Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
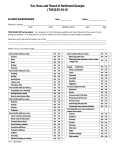
Mike S. Shin, MD Allergy History/Patient Questionnaire Patients Name_________________________________ Sex:_________ Date:___________________________ Age__________ Please answer the following questions as accurately as possible. Your answers will help us determine the cause of your allergy symptoms. Yes No Trouble with your skin? ? Yes No ? Yes No ? During what months do you usually have symptoms? Eczema Which of the following cause or aggravate your symptoms? Hives Indoors All months Outdoors January Trouble with your ears? At home February Popping At work March Itching Morning April Hearing Loss Afternoon May Fluid in Ears At night June Infection/Pain Weather change July Dry weather August Trouble with throat? Windy day September Frequently sore/drainage Hot day October Itching throat/mouth Cold day November Air conditioning December Trouble with eyes? In barns Redness Damp areas Itching Hay, circus Tearing Mowing lawn Puffiness Dusty environment Describe what symptoms bother you High air pollution Trouble with nose? Animas Clear/colorless discharge Cooking odors Thick/colored discharge Smoke Nasal itching/rubbing Soap powder Constant stuffiness Insecticides Sniffles Paint fumes Sneezing Perfumes Mouth breathing or snoring Cosmetic Wave sets Are your symptoms mild? Newspapers Moderate Wool Severe Road dust Present most of the time Milk or milk products Present part of the time Eggs Present rarely Wheat products Interfering with your life Preventing may normal activities? Please specify below Nuts, beans or seeds Chocolate Fish Meat Fruit Trouble with chest? Vegetables Wheezing with colds Alcoholic beverages Wheezing when exposed to dust pollen, animal, etc Cheese, mushrooms Wheeze/cough after exercise Wine Cough Aspirin Chemicals (list) Deep or productive Constant Daytime Nighttime Do you use medication regularly for nasal symptoms What medication? Does it help? Do any of your blood relatives have allergies? Have you ever had skin test for allergies? Do you have allergies? What are you allergic to? Beer Loose Dry/tight When did your condition begin? Drugs (list) Is there anything else about your problem which you think might be important or unusual? onnaire Yes No Do you have a history of: Migraine headaches ? Yes No Do you spend a good deal of time in activities? List: ? Yes No Lower floor Skin disease Main floor Heart disease Upper floor Frequent headaches Wall to wall carpet? Sinus disease Stomach disease Asthma If so, age of carpet? _____________________ Do you take any medications daily or frequently? Nasal polyps Aspirin Emphysema Cortisone Broken nose Laxatives Overactive thyroid Sedatives Bronchitis Birth control pills Nasal surgery Vitamins Underactive thyroid Ointments Hay fever Nose drops/sprays Deviated septum Hormones Hormonal difficulty Others? Specify: Hives Food allergy ? Is your bedroom on: Do you sleep with a pillow? Circle one Dacron Foam Rubber Feather Is your mattress? Circle one Cotton Feather Foam rubber Horse hair Other: Is your heating system? Circle one Oil Gas Electric Wood stove Drug allergy (describe): Other: Other conditions (describe): Smokers in your home? Is delivered by? Circle one Do you smoke? Do you take any medication for Blower any of the previous conidtions? List: Cigarettes #__________________ per day Do you think your occupation has anything to do with your symptoms? Describe: Cigars #______________________per day Radiators Electric panels Other: Filter? Circle one Pipe #_______________________ per day Fiberglass Years smoked?________________________ Describe your occupation: HEPA Permanent electrostatic How often cleaned or changed?__________________ Ducts cleaned? Stopped smoking in year ___________________ When? How often? Do you have animals in your home? List: Any materials used in your occupation that may be something to do with your condition? Describe: Do you have a basement? Do you have a crawl space? Vapor barrier under house? Have you ever had animals in your home? List: Exhaust fan? Circle one Basement At work are your symptoms Kitchen Bath Is vacuum? Circle one Better Do you live in: Worse House? The same Apartment? In the city? Do you use a humidifier? Laundry In the subarbs? Cold mist or steam? Canister Upright Central Vacuum bag type? Circle one Permanent Disposable HEPA Do you have air conditioning? Is you dwelling: At work? New? Family room: At home? 3-10 years old? Wall to wall carpet? Central? 11-25 yearls old? If so, age of carpet?________________ Window unit in bedroom? 25+ years old? Hard surface in family room? water