Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
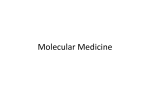
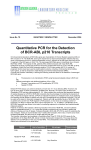
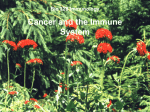
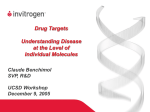
From www.bloodjournal.org by guest on June 17, 2017. For personal use only. BCR-ABL Protein Expression in Peripheral Blood Cells of Chronic Myelogenous Leukemia Patients Undergoing Therapy By Jie Qiang Guo, Jin Ying Lian, Yong Ming Xian, Ming-Sheng Lee, Albert B. Deisseroth, Sanford A. Stass, Richard E. Champlin, Moshe Talpaz, Jean Y.J. Wang, and Ralph B. Arlinghaus Chronic myelogenous leukemia (CML) is a myeloproliferative disorder associated with thePhiladelphia chromosome (Phl) in more than 95% of these patients. The Ph' and the resulting BCR-ABL fused genes are markers for this type of leukemia. In CML, the product of the fused BCR-ABL gene is typically a protein of approximately 2,000 amino acids termed P210 BCR-ABL. We have developed an assay for the BCR-ABL protein involving Western blotting of circulating white blood cells (WBC) with an anti-ABL monoclonal antibody that can detect P210 BCR-ABL and P145 ABL in peripheral blood cells from chronic phase Ph'-positive leukemia patients. This assay was used to analyze the BCR-ABL protein content of circulating WBC from CML patients before and after various treatments. In parallel to changes in percentages of Ph'-positive blood cells as determined by cytogenetic analyses of bone marrow samples, BCR-ABL protein expression in blood cells decreased or increased aspatients entered remission or underwent relapse. Of interest, six Ph'negative CML patients were BCR-ABL protein-positive. All except one had a rearrangement in the major breakpoint cluster region and that patientexpressed P185 BCR-ABLand not P210. Our results indicate that the BCR-ABL Western blotting assayhasclinical applications for both diagnosis and prospective evaluation of Ph'-positive and Ph'-negative CML patients. 0 1994 by The American Society of Hematology. C of CML." Using this assay, we have also been able to detect the P185 form of BCR-ABL protein in white blood cells (WBC) from a patient in chronic phase of CML." Cells from this patient lacked P210 BCR-ABL and lacked a DNA rearrangement in the major breakpoint cluster region (BCR) of the BCR gene. Furthermore, RNA extracted from this patient contained only transcripts with the BCR exon 1 fused to ABL exon 2. We now report results of analyses of CML patients undergoing treatment, either chemotherapy or bone marrow transplantation. Of importance, six patients lacking a detectable Phl at diagnosis were found to express BCR-ABL proteins in their peripheral WBC. HRONIC MYELOGENOUS leukemia (CML) is characterized most frequently by its association with an abnormal chromosome 22, known as the Philadelphia chromosome (Ph').'.' It is estimated that at least 95% of CML cases possess the Ph'.3 In CML this abnormal chromosome fuses a central portion of the BCR gene to the second exon of the ABL gene?5 The protein product produced by this fusion is termed P210 BCR-ABL. In one form the protein contains 927 amino acids encoded by the 5' portion of the BCR gene fused to 1096 amino acids encoded by the ABL gene. A second form fuses 902 amino acids of BCR fused to the same ABL sequences. These two forms of BCR-ABL protein together with alternate splicing patterns result from the fusion of one of two small central exons termed either b2 or b3 to the second ABL exon termed a2. RNA analyses indicate that CML patients can have either form or both, known as b2a2 or b3a2 junctions.6 Another form of the BCR-ABL protein is detected typically in Ph'-positive acute lymphocytic leukemia This form fuses the relatively long first exon of BCR (426 amino acids) to ABL exon 2 (aQ9 This protein termed P190 or P185 BCR-ABL has a higher specific protein kinase activity than P210 BCR-ABL." P185 BCR-ABL also has more neoplastic transformation activity than P210 as measured in cell culture systems." Consistent with its increased potency, P185 BCR-ABL expression is typically butnot always" detected in Phl-positive ALL, which is a subgroup of ALL with a poor p r o g n o s i ~ . ~ . ~ ~ " ~ One important goal in CML is to develop methods to monitor the level of BCR-ABL proteins and their activity during treatment. A first attempt to do this was accomplished several years ago" by using an in vitro kinase to measure the autophosphorylation activity of the activated ABL tyrosine protein kinase present in these BCR-ABL proteins. Unfortunately, although useful for detecting active BCR-ABL tyrosine kinase activity in terminal stage patients (blast crisis), this assay is not useful in monitoring patients in the early stage of this disease known as the chronic or benign stage.15 Lysis of mature blood cells harboring the BCR-ABL protein causes rapid destruction of this and other proteins. A Western blotting assay was developed that allows detection of BCR-ABL protein at early as well as late stages Blood, Vol 83, No 12 (June 15), 1994: pp 3629-3637 MATERIALS AND METHODS Patient samples. Western blotting assays for all patient samples were performed in a BCR-ABL protein screening laboratory within the Department of Molecular Pathology at The University of Texas M.D.Anderson Cancer Center in Houston. Blood samples were obtained from patients as part of a progradproject study sponsored by The National Cancer Institute (NCI). All patients signed an appropriate informed consent form. Peripheral blood samples yielding at least 2 X lo7 WBC were cryopreserved. Ph' percentages were obtained by cytogenetic analysis of bone marrow samples obtained on the same day as the blood sample thus allowing comparison between our results and Ph' chromosome percentage. Cytogenetic analyses From the Department of Molecular Pathology, Divisionof Laboratory Medicine, and the Departments of Hematology, and Clinical Investigation, Houston, T X ; and The Department of Biology, The University of California at San Diego, La Jolla. Submitted July 29, 1993; accepted February 10, 1994. Supported by Grants No. CA49369 and CA16672 from the National Institutes of Health. Address reprint requests to Ralph B. Arlinghaus, PhD, The University of Texas, M.D., Anderson Cancer Center, 1515 Holcombe Blvd, Houston, TX 77030. The publication costsof this article were defrayedin part by page chargepayment. This article must therefore be hereby marked "advertisement" in accordance with 18 U.S.C. section 1734 solely to indicate this fact. 0 1994 by The American Society of Hematology. 0006-4971/94/8312-0015$3.00/0 3629 From www.bloodjournal.org by guest on June 17, 2017. For personal use only. GUO ET AL 3630 were performed by the Division of Laboratory Medicine. CML and ALL were diagnosed according to standard criteria. Normal WBC were donated by volunteers from our laboratory. Cell lines. The K562I9 (positive control), HL-60,2"and KG-12' cell lines (negative controls) were grown inRPM1medium containing 10% fetal bovine serum. K562 cells expressing P210 BCRABL were derived from a CML patient in blast crisis." KG-l cells were derived from an acute myelogenous leukemia patient lacking BCR-ABL proteins. 8E9 antibody. The SE9 antibody was originally isolated by Richardson etIt is a mouse monoclonal antibody directed toward the SH2 region of the mouse gag-ABL protein.ln Processing of patient cells. Peripheral bloodwas collected in heparanized tubes atroom temperature. Bloodwas treated with a mixture of protease inhibitors immediately after receiving the specimen.".'* Red blood cells were removed by two cycles of treatment with NH4CI.I' Of interest, heparanized blood received 4 days after being drawn from the patient gave informative results from both Ph'-positive and negative leukemia patients, but a 1 to 2 day time period is preferred to reduce protein degradation. After removal of red blood cells, intact WBC were treated with diisopropyl fluorophosphate (DIFP), a very potent protease inhibitor as described." The manufacturer's precautions were strictly adhered to when handling DIFP. WBC were stored immediately at -72°C. Western blotting procedure. The BCR-ABL Western blotting test was performed as described,"." butmodified to increase the sensitivity. The more sensitive test involved two fundamental changes. First the enhanced chemiluminescent (ECL) detection system was usedin place ofthe ["'I] protein A detection system. Second, the backgrounds were dramatically reduced by substituting powdered milk for bovine serum albumin (BSA) in our blocking solutions. The detailed procedure is as follows: Western blotting was performed withan anti-ABL (8E9) monoclonal antibody as described previously. Briefly, frozen WBC were lysed in boiling sodium dodecyl sulfate (SDS) sample buffer for 5 to 7 minutes, and the lysate was clarified by centrifugation. Aliquots of the extracts corresponding to IO' cells were applied to each gel lane. Samples were electrophoresed through 6.5% polyacrylamide gels, the gels were electroblotted at 4°C overnight and transferred to lmmobilon P filters (Millipore, Bedford, MA). The ECL Western blotting detection system was used to probe for BCR-ABL protein according to themanufacturer's protocol (Amersham, Arlington Heights, IL). Filters were preblocked by washing with 10% non-fatmilk (NFM) in Tris-buffered saline-Tween 20 (TBS-T) buffer (20 mmol/L Tris base, 137 mmol/L NaCI, 0.0038 N HCI) for 2 hours and then incubated with 1:15,OOO to 20,000 dilution of SE9 in5% NFM TBS-T buffer overnight at room temperature. The filters were then incubated with a 1:3,000 to3,500 dilution of horseradish peroxidase (HRP)-labeled sheep anti-mouse IgG (Amersham, Cat. No. NA 9310) for 2 hours. The filters were mixed with ECL reagents and exposed to X-ray film for I to 10 minutes. Where indicated, the intensities of P210 BCR-ABL, the lower molecular weight BCR-ABL proteins, and P145 ABL within appropriate autoradiograms were scanned with a soft laser scanning densitometer (Zeineh Biomed Instruments, Inc. Fullerton, CA). Southern blotting and polymerase chain reaction (PCR) assays. Sample DNA was extracted, digested with restriction enzymes, separated on agarose gels, blotted on to nylon filters, and probed with a universal BCR probe (UBCR) (Transprobe-l); Oncogene Sciences, Manhasset, NY) and a 3' probe (human BCR DNA Probe-l, Oncogene Sciences), as described." PCR analyses was performed as described." RESULTS Increased sensitivity of the ECL detection system. After a number of unsuccessful attempts to improve the sensitivity A 1 2 3 4 5 6 7 8 9 101112 P2 10- -200 P145- 0 " ' " " " " 0 100 200 300 400 500 800 700 800 900 1000 K582 C E U NUMBER C 0-35 c 50.051 / ow. 0 m ' 10 I 20 I 30 40 50 80 K582 CELL NUMBER (x10 -3 ) Fig 1. ECL Western blotting procedure for detection ofBCR-ABL proteins. (A) Various mixtures of cell extracts from K562 cells and KG-l cells were analyzed.Each lane was loaded with cell extract from 10' cells. The amount of K562 + KG-l cells used in each lane is as follows: lane 1, 1 x 10'K562 cells; lane 2, 5 x lo5 K562 cells + 5 x lo5 KG-l cells; lane 3,2.5 x lo5 K562 cells + 7.5 x 10'KG-l cells; lane 4, 1.2 x lo5; lane 5, 6 x lo'; lane 6, 3 x lo'; lane 7, 1.5 x lo'; lane 8, 7 x 10'; lane 9, 3.5 x 10'; lane 10, 1.7 x 10'; lane 11, 8.5 x 10': lane 12, 1 x 10' KG-l cells. The samples were analyzed on 6.5% gel, molecular weight marker were included. Exposuretime: 8 minutes. BCR-ABL/ABL protein ratios were plotted versus the number of K562 cells ranging from 6 x 10' to 1 x 10' cells in a mixture with KG-l cells, totaling 1 x 10' cells (B) and 0 to 6 x 10'K562 cells IC). of the test by various methods, we found that theECL system could improve the sensitivity more than 100-fold. A typical example is shown in Fig 1A. In this experiment, increasing concentrations of K562 cells were added to KG-I cells so From www.bloodjournal.org by guest on June 17, 2017. For personal use only. BCR-ABL PROTEIN EXPRESSION INCML 3631 PATIENTS 1 2 3 4 5 6 7 8 9101112 P210P145- -200 2 " W -95 Fig 2. Sensitivity of the ECL Western blotting procedure for BCR-ABL protein with extracts from two chronic phase CML patients. Mixtures of cell extracts of 100% Ph'-positive chronic phase CML samples (patients J.S. and 0,s.)mixed with normalWBCs. Each lane was loaded with extract from lo' cells. Amount of CML cell + normal WBC in each lane is as follows: lane 1, 1 x lo' CML cells; lane 2, 5 x 10' CML cells + 5 x 10' normal cells; lane 3, 2.5 x 10' CML cells + 7.5 x 10' normal cells; lane 4, 1.25 x 10' CML cells; lane 5,6 x lo'; lane 6,3 x lo'; lane 7,1.5 x lo5;lane 8, 7 x lo'; lane 9, 3.7 x lo'; lane 10, 1.8 x lo'; lane 11,9 x 10'; lane 12,l x 10' normal WBCs. The samples were analyzed on 6.5% gel, molecular weight markers were included. Exposure time: 12 minutes. 1 2 3 4 5 6 7 8 9 1 0 1 1 12 1 P210P145- that in all cases the total number of cells was kept constant at IO'. The results show that approximately 2,000 to 3.000 K562 cells gave a detectable BCR-ABL signal in a mixture of 10" KG-l cells (ie, 0.3%) (Fig IA, lanes 9 and 10). About 3.000 K562 cells could also be detected in a mixture of 10 million KG-l cells (results not shown). A plot of the BCRABL protein response versus the number of K562 cells demonstrated that at either low or high concentrations. the relationship in this more sensitive assay was linear (Figs I B and C) and very significant:Fig IB, r = 0.99. P < 0.01: and Fig IC. r = 0.98. P < 0.01. In these experiments to account for possible differences in cell number and blotting technique (ie, band intensity). the ratios of BCR-ABL to ABL proteins were plotted versus the K562 cell number. Similar results were obtained with mixtures of WBC from CMLchronic phasepatients that were 100% Ph'-positive when mixed with normal WBC (Fig 2). These results clearly showed that with cells from one patient (J.S.).as few as I .8 X IO4 scored positive for BCR-ABL protein expression (Fig 2, lane IO). In other studies, there was a positive correlation between the ratio of BCR-ABL to ABL proteins in the peripheral blood sampleand the percentage of Phi-positive cells in the bone marrow (manuscript in prep). BCR-ABL protein e.rpression in inclividrtrrlpccticwtsrrrnples. Using the more sensitive assay. Western blot analysis has been performed on more than 250 blood samples from Ph'-positive CML patients at various stages of treatment. many of which had cytogenetic analyses performed on bone marrow cells on the same day. Typically, the relative intensity of the BCR-ABL protein bands compared with the ABL protein band increased or decreased as the Ph' percentage in the marrow increased or decreased. As an example. we show Western blotting data on peripheral WBC together with cytogenetic results of nine such patients a s they underwent therapy. Figure 3A shows blots of a patient (patient M.J.) who was treated with interferon and homoharringtonine simultaneously. PCR analyses indicated that M.J. had a W a 2 BCR-ABL junction. After a brief cytogenetic remission in May of 1992. the patient relapsed because the therapy was stopped due to severe anemia. Thepatient's peripheral blood cells showed amarkedincrease in the BCR-ABLprotein, seen a s early as November of 1992. Patient J.J. (b3/a2) underwent 24 months of homoharringtonine/interferon treatment. Cytogenetic analyseson marrow indicated that diploid cells were predominant in this patient (Nov 1993). The blood sample analyses indicate a low level of BCR-ABL protein throughout the course of treatment. consistent with the cytogenetic results (Fig 3A). Blood samples from twoother patientswereanalyzed during the course of their chemotherapy. Figure 3B shows Western blot resultsfrompatientJ.R. (b3/a2)who was treated with interferon alone. The patient entered into remission a s of January of 1992. as indicated by cytogenetic studies where the bone marrow contained 40% Ph'-positive cells (6 of 15 cells analyzed). BCR-ABL protein expression decreased dramatically at that time and remained undetectable o n two other occasions in 1993. Figure 3B also shows the results of patient S.F.. who was resistant to homo-harringtonine treatment but after changing to interferon. responded well based on BCR-ABL protein analysis in March of 1993. At that time the bone marrow showed 30% of the cells to be Ph'-positive. In September of 1993. the patient lacked detectable BCR-ABL in peripheral blood cells and contained one Ph'-positive metaphase in 90 analyzed. Figure 4 shows BCR-ABL Western blotting results of five patients undergoing bone marrow transplantation receiving From www.bloodjournal.org by guest on June 17, 2017. For personal use only. GUO ET AL 3632 A P.MJ U P.JJ P210- -200 P 145- I"-" 8/8/97 9/5/91 1/3/92 4/24/926/28/9310/5/9212/10/924/1/93 4/29/93 6/1/936/30/93((/30/90 ph' 96% NO 10% 12% ND 10% ND 10% ND ND ND 5% (7/12/91) (1131192) (10/30/92) (11/2/93) B P.JR P210- - -200 - r v U Ph' 112219l 100% 7124191 90% 1!30/92 40% 5/21/93 9/16/93 0% 0% (12/ 13/90) P.SF p210P145- FE 8/7/92 Ph' 100% - -3"m 1018192 1111Ql92 ND -200 3/4/93 9/24/93 50% 30% 5% Fig 3. Changes in BCR-ABL protein expression in peripheral blood cellsfollowing chemotherapy. BCRABL Western blotting analyses and cytogenetic tests were performed on blood and bone marrow samples, respectively, from fourCML patients atvarious stages of treatment with chemotherapy. Western blot analyses were performed ongels in which positive and negative control cell lines were analyzed at withthe along same time molecular weight markers. Dates of BCR-ABLWestern blotting are shown at the bottom of gel lane; results (Ph'%) and dates of bone marrow cytogenetic tests also are shown bot- at the tom of eachlane, if performed. (AI Patient M.J. initially showed partial cytogenetic remission (5/26/92) and thenrelapsed as is evident in the11/12/92sample. Patient J.J. shows decreasing Ph' percentage from 96%t o 10% after undergoing about 20 months HHT/IFN therapy. (B) Patient JR. was treated with interferon. Patient SF.wasinitiallytreatedwith Homo-harringtonine laterand with interferon. OTEIN From www.bloodjournal.org by guest on June 17, 2017. For personal use only. IN CML PATIENTS BCR-ABL A P.TS rALL0 3633 BMT(10/91) B C P.KH P210-3 -- P.AH r ALLO BMT(2/26/93) ,- 4 -200 P210- W Pl45-1 P1452/1/93 2/16/93 4/19/93 9/1/93 0% 0% (114/93) (1/4/93) (5128193) m95%95% P.DS ALLO BMT(10/90) ALLO BMT(4/93) _. P.SH 3 ALLO W(10190) -200 200 ~ pH 3/15/90 8/28/91 100% 3116192 M) 0% 4/8/83 94% 6/7/93) Fig 4. Changes in BCR-ABL protein expression in peripheral blood followingallogeneic bone marrow transplantation. Bloodsamples and bone marrow were taken for BCR-ABL protein analyses and Ph' measurements at various pointsbefore and after transplant. (A) Patient T.S. cytogenetics indicate this patientt o be received an allotransplant in October of 1991. BCR-ABL Western blotting patterns and bone marrow in complete remission through May of1993. (B)Patient K.H. underwent an allotransplant in February of 1993. Of interest, although marrow cytogenetics failedt o detect Ph', low levels of BCR-ABL protein were expressed in this patient. Patient D.S. underwent an allotransplant in April, 1993. (C) Patient A.H. underwent an allotransplant in October of 1990 and had a relapse some time before March of 1992. Patient S.H. underwent an allotransplant in October of 1990 and relapsed before April of 1993. The 3/15/90 assay of patient S.H. was done by the ['=l1 procedure.'' All analyses were performed ona gel with positive and negative control cell lines and molecular weight markers. Dates of BCRABL Western blot analyses are shown at the bottom ofeach gel lane; dates of cytogenetic bone marrow analyses are shown at the bottom of each lane. cells from a healthy donor. Patient T.S. (b2la2) (Fig 4A) had high levels of BCR-ABL proteins in his blood cells before the transplant. After transplant, patient T.S. containqd no detectable BCR-ABL protein as analyzed on six occasions through May of 1993, but was consistently b2la2 positive after transplant except on May 15, 1992 and May 28, 1993, which were negative by PCR. There was an excellent correlation with cytogenetic studies, as the patient was 80% Ph'positive before transplant (16 of 20 cells positive for the Ph'), but lacked the Ph' after transplant. Patient K.H. (b2/ a 2 ) (Fig 4B), although lacking detectable BCR-ABL protein and containing only diploid cells in the marrow shortly after receiving an allotransplant, was weakly positive for BCRABL protein in peripheral blood cells at about 7 months posttransplant. Of importance, cytogenetic analysis failed to detect a Ph'-positive cell in the bone marrow of this patient analyzed on the same day. Of interest, patient K.H. had the b2la2 junction on June 30,1993.Patient D.S. (b2/a2) received an allogeneic bonemarrow transplant in April of 1993. Before that, patient D.S. was strongly BCR-ABL pro- From www.bloodjournal.org by guest on June 17, 2017. For personal use only. GUO ET AL 3634 4 a 0 a9 J a p210- ?$ -- " B3 7 7 a - . . ". a -200 -95 Fig 5. BCR-ABL protein analyses ofperipheral blood cells from CML, ALL, and non-CML disease patients. Peripheral blood cells from patients were harvested as usual and processed for Western blotting. P.7, ALL patient expressing P210 BCR-ABL; P.8, two samples of the same Ph'positive CML patient from peripheral blood (P) or bone marrow (B), respectively; P.9, a Ph'-positive ALL patient expressing P185 BCR-ABL; P.10,chronic lymphomatic leukemia (CLL) patient; P.ll, lymphoma patient; P.12, Down's syndrome; P.13, vasospastic angina. All rasulto obtained with the ECL assay. Every assay contained K562 cells and KG-l cells as positive and negative controls, respectively. tein positive and 100% Ph'-positive (Fig 4B). After the transplant, the patient lacked detectable BCR-ABL proteinin blood cells and no detectable Phl in marrow cells. Patient A.H. (b2/a2) (Fig 4C) underwent an allotransplant in October of 1990. Western blot analyses on three occasions in 1991 did not detect BCR-ABL protein expression in circulating blood cells, although the patient was b21a2 positive on September 13, 1991. After 17 months, this patient relapsed as indicated in the Western blot of March of 1992. This was confirmed by PCR as the patient was b21a2 positive. Subsequent analyses through June of 1993 showed a high level of BCR-ABL protein in blood cells and 100% Ph'-positive marrow cells in samples analyzed on the same day. Patient S.H. (b2la2) (Fig 4C) showed a relapse following an allotransplant some 30 months earlier. This patient had the b2/ a2 junction before and after transplant. BCR-ABL proteins were present in high amounts in his peripheral blood cells at that point and bone marrow cytogenetic analyses showed 18 of 19 cells to be Phl-positive. In summary, all nine patients showed a strong correlation between cytogenetic findings within marrow cells and the level BCR-ABL protein expression in peripheral blood cells. The use of P145 ABL as an internal control clearly showed a diminution of the intensity of the BCR-ABL bands compared with the P145 ABL band as the percentage of Ph'-positive cells decreased. Moreover, as patients underwent cytogenetic relapse, the intensity of BCR-ABL bands showed a corresponding increase relative to the P145 ABL band. Our results show that we can detect the BCR-ABL protein both in peripheral blood samples and bone marrow samples (Fig 5 , patient 8, P & B). Also, our Western blot assay not only detected P210 BCR-ABL in Ph'-positive CML patients, but also detected the BCR-ABL protein in Ph'-positive ALL, either P210 BCR-ABL (patient no. 7) or P185/P190 BCRABL (patient no. 9). Using the more sensitive assay, we also analyzed clinical samples from patients with various other medical problems (Fig 5 ) . Analysis of a large number of blood samples (more than 95 at this point) have not yet detected a false positive, as BCR-ABL proteins were not detected in these samples. Similarly, in more than 231 CML patients (357 blood samples) that were 100% Ph'-positive, we have not had a false negative (manuscript in preparation). BCR-ABL protein detection in Ph'-negative patients. We also analyzed blood samples from six patients that were found to lack a detectable Ph' at diagnosis of disease (originally Ph'-negative) (Fig 6A-C). Western blotting results detected P210 BCR-ABL in five of these patients. Patients J.N. (b2/a2), T.D. (b3/a2), G.S., and J.L. (b2/a2) were BCR-ABL protein-positive in morethan one blood sample taken on different dates (Fig 6A and B). Of interest, blood cells from patient J.M.lacked P210 BCR-ABL expression but contained P185 BCR-ABL (Fig 6C). To verify the presence of a rearranged BCR gene, Southern blotting using a bcr probe was performed on these six patients. The results indicated that five of these BCR-ABL protein-positive patients had a rearrangement in the major bcr site and one patient (J.M.) lacked detectable major bcr rearrangement (germ line) (Table l). The finding that patient J.M. expressed P185 and not P210 BCR-ABL is consistent with the lack of rearrangement in the major bcr region. Presumably, this patient has a break in the first intron of the bcr gene. A seventh patient (P.H.) also diagnosed as Ph'-negative, bcr-positive, was not informative because her blood cells gave only a faint P145 ABL signal (not shown). These findings emphasize the medical utility of the BCR-ABL Western blotting test in Phl associated leukemias. Our results indicate that it is more reliable for diagnosing these leukemias than either classical cytogenetics or the widely used bcr Southern blotting assay. DISCUSSION The results presented here indicate that the level of BCRABLprotein expression in peripheral WBCmimicsthe changes in percentages of Ph'-positive cells in bone marrow cell populations. An improved assay was developed that can detect BCR-ABL protein expression in mixed populations of normal and leukemic cells. BCR-ABL expression can be detected in mixtures of BCR-ABL negative cells containing From www.bloodjournal.org by guest on June 17, 2017. For personal use only. BCR-ABL PROTEIN EXPRESSION IN CML PATIENTS 3635 A P.TD P.JN .L 2/22/93 7120193 P.GS I * 12/7/90 12/28/90 2119/93 81 13/93 B P.JL C P.JB Fig 6. Detection of BCR-ABL protein in peripheral blood cells from Ph'-negative CML patients. (A) Patient J.N., patient T.D., and patient G.S.; (B) patient J.L.; (C) patient J.B. and patient J.M.; samples were analyzed by BCRABL Western blotting.Patient J.M. was assayed by the ['2511 procedure." As in Figs 3 and 4, appropriate positiveand negative controls as well as molecular weight markers were run on the same gel in each case. P.JM K562 as fewas 2,000 to 3,000 K562 (Fig 1A). Moreover, the intensity of the P210 BCR-ABL band is proportional to the number of BCR-ABL cells in the mixture even at very low levels (Fig 1B and C). In studies carried out with 100% Ph'positive chronic phase CML patients, BCR-ABL protein expression can be detected in mixtures of WBC that contain as fewas 0.2% to 0.4% BCR-ABLexpressingleukemiccells (approximately 20,000 to 40,000 leukemic cells in a mixture of 10 million cells) (Fig 2). Thus, in addition to its medical utility for diagnosis, the BCR-ABL protein test performed on peripheral blood provides a convenient way to monitor CML patients as they enter remission or as they undergo relapse. From www.bloodjournal.org by guest on June 17, 2017. For personal use only. 3636 GUO ET AL Table 1. Ph’-Negative CML Patients Express BCR-ABL Patient J.N. T.D. G.S. J.L. J.B. J.M. BCR-ABL Protein bcr Analyses + + i + + i + i + + t* - * No P210 BCR-ABL, but cells express P185 BCR-ABL. These results were obtained by [‘2511proteinA Western blotting assay.” However, it is clear that even with the improved BCRABL test, mixtures of lo7 circulating WBC containing significantly less than lo4 cells leukemic cells will score negative. Moreover, in CML patients who are in remission and have less than 20% Phl-positive bone marrow cells, BCRABL protein detection in circulating blood cells may in some cases fall below the level of detection. Of interest, patients that lack detectable Ph’-positive cells in bone marrow cytogenetic assays may in some cases score positive for BCRABL protein expression in blood cells (Fig 4B, patient K.H.). Thus, cytogenetic bone marrow analyses and BCR-ABL protein expression in circulating blood cells maynot always agree in CML patients with less than 20% Ph’-positive bone marrow cells (manuscript in preparation). Nevertheless, the assay should be quite useful to physicians, as reduction of leukemic cells by more than two logs can be discerned by assay of peripheral WBC from the patient. Although further studies are needed to determine the percentage of false-positives, our experience with more than 350 patients with various types of leukemias, lymphomas, and other diseases shows a perfect correlation between diagnosis of CML and BCR-ABL protein expression (manuscript in preparation). Studies of nine CML patients at various stages of treatment andremission andor relapse showed a clear correlation between the patients cytogenetic analyses for the Ph’ in marrow cells and BCR-ABL protein levels in circulating WBC. Examples of these types of analyses are shown in Figs 3 and 4. The BCR-ABL Western blot test was also shown to detect both forms of BCR-ABL proteins, either P210 or P185 BCR-ABL, in Phl-positive ALL patients (Fig 5). A study is underway to establish firmly the test’s usefulness for diagnosing Ph’-positive ALL (H. Kantarjian, J.Q. Guo, and Arlinghaus, in prep). Also of importance, analysis of blood samples from six patients with a history of being Phl-negative revealed that they were BCR-ABL protein-positive despite being Ph’-negative (Table 1, Fig 6). One of these patients lacking the Phl was also bcr negative, whereas the other five were bcr positive. Of interest, this patient expressed P185 BCR-ABL and not P210 BCR-ABL, suggesting the presence of a BCR exon 1: ab1 2 junction. A similar phenotype has been previously reported by us in a chronic phase CML patient.” Further studies are in progress on cells from this Ph’-negative patient to identify the type of junction. Considering the 100%correlation with the presence of the Phl in newly diagnosed CML patients and the lack of fdsepositives in patients with other diseases (manuscript in prep- aration), the BCR-ABL Western blotting assay has value as a relatively easy means of assessing whether or not patients with leukocytosis andor myeloproliferative syndrome have Ph’-positive leukemia. The sensitivity of the BCR-ABL Western blotting assay does not compare with that of the polymerase chain reaction (PCR) methodology, as indicated by comparing PCR results with BCR-ABL Western blotting data on patients T.S., A.H., and S.H. (Fig 4). However, the detection of the BCR-ABL gene product in peripheral blood cells has importance based on two considerations. First, it indicates that the patient’s cells are expressing the BCR-ABL gene product (which may or may not be kinase active). Second, detection of leukemic cells in the peripheral blood indicates that the leukemic clone is actively dividing. Further, studies are needed to determine whether low levels of detectable BCR-ABL protein in circulating blood cells has clinical prognostic significance in patients who are in remission. ACKNOWLEDGMENT RBA is the recipient of the Hubert L. Stringer Chair in Cancer Research. The ABL monoclonal antibody was either produced in tissue culture or by production of ascites in mice maintained in facilities approved by the American Association for Accreditation of Laboratory Animal Care, and in accordance with current United States Department of Agriculture, Department of Health and Human Services, and National Institutes of Health Regulations and Standards. We thank Leslie Calvert for obtaining patient samples and providing patient information, Dr Hagop Kantarjian for helpful comments, and Tammy Trlicek for assistance in manuscript preparation. REFERENCES 1. Nowell PC, Hungerford DA: A minute chromosome in human chronic granulocytic leukemia. Science 132:1497, 1960 2. Rowley JD:A new consistent chromosomal abnormality in chronic myelogenous leukemia identified by quinacrine fluorescence and Giemsa staining. Nature 243:290, 1973 3. Dreazen 0, Klisak I, Jones G, Ho WG, Sparkes RS, Gale RP: Multiple molecular abnormalities in Ph’ chromosome positive acute lymphoblastic leukaemia. Br J Haematol 67:319, 1987 4. Lifshitz B, Fainstein E, Marcelle C, Shtivelman E, Amson R, Gale RP, Canaani E: bcr genes and transcripts. Oncogene 2113, 1987 5 . Shtivelman E, Lifshitz B, Gale RP, Roe BA, Canaani E: Alternative splicing of RNAs transcribed from the human ABL gene and from the BCR-ABL fused gene. Cell 47:277, 1986 6. Shtivelman E, Gale RP, Dreazen 0, Berrebi A, Zaizov R, Kubonishi I, Miyoshi I, Canaani E: BCR-ABL RNA in patients with chronic myelogenous leukemia. Blood 69:971, 1987 7. Hermans A, Heisterkamp N, von Lindern M, vanBaal S, Meijer D, van der Plas D, Wiedemann LM, Groffen J, Bootsma D, Grosveld G: Unique fusion of bcr and c-ab1 genes in Philadelphia chromosome positive acute lymphoblastic leukemia. Cell 5 1:33, 1987 8. Clark SS, McLaughlin J, Timmons M, Pendergast AM, BenNeriah Y, Dow LW, Crist W, Rovera G, Smith SD, Witte ON: Expression of a distinctive BCR-ABL oncogene in Phl-positive acute lymphocytic leukemia (ALL). Science 239:775, 1988 9. Hooberman AL, Carrino JJ, Leibowitz D, Rowley JD, Le Beau MM, Arlin ZA, Westbrook CA: Unexpected heterogeneity of BCRABL fusion mRNA detected by polymerase chain reaction in Philadelphia chromosome-positive acute lymphoblastic leukemia. Proc Natl Acad Sci USA 86:4259, 1989 From www.bloodjournal.org by guest on June 17, 2017. For personal use only. BCR-ABL PROTEINEXPRESSION IN C M L PATIENTS IO. Lug0 TG, Pendergast A-M, Muller A J , Witte ON: Tyrosine kinase activity and transformation potency of BCR-ABL oncogene products. Science 247:1079, 1990 11. Guo JQ, Hirsch-Ginsberg CF, Xian YM, Stass SA, Champlin RE,, Giralt SA, McCredie KB, Campbell ML, Arlinghaus RB: Acute lymphoid leukemia molecular phenotype in a patient with benignphase chronic myelogenous leukemia. Hematol Pathol 7:91, 1993 12. Kurzrock R, Shtalrid M, Romero P, Kloetzer WS, Talpaz M, Trujillo JM, Blick M, Beran M, Gutterman JU: A novel c-ab1 protein in Philadelphia positive acute lymphoblastic leukemia. Nature 325:631, 1987 13. Chan LC, Karhi KK, Rayter SI, Heisterkamp N, Eridani S , Powles R, Lawler SD, Groffen J, Foulkes JG, Greaves M F , Wiedemann LM: A novel ab1 protein expressed in Philadelphia chromosome positive acute lymphoblastic leukaemia. Nature 325:635, 1987 14. Walker LC, Ganesan TS, Dhut S , Gibbons B, Lister TA, Rothbard J, Young BD: Novel chimaeric protein expressed in Philadelphia positive acute lymphoblastic leukaemia. Nature 329:851, 1987 15. Maxwell S , Kurzrock R, Talpaz M, Keating M, Gallick G, Kloetzer W, Arlinghaus RB, Gutterman J: Analysis ofP210k"b' tyrosine protein kinase activity in various subtypes of Philadelphia chromosome-positive cells from chronic myelogenous leukemia patients. Cancer Res 47:1731, 1987 16. Kloetzer W, Kurzrock R, Smith L, Talpaz M, Spiller M, Gutterman J, Arlinghaus RB: The human cellular ab1 gene Droduct in 3637 the chronic myelogenous leukemia cell line K562 has an associated tyrosine protein kinase activity. Virology 140:23O, 1985 17. Konopka JB, Watanabe SM, Witte ON: An alteration of the human c-ab1 protein in K562 leukemia cells unmasks associated tyrosine kinase activity. Cell 37:1035, 1984 18. Guo JQ, Wang JYJ, Arlinghaus RB: Detection of BCR-ABL proteins in blood cells of benign phase chronic myelogenous leukemia patients. Cancer Res 51:3048, 1991 19. Lozzio CB, Lozzio BB: Human chronic myelogenous leukemia cell-line with positive Philadelphia chromosome. Blood 45:321, 1975 20. Collins SJ, Gallo RC, Gallagher RE: Continuous growth and differentiation of human myeloid leukaemic cells in suspension culture. Nature 270:347, 1977 21. Koeffler HP, Golde DW: Acute myelogenous leukemia: A human cell line response to colony stimulating activity. Science 200:1153, 1978 22. Richardson JM, Marla AO, Wang JYJ: Reduction in protein tyrosine phosphorylation during differentiation of human leukemia cell line K562. Cancer Res 47:4066, 1987 23. Lee M-S, LeMaistre A, Kantarjian HM, Talpaz M, Freireich EJ, Trujillo JM, Stass SA: Detection of two alternative BCR-ABL mRNAs and minimal residual disease in Philadelphia chromosomepositive chronic myelogenous leukemia by polymerase chain reaction. Blood 73:2115. 1989 From www.bloodjournal.org by guest on June 17, 2017. For personal use only. 1994 83: 3629-3637 BCR-ABL protein expression in peripheral blood cells of chronic myelogenous leukemia patients undergoing therapy JQ Guo, JY Lian, YM Xian, MS Lee, AB Deisseroth, SA Stass, RE Champlin, M Talpaz, JY Wang and RB Arlinghaus Updated information and services can be found at: http://www.bloodjournal.org/content/83/12/3629.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.