
doses of the drug on different occasions; one while fasted,
and one after being fed.
73
Phase II
Larger group
Phase IIA is specifically designed to
assess dosing requirements (how much
drug should be given).
Phase IIB is specifically designed to
study efficacy (how well the drug works
at the prescribed dose(s)).
74
Phase II
Toxixity & efficacy defines go ahead or
not
75
Phase III
Phase III studies are randomized
controlled multicenter trials on large
patient groups (300–3,000 or more
depending upon the disease/medical
condition studied)
76
Phase IV
Phase IV trial is also known as Post
Marketing Surveillance Trial
= Pharmacovigilance
77
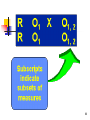
Research Design
It's always easier to explain design
notation through examples than it is to
describe it in words. The figure shows
the design notation for apretest-
posttest (or before-after)
treatment versus comparison
group randomized
78
Research Design
79
80
Experimental study- steps
Animal model
Induce tumor by viral inoculation
Treat tumor by various laser wavelength
Correct wavelength applied in incurable
humans
Regular Clinical approach
81
Pilot study
Somprakas Basu, Bina Ravi & Ravi
Kant: Interstitial laser Hyperthermia, a
New Method in the Management of
Fibroadenoma of the Breast: A Pilot
Study. Lasers in Surgery and Medicine,
1999: Vol. 25: p 148-152.
82
83
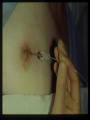
84
Interstitial Laser Hyperthermia
For solid tumors of-
Liver
Pancreas
Lymph nodes
85
86
87
88
89
90
ILH & Pancreas
Kant Ravi, Masters A, Lees WR, Bown
SG: Interstitial Laser Hyperthermia in
Human pancreas tumors: GUT,
supplement 1992. Vol. 33 No 1 W69,
p S18.
91
Lab studies► need
infrastructure
Hedau S, Jain N, Husain SA, Mandal AK, Ray
G, Shahid M, Kant R, Gupta V, Shukla NK,
Deo SS, & Das BC. Novel germ line
mutations in breast cancer susceptibility
genes BRCA1, BRCA2 and p53 gene in
breast cancer patients from India. Breast
Cancer Research Treat 2004 Nov,
88(2):177-86.
92
The Liver: The drains do not
offer any benefit after
elective liver resections.
Marcello Spampinato Hassan Elberm & Colin D
Johnson in Recent Advances in Surgery # 31, by
Irving Taylor & Colin Johnson, The Royal Society
of Medicine Press, 2008 page 189Gurusamy KS, Samraj K, Davidson BR. Routine
abdominal drainage for uncomplicated liver
resections. Cochrane Database Systemic Rev
2007; CD006232
93
GB
The Gall Bladder: The drains do not
offer any benefit after routine
uncomplicated laparoscopic
cholecystectomy.
Marcello Spampinato Hassan Elberm & Colin D
Johnson in Recent Advances in Surgery # 31, by
Irving Taylor & Colin Johnson, The Royal Society
of Medicine Press, 2008 page 196Gurusamy KS, Samraj K, Mullerat P et al.
Routine abdominal drainage for uncomplicated
laparoscopic cholecystectomy. Cochrane
Database Systemic Rev 2007; CD006004
94
The Thyroid: No drain is
required following
thyroidectomy.
Khanna J, Mohil RS, Chintamani, Bhatnagar D, Mittal MK,
Sahoo M, Mehrotra M. Is the routine drainage after
surgery for thyroid necessary? A prospective randomized
clinical study [ISRCTN63623153]. BMC Surg. 2005 May
19; 5:11.
Suslu N, Vural S, Oncel M, Demirca B, Gezen FC, Tuzun B,
Erginel T, Dalkilic G. Is the insertion of drains after
uncomplicated thyroid surgery always necessary? Surg
Today. 2006; 36(3):215-8.
Lee SW, Choi EC, Lee YM et al. Is lack of placement of
drains after thyroidectomy with central neck dissections
safe? A prospective randomized study. Laryngoscope
2006;116:1632-1635
95
The Breast: No drain is
required after conservation
surgery for breast cancer
Stojkovic C, Smeulders MJ, Van der Horst
CM. Wound drainage after plastic and
reconstructive surgery of the breast
(Protocol). Cochrane Database of
Systematic Reviews 2008, Issue 3. Art.
No.: CD007258. DOI:
10.1002/14651858.CD007258.
96
Rectal Surgery: The pelvic
drainage after rectal surgery adds
no benefit.
Urbach DR, Kennedy ED, Cohen MM.
Colon and rectal anastomosis donot
require routine drainage: a systemic
review and meta-analysis. Ann Surg
1999; 229:174-180.
97
Incision by electrocautery heal as
well as incision by knife. No
difference in either postoperative
results or in cosmesis.
Kears SR, Connolly EM, Mc Nally S,
McNamara DA, Deasy J. Randomized
clinical trial of diathermy versus scalpel
incision in elective midline laparotomy.
Br J Surg 2001; 88:41-44.
98
Summary
99
Evidence-Based surgery
Evidence-base study is a move to find out the
best ways of managing patients using clinical
evidence from collected studies.
Collecting published evidence together and
analyzing it often requires review of multiple
randomized trials.
These meta-analysis involve complex
statistical analysis designed to interpret
multiple findings and synthesize the results of
multiple studies.
100
Important advantages of
evidence-based medicine
Has the potential to improve quality of patient care
Identifies and promotes practices that are proven
scientifically to be effective
Identifies practices that are ineffective or harmful
Promotes critical thinking
Requires clinicians to be open-minded
Encourages researchers to focus on evidence and
outcomes that are important to clinicians and
patients
101
Type of study
Definition
Observational
Evaluating results of condition or treatment in a defined
population
Retrospective: analyzing past events
Prospective: collecting data contemporaneously
Case-control
Series of patients with a particular disease or condition contrasted
with matched control patients
Cross-sectional
Measurements mode on a single occasion, not looking at whole
population but selecting small similar group & expanding results
Longitudinal
Measurements are taken over a period of time, not looking at
whole population but selecting small similar group & expanding
results
Experimental
Two or more treatments are compared. Allocation to treatment
groups is under the control of the researcher
Randomized
Two randomly allocated treatments
Randomized controlled
Includes control group with no treatment
102
103
POEMS
patient-oriented evidence that matters
(POEMs)
104
Drains & Evidence
Presented in your book as a chapter
105
Cochrane
106
107