Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
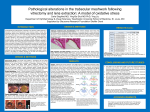
PECULIAR COMPLICATIONS OF VITREORETINA SURGERY IN SUBSAHARAN AFRICA Olufemi Oderinlo FRCSEd ,FWACS, DRCOphth. Consultant Ophthalmologist and Vitreoretina Surgeon EYE FOUNDATION HOSPITAL GROUP • FINANCIAL DISCLOSURE: NO FINANCIAL INTEREST IN MATERIAL PRESENTED INTRODUCTION • Sub-Saharan Africa contains less than 10% of the world’s population, but 20% of the world’s blind. • 1 ophthalmologist per million population • African studies confirm patients with VR diseases present late and with complex pathologies. 25 -40 % of RDs have advanced PVR of > grade C-1 at presentation • Frequent only eye presentations, sickle cell retinopathy, complications of PDR, complications of trauma from regional conflicts • Prolonged surgery and less satisfactory visual outcome Complications of VR surgery in2010 Cataract Elevated IOP Hyphaema Band keratopathy Rubeosis Hyperoleum Subretina fluid Ant staphyloma No post operative complicaction Frequency Percent 11 11.0 8 8.0 2 2.0 2 2.0 2 2.0 1 1.0 1 1.0 1 1.0 72 72.0 Timing of complication Immediate (first 3 days) Early (4 days to 6 weeks) Late (more than 6 weeks) Frequency Percent 1 3.7 11 40.7 15 55.6 Cataract • Incidence btw 50 and 95% • Mechanism unclear : antioxidant function of vitreous, pre-existing cataract, advancing age, light toxicity from the operating microscope, diabetes, use of intraocular gas or silicone oil, and trauma to lens. • duration of vitrectomy does not increase the risk. Elevated IOP/ Glaucoma • Incidence 6 – 8% • Gas : improper mixture, better to do mixture your self, pupil block. Acute elevation • Silicon oil (Chronically elevated IOP was more prevalent in silicone oil eyes than in C3F8 gas eyes) Silicon Study • Ghost cell : intavitreal bevacizumab and vitrectomy. Aim to reduce inflammation and IOP, paracentesis may be helpful • Inflammatory: trabeculitis. • Steroid induced Silicon oil and IOP • Overfill of vitreous cavity • Emulsification (Incidence equal for 1000cs and 5000cs) , Hyperoleum . • Pupil block : absent andoiridectomy in aphakia, closed iridectomy from fibrosis • may require reopening andoiridotomy (Yag) or sugical or oil exchange Cataract + pupil block Silicon oil complications • Changes in refractive status :4 TO 8D change • keratopathy: Punctate epithelial changes, cornea epithelial defect, band keratopathy are all reported • The Silicone Study was the first study to document that the postoperative incidence rates of corneal abnormalities are equivalent between oil and gas. Popovic SS, Sikic J, Pokupec R. Intraocular pressure values following vitrectomy with silicone oil tamponade. Acta Med Croatica. 2005; 59: 143-6. 6. Quintyn JC, Genevois O, Ranty ML, et al. Silicone oil migration in the eyelid after vitrectomy for retinal detachment. Cornea complications • Silicon oil Keratopathy • Light microscopy : increased cellularity and irregularity of collagen fibers of stroma. • Endothelium degeneration with some oil droplets noted • More likely due to barrier effects of silicon than direct toxicity Subretina silicon oil • Rare complication • Can cause redetachment or migrate with time. • Reduces visual function. • Usually requires reoperation, retinotomy, relieve residual traction . • Optic chiasmal and brain migration of silicon oil are reported (case reports). Retained subretina PFCL • retina toxicity may occur from retained perflourocarbon liquids as well as scotomata and elevated intraocular pressures • If very small bubble may be ignored but large bubbles shoud be removed. Hemorrhage • • • • Vitreous Retina Suprachoroidal Hyphema Inflammation • Severe inflammation is rare • Excessive retinopexy esp. cryo, repeat surgery. • Periocular and systemic steroids Endophthalmitis • An incidence of between 0.023% and 0.039% is reported, with staphylococcus aureus more often involved . • A recent large series study reported no difference in incidence of End. after 20G and 23G vitrectomy. Parolini B, Romanelli F, Prigione G, Pertile G. Incidence of endophthalmitis in a large series of 23gague and 20-gague transconjuntival pars plana vitrectomy. Graefes Arch Clin Exp Ophthalmol. 2009;247:895–8. [PubMed] Endophthalmitis • Outcomes are usually poor with greater than 67% having NPL vision. • organisms other than coagulase-negative staphylococci tend to have poor visual prognosis. • EVS results used as guide only • Systemic antibiotics (fourth generation flouroquinolones ), Intravitreal antibiotics (vancomycin, ceftazidime, amikacin) silicon oil exchange. • intravitreal quinupristin/dalfopristin Q/D( recently developed streptogramin antibiotic in 3/7 combination ratio) Am J Ophthalmol. 2004 Nov;138(5):799-802. Endophthalmitis after pars plana vitrectomy: Incidence, causative organisms, and visual acuity outcomes. Eifrig CW, Scott IU, Flynn HW Jr, Smiddy WE, Newton J Iatrogenic retina breaks • Incidence 1-2% • Peeling highly adherent ERM, PVR membranes • Insertion and removal of instruments from the eye can cause peripheral retina breaks. • Maximize use of each instrument before removal • Remove peripheral vitreous as much as possible before instruments Wound leaks and hypotony • Advent of small gauge vitrectomy raised some concern about wound leaks Avoiding complications such as wound leak, hypotony, choroidal detachment and endophthalmitis through optimal surgical technique is critical. Proper wound construction and closure are both necessary to ensure tight self-sealing wounds. • Partial or complete air-fluid exchange, thorough peripheral vitrectomy, and subconjunctival antibiotics are supplemental steps that may also help ensure successful surgical outcomes • Other factors that contribute to wound leakage, such as increased surgical duration and nonmacular diagnosis, may be indirect measurements of extensive trocar rotation, causing wound leakage . CHRONIC HYPOTONY • Chronic hypotony was more prevalent in C3F8 gas eyes than in silicone oil eyes. (The silicon study) • ? Retinectomy Retina toxicity • from ICG, Aminoglycosides and fiberoptic light are reported • Phototoxic lesions caused by the endoilluminator are similar to lesions caused by the operating microscope but are usually larger in size and have less well-delineated borders. • The wavelength of light used, the power of the light source and the duration of use determine the amount of ocular damage in phototoxicity. Aminoglycoside toxicity • Can cause acute, toxic ischaemic retinopathy • Severe retina vasc occlusion and optic neuropathy. • Prevention is crucial. Scleral buckle • Retina hemorrhage from drainage of subretina fluid. • Drainage safer on both sides of horizontal recti and highest level of subretina fluid. Extrusion of buckle • Incidence 3.5 to 24% with silicon sponge • Incidence0.6 to 1.2% with solid silicon Anisometropia • Increase in axial length • Lens can become thicker and displaced anteriorly • 2 – 3 D myopic shift • Cornea steepening leading to astigmatism Strabismus • Incidence 3 – 30% • Exotropia, esotropia, hypertropia and cyclotorsional changes • Many times removal of buckle does not resolve deviation • MRI of orbit useful • Squint surgery may be required • Generally complication rates after vitreoretina surgery is low and most can be prevented by paying attention to detail and being meticulous. THANK YOU REFERENCES • Foos RY, Simons KB, Wheeler NC. Comparison of lesions predisposing to rhegmatogenous retinal detachment by race of subjects. Am J Ophthalmol 1983; 96: 644–649 • D Yorston and S Jalali .Retinal detachment in developing countries Eye (2002) 16, 353–358. doi: 10.1038/sj.eye.6700188 • Lin, Albert L B; Ghate, Deepta A ; Robertson, Zachary M ; O'sullivan, Patrick Sean ; May, Warren L ; Chen, Ching-Jygh Factors Affecting Wound Leakage in 23-Gauge Sutureless Pars Plana Vitrectomy Retina: June 2011 - Volume 31 - Issue 6 - pp 1101-1108