Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
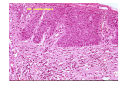
Vulval problems in the post menopausal years Dr. Sallie Neill MB ChB FRCP St John’s Dermatology Unit St Thomas’ Hospital London June 7th 2008 Mucous membrane or skin ? Problems Irritant eczema \ non scarring Psoriasis / Lichen sclerosus \ Scarring Lichen planus Malignancy Pain syndromes - vulvodynia / SCC, verrucous Ca, EMP and vulval intraepithelial neoplasia Rx Soap substitute Barriers Topical steroid Topical local anaesthetic Topical immune modulating cream “Control versus Cure” Eczema Irritant Contact / \ Allergic Rx Contact eczema Avoidance of irritants Soap substitute Mild steroid Daily barrier ointments e.g. zinc,metanium Patch test if ? Allergic CD Psoriasis Flexural Pruritus and burning. Intolerance to irritants Other sites flexures, scalp, auditory canals, nails, knees and elbows Eczema and psoriasis Difficult to distinguish Look for evidence at other sites FH Eczema or psoriasis Irritants. Bubble bath, shampoo, swimming Continent? Vaginal discharge? Rx soap substitute Barriers Mild to mod potent steroid ?pimecrolimus Scarring dermatoses Lichen sclerosus Lichen planus Mucous membrane pemphigoid Clinical Lichen sclerosus o Atrophy Wrinkled skin Ecchymosis o Scarring o Mucosal sparing Loss of architecture No vaginal lesions o Predilection for anogenital skin o Extragenital lesions 1 in 10 o Koebnerises Lichen sclerosus in the older woman Treatment Ultra potent topical steroid Dermovate Once a day Month 1 Daily Month 2 Alt days Month 3 Twice a week Then as required and see the patient than Complications Scarring Malignancy Sexual Still symptomatic but disease quiescent Another agenda? Psychosexual → Psychosexual therapist Lichen planus Treatment Vulval disease Potent topical steroid ? Drug induced Vaginal lichen planus Divide adhesions/EUA Prednisolone suppositories Colifoam Dilators Vaseline petroleum jelly 5% lidocaine is touch sensitive Complications Scarring Malignancy Sexual Safe steroid use frequency once a day amount Finger tip 30gm in 3/12 initially 6/12 maintenance wrong place Topical steroid problems Steroid ointment not used Ultrapotent steroid reactivates viral infection or masks tinea Contact allergy Inappropriate use frequency amount wrong place wrong indication Steroid ointment not used Fear of steroid Package insert Physical inability Unaware of anatomy Symptoms worsen Rx EMP Imiquimod Immune response modifier cytokine activation INF α + IL12 → INF γ TNF α ↑ TH1 response cytotoxic T cells Type IV Vulval intraepithelial neoplasia VIN Full thickness atypia VIN undifferentiated Atypia confined to the lower layer VIN differentiated VIN Undifferentiated Verrucous carcinoma Background of lichen sclerosus Missed on small biopsies Rx ? Role of acetretin Wide local excision Vulvodynia or vulval dysaesthesia Definition no visible or inducible explanation for sensation of pain or itch. Soap substitute Ung emulsificans Few preservatives ÈIrritancy ‘stingers’ No detergents Local anaesthetic 5% lignocaine oint Cheap Contact dermatitis rare Amitriptyline Not for depression Side effects a problem start 10mg Need 50mg or more Unresponsive 90mg . Try alt RX pregabalin, venlafaxine Influences Social Physical Pain Personality Psychological Stress and depression Important role in perpetuation ? in initiation Lifestyle Life events Coping mechanisms www A genital problem 5 questions to ask yourself Is it red or white? Is this scarring or non scarring? Is it affecting skin or mucous membrane? Should I biopsy? Do the symptoms fit the clinical picture? Good dermatology website DermNetNZ Information for docs and patients Information sheets