Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Jatene procedure wikipedia , lookup
Heart arrhythmia wikipedia , lookup
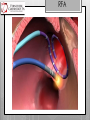
A Fib begets A fib An Overview of AF and Treatment Strategies Jad Skaf, MD 11/12/15 Southern Regional AHEC adheres to ACCME Essential Areas and Policies regarding industry support of continuing medical education. All those in a position to control content have disclosed and there are no unresolved conflicts prior to this program. The following presenters and panelists (and their family members) have no relevant financial disclosures to make: Jad Georges Skaf, MD There will not be discussion of any off-label, experimental, or investigational use of drugs or devices in this presentation This program is not being supported by any commercial funding. Background Atrial fibrillation is the most prevalent cardiac arrhythmia It affects 1% to 2% of the general population with an important increase in incidence with age (10% after age 75) AF has multiple adverse clinical implications The loss of atrial systole and the irregular, fast heart rate contribute to symptoms such as palpitations and reduced exercise tolerance and also predispose to the development of intracardiac thrombus and systemic thromboembolism Background AF can also cause tachycardia-mediated cardiomyopathy or worsening of preexisting heart failure Moreover, AF is known to increase the mortality risk 1.5- to 2-fold and the risk for stroke 5-fold Cost CLASSIFICATION Symptoms ~60% of patients with AF are asymptomatic initially. Mechanisms ANTICOAGULATION Class I LOE C In patients with AF, antithrombotic therapy should be individualized based on shared decision making after discussion of the absolute and relative risks of stroke and bleeding and the patient’s values and preferences Class I LOE B In patients with nonvalvular AF, the CHA2DS2-VASc score is recommended for assessment of stroke risk CHA2DS2-VAsc WARFARIN - ASA Class IIa LOE B For patients with nonvalvular AF with a CHA2DS2-VASc score of 2 or greater and who have end-stage chronic kidney disease (CKD) (creatinine clearance < 15 mL/min) or are on hemodialysis, it is reasonable to prescribe warfarin (INR 2.0 to 3.0) for oral anticoagulation Class I LOE B For patients with AF who have mechanical heart valves, warfarin is recommended, and the target international normalized ratio (INR) intensity (2.0 to 3.0 or 2.5 to 3.5) should be based on the type and location of the prosthesis Class IIb LOE C For patients with nonvalvular AF and a CHA2DS2-VASc score of 1, no antithrombotic therapy or treatment with an oral anticoagulant or aspirin may be considered. MANAGEMENT RATE vs. RHYTHM The decision to adopt a rhythm or rate control strategy is often dictated by the 1) presence of symptoms associated with atrial fibrillation and/or 2) presence of diminutions in left ventricular systolic function thought secondary to the arrhythmia. MANAGEMENT RATE vs. RHYTHM What do we know? Framingham study, 10 year follow-up 5209 patients AF is BAD Benjamin EJ, Wolf PA, D'Agostino RB, et al. Circulation 1998; 98:946. MANAGEMENT RATE vs. RHYTHM Rate Control Which Patients? AFFIRM Trial AFFIRM Baseline Characteristics 4060 patients Age = 69.7 ± 9.0 yrs 39% female > 2 days of AF in 69% CHF class > II in 9% Wyse DG, N Engl J Med. 2002;347(23):1825 AFFIRM Trial Wyse DG, N Engl J Med. 2002;347(23):1825 AFFIRM Trial Wyse DG, N Engl J Med. 2002;347(23):1825 AFFIRM Trial Wyse DG, N Engl J Med. 2002;347(23):1825 RACE Trial Rate Control versus Electrical Cardioversion for Persistent Atrial Fibrillation (RACE) Trial (n=522) Van Gelder, I. et al. N Engl J Med 2002;347:1834-1840 Are we done? Is rate control the answer? LIMITATIONS 1 LIMITATIONS of Trials: AGE Guideline Statement - The mean ages in AFFIRM and RACE were 70 and 68 years, respectively. -The RACE and AFFIRM trials did not address AF in younger, symptomatic patients with little underlying heart disease, in whom restoration of sinus rhythm by cardioversion antiarrhythmic drugs or nonpharmacological interventions still must be considered a useful therapeutic approach. One may conclude from these studies that rate control is a reasonable strategy in elderly patients with minimal symptoms related to AF. ACC/AHA/ESC Guidelines 2014 LIMITATIONS 2 LIMITATIONS of Trials: SYMPTOMS Approximately one-half of patients in AFFIRM who had a detailed history had symptomatic episodes of AF that occurred less often than once per month. Such patients would be expected to derive little symptomatic benefit from rhythm control, and the results may not directly apply to patients with frequent episodes of symptomatic AF LIMITATIONS 3 LIMITATIONS of Trials: ANTICOAGULATION Both trials allowed for cessation of anticoagulant therapy four weeks after documentation of SR, leading to a higher rate of stroke. It has been postulated that continued anticoagulation might have led to a lower mortality in the rhythm control group LIMITATIONS 4 LIMITATIONS of Trials: DRUGS The use of antiarrhythmic drugs in AFFIRM was associated with a significant increase in mortality (HR 1.49), which was due to non-cardiovascular causes, while the presence of SR was associated with a significant reduction in mortality (HR 0.53). A similar benefit from being in sinus rhythm (relative risk 0.44) was noted in the DIAMOND trial that compared dofetilide to placebo in patients with reduced left ventricular systolic function LIMITATIONS LIMITATIONS of Trials: DRUGS One interpretation of these data is that maintenance of SR might be beneficial if there were a safer and more effective approach than current antiarrhythmic drugs: The AFFIRM and RACE data were largely gathered before catheter ablation was common. The potential impact of this procedure (versus chronic antiarrhythmic therapy) remains incompletely explored NEW TRIALS CABANA The Catheter Ablation versus Antiarrhythmic Drug Therapy for Atrial Fibrillation trial is being done to compare drug therapy with catheter ablation in patients with atrial fibrillation. This study will help to decide which treatment approach is best and if under certain circumstances, one therapy is preferred over the other treatment. NEW TRIALS CABANA Estimated Enrollment: 2200 patients Study Start Date: August 2009 Estimated Study Completion Date: June 2018 Estimated Primary Completion Date: December 2017 (Final data collection date for primary outcome measure) https://clinicaltrials.gov/ct2/show/NCT00911508 Anti-Arrhythmics ABLATION % Patients Free of Symptomatic AF 100 80 Ablation… 60 Amiodarone* 40 Propafenone** Sotalol** Hx of Two Failed Drugs*** 20 2 * Roy et al NEJM, 2000 **Antman et.al., JACC 1990 ***Crijns et. al., AJC 1991 4 6 Months 8 10 12 ABLATION Guidelines Paroxysmal AF Class I LOE A PAROXYSMAL REFRACTORY AF catheter ablation is useful for symptomatic paroxysmal AF refractory or intolerant to at least 1 class I or III antiarrhythmic medication when a rhythm-control strategy is desired Class IIa LOE B PAROXYSMAL INITIAL In patients with recurrent symptomatic paroxysmal AF, catheter ablation is a reasonable initial rhythm-control strategy before therapeutic trials of antiarrhythmic drug therapy, after weighing the risks and outcomes of drug and ablation therapy ACC/AHA/ESC Guidelines 2014 ABLATION Guidelines Persistent AF Class IIb LOE B PERSISTENT REFRACTORY AF catheter ablation may be considered for symptomatic long-standing (>12 months) persistent AF refractory or intolerant to at least 1 class I or III antiarrhythmic medication when a rhythmcontrol strategy is desired Class IIb LOE C PERSISTENT INITIAL AF catheter ablation may be considered before initiation of antiarrhythmic drug therapy with a class I or III antiarrhythmic medication for symptomatic persistent AF when a rhythm-control strategy is desired. ACC/AHA/ESC Guidelines 2014 Does not work in AF Hypothesis Atrial fibrillation itself causes progressive electrophysiological and/or structural changes to the atria, which promote the initiation or perpetuation of atrial fibrillation Electrical Remodeling Mechanical Remodeling Diagram showing the localization of the 27 chronically implanted electrodes on the atria. Wijffels M C et al. Circulation. 1995;92:1954-1968 Copyright © American Heart Association, Inc. All rights reserved. Prolongation of the duration of episodes of electrically induced atrial fibrillation (AF) after maintaining AF for respectively 24 hours and 2 weeks. Wijffels M C et al. Circulation. 1995;92:1954-1968 Copyright © American Heart Association, Inc. All rights reserved. Prolongation of the duration of episodes of electrically induced atrial fibrillation (AF) after maintaining AF for respectively 24 hours and 2 weeks. Wijffels M C et al. Circulation. 1995;92:1954-1968 Copyright © American Heart Association, Inc. All rights reserved. AF Begets AF AF causes changes in atrial electrophysiology that promote AF maintenance Wijffels Circulation 1995; 92: 1954-68 Clinical implications Shortening of the atrial refractory might explain the diminished success rate of chemical and electrical cardioversion in patients with longlasting atrial fibrillation Study implicates that the best prevention of atrial fibrillation is to terminate the arrhythmia as soon as possible, thus interrupting the electrophysiological sequelae which will lead to chronic atrial fibrillation Mechanisms Interplay of Trigger and Substrate Induction of AF requires an initiating trigger (usually the pulmonary veins ~80% of times) Perpetuation occurs because triggering activity is sustained or because of the presence of a susceptible atrial substrate Premature atrial ectopy has been shown to be the most frequent trigger for AF Precipitants Observations in patients with dual chamber pacemakers revealed that 48% of AF episodes were triggered by premature atrial beats, 33% were preceded by bradycardia, and 17% were sudden in onset Also, continuous cardiac monitoring in postoperative patients demonstrated that supraventricular premature beats induced AF in 72% to 100% of cases AF Sustenance TRIGGERS Development of AF requires trigger + susceptible substrate APD Goal of ablation: Eliminate triggers and/or alter substrate (may also interrupt innervation from autonomic ganglia) PV Isolation ABLATION RadioFrequency Ablation – RFA Vs. Cryoablation RFA RadioFrequency Ablation – RFA Vs. Cryoablation TRIGGERS PV Origin for Triggers for Initiating Atrial Fibrillation ~ 80 –90% of Triggers Preferential inputs or “breakthroughs” enable non-circumferential disconnection myocardial sleeves Focal Ablation PV Isolation TRIGGERS MRA of LA Success ~ 70-80% paroxysmal ~ 50-70% persistent Multiple Foci from Multiple Veins PVI CRYO CRYO CRYO Contrast injected to verify pulmonary vein ostium occlusion and full contact CRYO Complications of RF ablation: Systemic embolism/CVA (1-2%) PV stenosis < 1-3% Pericardial effusion/cardiac tamponade (1%) Proarrhythmia (intra-atrial reentry tachycardia/left atrial flutter) Atrial-esophageal fistula (very rare) Need for multiple procedures (10 to 30%) to achieve clinical efficacy Complications of Cryo-ablation Systemic embolism/CVA (1-2%) PV stenosis < 1-3% Pericardial effusion/cardiac tamponade (1%) PN palsy 1-3% Atrial-esophageal fistula (very rare) Need for multiple procedures (10 to > 30%) to achieve clinical efficacy end Thankyou You … Thank …