Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
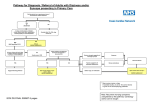
Adult Emergency Nurse Protocol 20XX SYNCOPE Aim: Early identification and treatment of life threatening causes of syncope e.g. arrhythmia, hypovolaemia & escalation of care for patients at risk. Early initiation of treatment / clinical care and symptom management within benchmark time. Assessment Criteria: On assessment the patient may have one or more of the following signs / symptoms: History of faint / brief LOC Diaphoresis Nausea or vomiting Light headedness / weakness Confusion / anxiety Blurry or dim vision Escalation Criteria: Immediate life-threatening presentations that require escalation and referral to a Senior Medical Officer (SMO): Cardiac Arrhythmia Hypotension & tachycardia Suspected Ectopic pregnancy Suspected Pulmonary Embolism Haematemasis Suspected Stroke / TIA Blood in Stool - Malaena Abdominal distension / rigidity Seizures / Postictal Primary Survey: Airway: patency Circulation: perfusion, BP, heart rate, temperature Breathing: resp rate, accessory muscle use, air entry, SpO2. Disability: GCS, pupils, limb strength Notify CNUM and SMO if any of the following red flags is identified from Primary Survey and Between the Flags criteria.1 Airway - at risk Breathing - Respiratory distress Circulation – shock / altered perfusion Partial / full obstruction RR < 5 or >30 /min HR < 40bpm or > 140bpm SpO2 < 90% BP < 90mmHg or > 200 mmHg Disability - decreased conscious level Exposure Capillary return > 2 sec GCS ≤ 14 or any fall in GCS by 2 points Temperature < 35.5°C or > 38.5°C Postural drop > 20mmHg BGL < 3mmol/L or > 20mmol/L History: Presenting complaint Allergies Medications: Anticoagulant Therapy, Anti-hypertensives, Diabetic meds, Analgesics, Inhalers, Chemotherapy, Non-prescription meds, Any recent change to meds Past medical past surgical history relevant Last ate / drank & last menstrual period (LMP) Events and environment leading to presentation i.e. Red flags – palpitations, syncope with exercise, chest pain, palpitations, back pain, haematemesis / melaena before the syncopal episode. Pain Assessment / Score: PQRST (Palliating/ provoking factors, Quality, Region/radiation, Severity, Time onset) Associated signs / symptoms: chest pain, palpitations, low blood pressure, dizziness, lightheadedness, any associated injuries Systems Assessment: Focused cardiac & neurological assessment: Inspection / Palpation / Auscultation Identify location of pain i.e. look for any signs of injury or illness. BP should be checked in the upper extremity bilaterally in supine and standing positions. Pulse rate and rhythm are useful in the diagnosis of arrhythmias and Pulmonary Embolism. Cardiac auscultation may reveal murmurs of aortic stenosis and pulmonary arterial hypertension. Presence of sensory, motor, speech, and vision deficits suggests an underlying neurological problem. Notify CNUM and SMO if any of the following red flags is identified from History or Systems Assessment. Chest pain / palpitations Acute Coronary Syndrome (ACS) Decreased LOC Elderly > 65years Anticoagulant therapy Acute confusion / agitation Severe headache Postural drop > 20mmHg Trauma head / neck Investigations / Diagnostics: Bedside: BGL: If < 3mmol/L or > 20mmol/L notify SMO ECG: look for Arrhythmia , AMI Urinalysis / MSU & βHCG Postural Blood Pressure (3mins > 20mmHg) Laboratory / Radiology: Pathology: Refer to local nurse initiated STOP Quantitative ßHCG if urine positive for same Group and Hold (if bleeding suspected) Blood Cultures (if Temp≥38.5 or ≤35°C) Radiology: Refer to local nurse initiated STOP Nursing Interventions / Management Plan: Syncope – Adult Emergency Nurse Protocol Page 1 Adult Emergency Nurse Protocol 20XX SYNCOPE Resuscitation / Stabilisation: Oxygen therapy & cardiac monitor [as indicated] IV Cannulation (consider large bore i.e. 16-18gauge) IV Fluids: Sodium Chloride 0.9% 1 L IV stat versus over 8 hours (discuss with SMO) Symptomatic Treatment: Antiemetic: as per local nurse initiated standing order Analgesia: as per local nurse initiated standing order IV Fluids: as per local nurse initiated standing order Supportive Treatment: Nil By Mouth (NBM) Monitor vital signs as clinically indicated (BP, HR, T, RR, SpO2) Monitor neurological status GCS hourly Fluid Balance Chart (FBC) Monitor pain assessment / score Practice Tips / Hints: When a patient presents to the emergency department, it is important to correctly differentiate benign neurocardiogenic causes of syncope from life-threatening causes of syncope. A detailed account of the event should be taken from the patient / family or bystander 2 Precipitating factors, signs and symptoms, patient's position at the time of event, duration of syncope, recovery time, and family history are all important points to be considered 2. Red flag symptoms of potentially life-threatening causes of syncope are syncope with exercise, chest pain, palpitations, back pain, haematemesis, and melaena before the syncopal episode. Palpitations before loss of consciousness are a significant predictor of a cardiac cause of syncope 2. Situational syncope with activities including coughing, swallowing, micturition, and defecation suggests that the cause is neurocardiogenic or vasovagal 2. Neurocardiogenic syncope is frequently recurrent and precipitated by fatigue, hot environment, severe pain, starvation, alcohol consumption, emotional or stressful situations, and prolonged standing. The patient is usually in the standing position and complains of symptoms of feeling weak, nausea, diaphoresis, palpitations, and blurring of vision 2. Patients with exertional syncope and positive family history of syncope or sudden cardiac death are at increased risk of sudden death and need to be evaluated further to rule out cardiac causes of syncope such as prolonged QT syndrome 2. Reference: http://bestpractice.bmj.com.acs.hcn.com.au/best-practice/monograph/248/diagnosis/step-by-step.html Further Reading / References: 1. SESLHD Patient with Acute Condition for Escalation (PACE): Management of the Deteriorating Adult and Maternity Inpatient SESLHD/PR283. http://www.seslhd.health.nsw.gov.au/Policies_Procedures_Guidelines/Clinical/Other/SESLHDPR283-PACEMgtOfTheDeterioratingAdultMaternityInpatient.pdf 2. BMJ Best Practice - Assessment of Syncope (CIAP) http://bestpractice.bmj.com.acs.hcn.com.au/bestpractice/monograph/248/diagnosis/step-by-step.html 3. Huff, J.S; Decker W; Quinn J. et al (2007) Clinical Policy: Critical Issues in the Evaluation and Management of Adult Patients Presenting to the Emergency Department with Syncope. Annuals of Emergency Medicine (49) 431-444. http://www.nursingconsult.com/nursing/guidelines/article?guideline_id=189227&parentpage=search Acknowledgements: SESLHD Adult Emergency Nurse Protocols were developed & adapted with permission from: Murphy, M (2007) Emergency Department Toolkits. Westmead Hospital, SWAHS Hodge, A (2011) Emergency Department, Clinical Pathways. Prince of Wales Hospital SESLHD. Revision & Approval History Date Revision No. Syncope – Adult Emergency Nurse Protocol Author and Approval Page 2