Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Wittenoom, Western Australia wikipedia , lookup
Mesothelioma wikipedia , lookup
Health impact of asbestos wikipedia , lookup
Asbestos and the law wikipedia , lookup
Organophosphate poisoning wikipedia , lookup
Furthering Asbestos Claims Transparency (FACT) Act of 2015 wikipedia , lookup
Spodden Valley asbestos controversy wikipedia , lookup
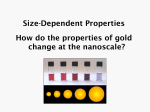
Occupational Medicine 2006;56:312–316 doi:10.1093/occmed/kql053 IN-DEPTH REVIEW ............................................................................................................................................................................................... Nanotechnology and the occupational physician Anthony Seaton ................................................................................................................................................................................... Abstract Nanoparticles differ from the same material at larger scale in chemical and physical properties. Evidence from studies of fibres leads to the conclusion that inhalation of nanotubes could be dangerous and should be regulated. Air pollution research has suggested that particles may be more toxic to cells at the nanoscale. At present the marketing of nanoparticles is advancing more rapidly than research into their safety and toxicology, and one serious inhalation episode has been reported in Germany from apparent use of a nanoproduct. This rapidly developing industry will make an impact on the work of occupational physicians, first in universities and small concerns but later more widely. The future safety of workers and consumers is dependent on research into hazard and risk, an area in which the UK and most other countries are dragging their feet. However, a resource, the Safety of Nanomaterials Interdisciplinary Research Consortium, has been established in the UK to assist those active in this field. ................................................................................................................................................................................... Key words Nanoparticles; nanotubes; occupational exposure. ................................................................................................................................................................................... Introduction It is a commonplace that all new technologies arrive to a fanfare, which is later followed by a reaction as adverse consequences become apparent. More recently, this experience has led to a tendency for proponents of the new to indulge in hyperbole about possible benefits to mankind or the environment while opponents predict dire consequences from its application. The media tend to prefer the dramatic, and publicize both extreme views, leading to the public getting a distorted message depending on the source from which they derive their information. In the case of genetic modification, this led to very restricted application in Europe of a technology that promised many benefits, the media having generally taken the message of those opposed to it. It has to be understood that nobody is disinterested in this process: the media wish to sell their product, the enthusiasts wish to promote their research or product and the opponents wish to publicize their cause and increase their sources of funding. As the preceding papers make clear, nanotechnologies present major economic and academic opportunities wherever they may be developed, and the world’s largest economies are already taking advantage of the possibilities they present. Benefits are likely to come from their exploitation; are we able to predict and prevent adverse consequences? With this in mind, the UK Government Institute of Occupational Medicine, Edinburgh, UK. Correspondence to: Anthony Seaton, Institute of Occupational Medicine, Research Park North, Riccarton, Edinburgh EH14 4AP, UK. E-mail: [email protected] requested the Royal Society and Royal Academy of Engineering [1] to set up a Working Group to consider the opportunities and uncertainties and to advise on what new regulation might be desirable. The Working Group was broadly based, its members ranging from consumer advocates and social scientists to engineers and nanoscientists. In this paper, I consider the main conclusions of the Working Group in relation to hazards and how these might impact on the role of occupational physicians. Hazards and risks of nanomaterials It is of course possible to predict that developments in nanotechnologies, leading to faster communications, greater miniaturization of devices, more effective explosives, more devastating armour-piercing shells and so on, may be exploited to someone’s detriment, but these are risks associated with many new technologies and not confined to those in the nanofield. In considering specific nanotechnological risks, the Working Group concentrated on nanoparticles, in other words discrete pieces of matter that had uniquely new properties because of their scale. It is pertinent to recognize that matter will not be produced at such small sizes unless it has exploitable properties that make it behave differently at that scale. These properties are likely to affect not only its chemistry and physics but also its behaviour in biological systems. Here, it is possible to find some evidence by analogy with what is already known about exposure to more mundane particles in the nanosize range. Two of these are asbestos and combustion-generated nanoparticles. The Author 2006. Published by Oxford University Press on behalf of the Society of Occupational Medicine. All rights reserved. For Permissions, please email: [email protected] A. SEATON: NANOTECHNOLOGY AND THE OCCUPATIONAL PHYSICIAN 313 What can be learned from the asbestos experience? While the risks from asbestos exposure are well known to occupational physicians, the reasons that asbestos causes these diseases are perhaps rather less so. The 2000 people who die each year currently in the UK from mesothelioma do so because of some specific properties of asbestos that also made it the remarkably useful material that it once was. Its many applications relied on its fine fibrous nature and its resistance to degradation— its indestructibility. It is now known that its toxicity depends on the diameter of individual fibres (it can be inhaled to respiratory bronchiole level if 3 mm in diameter), the length of the fibres (they are not removable by macrophages if 15 mm in length) and its resistance to dissolution in the lung. Thus, fibres gain access, cannot be removed and ultimately cause an inflammatory reaction that leads to fibrosis and carcinogenesis [2]. These physical properties, together with another that depends on the chemical reactivity of the fibre’s surface, dictate its hazard, and the risk from inhalation then depends on individual dose. All fibres would be expected to conform to this rule, the differences between them depending on subtle differences in their physicochemical constitution. Thus chrysotile asbestos is generally less likely to cause mesothelioma than the amphiboles as it is more soluble in lung, while the naturally occurring erionite, that caused mesothelioma in villagers in Turkey, is more dangerous because of increased surface reactivity. Carbon and other nanotubes are even finer than asbestos fibres and may be produced at lengths that would make it difficult for them to be removed if inhaled. They are also extremely strong and likely to persist in tissue once introduced. It is predictable that, if inhaled in sufficient quantity, they could cause mesothelioma. As pointed out by Paracelsus, dose is critical. Individuals dying from asbestos diseases usually have millions of fibres per gram of dried lung tissue, the consequence of exposures of several fibres per millilitre (or more realistically, hundreds of fibres per breath or millions of fibres inhaled per day) over several months or years of exposure. It follows from this that tight regulation of a new nanotube industry will be required to prevent exposure not only of production workers but also of those who may be exposed ultimately in the use and disposal of products containing the tubes. At present, the nascent industry is small and the tubes adhere together tightly in clumps; it is predictable that this will not always be the case. The lessons from air pollution research When combustion occurs, nuclear particles of carbon are formed that aggregate together into somewhat larger but still nanometre diameter masses. Interest in the toxicity of such particles arose from the convergence of two streams of research: one, by Oberdörster and his colleagues in Rochester, NY, USA, had been investigating the deposition and clearance of nanometre-sized particles in the lungs of rats [3], while the other, by US epidemiologists, had shown relationships between air pollution and deaths at remarkably low concentrations [4]. In an attempt to explain these latter observations, particularly relating to death from cardiac disease, it was suggested that such very small (primarily carbon) particles could exert toxic effects because of their ability to cause inflammation and secondary effects on blood coagulation when present in very large numbers, even though the total mass inhaled was very small [5]. Subsequent epidemiological work has given limited support to this complex hypothesis, in showing some evidence of changes in inflammatory markers and coagulation factors in relation to air pollution exposure, but as yet little evidence that such effects are due particularly to the nanometre-sized particles. On the other hand, there is now considerably more experimental evidence that nanoparticles are markedly more toxic than the same material at a larger scale [6]. Some of this enhanced toxicity may be explicable in terms of surface contamination—air pollution particles, for example, are usually contaminated by metallic ions and organic molecules—but size alone seems also to be important. Below about 40 nm diameter, particles behave differently not only physically but also possibly in the way they interact with cell membranes [7]; indeed, there is evidence that inhaled nanoparticles may even access the brain, perhaps by neural conduction along olfactory or trigeminal nerves [8]. With respect to lung toxicity, there is sufficient evidence to conclude that for all inhaled particles, a primary determinant of toxicity is total inhaled surface area and that this is increased or decreased by additional properties of the surface, particularly its ability to release free radicals in reaction with tissue [9,10]. The most obvious pathological explanation of such toxicity is inflammation, but it is possible also that, without causing inflammation, lower nanoparticle number concentrations might have direct effects on lung endothelial cells, leading to secondary vascular changes that increase risks of heart attack in both the long and short term [11]. At present these conclusions are based on a combination of experimental work, epidemiology and speculation, and the occupational physician will be aware of some anomalous findings. For example, welders and many other skilled tradespeople are commonly exposed to fumes comprising high number concentrations of nanoparticles, yet they do not seem to have a high death rate from cardiac disease. Some of the highest exposures to particles (and nitrogen dioxide) occur in the kitchen, but few adverse effects have to date been associated with these exposures. There is clearly much still to understand 314 OCCUPATIONAL MEDICINE about nanoparticle exposure. Nevertheless, a warning has been sounded—small particles behave differently and in general are more toxic than the same material in larger size. They thus require special attention from regulators. Where might problems be foreseen with nanoparticles? In the associated commercial exhibition at a scientific meeting on nanotechnology in Japan in 2006, several hundred companies were showing products. It was apparent that most of these, including many nanoparticles, were available to the market. One researcher reported informally that a sample he had been sent had caught fire spontaneously in the mail. Although feeling somewhat uneasy, I originally wrote: ‘‘. . . as far as we know, nobody has yet been harmed by deliberately manufactured nanomaterials.’’ On that very day in April 2006, however, the German Federal Institute for Risk Assessment recalled an aerosol, Magic Nano, marketed for bathroom cleaning and hygiene purposes, the use of which had caused respiratory problems in more than 90 customers, of whom several had been hospitalized with severe pulmonary oedema [12]. It remains unclear as to what this product contained, but it appears that the intention was to create a nanolayer of silica on surfaces. It does not take much imagination to speculate what effect such a nanolayer might have on the alveoli. Occupational physicians will be familiar with the process of assessing risk in relation to determining the intrinsic hazard of materials and the potential exposure of human beings to them. Thus, one might consider the case of nanotubes. In terms of intrinsic hazard, there is a good case for regarding them as likely to be quite toxic but experimental studies to date have been difficult to interpret since the tubes aggregate together and it is difficult to dose rats with them in the way asbestos has been tested. However, the results to date are not reassuring [13]. The problems of their separation give some hope that exposure to individual fibres may not be very great but there are real problems in measuring them in air [14]. For the moment, it would be no bad thing if they were to be treated by those making and using them as though they were asbestos. In terms of potential exposure, it is important to consider the life history of products containing nanotubes. They will undoubtedly be used to strengthen and give new properties to materials. What will happen to these materials? Will they be machined? How will they be disposed of ? At an early stage in development of the technologies, these matters need to be considered in the light of our tragic experience with asbestos. At present, those potentially exposed are mainly in university laboratories and small pilot plants and many of the relevant processes are enclosed. However, it is easy to persuade a laboratory worker to give you a bottle of nanotubes, which look just like soot. I recall a time when it was equally easy to get a sample of crocidolite asbestos. A similar approach may be used in considering any new nanoparticle. How toxic is it? How will it be produced? What will it be used for? How might it be misused? How will it be degraded or disposed of ? Who may be exposed, and to how much, in these different stages of its life history? If, for example, it is to be added as a catalyst to fuel for the worthy purpose of increasing efficiency and reducing CO2 emissions, does it increase or decrease the toxicity of the exhaust emissions? If it is to be added to a cosmetic such as a lipstick or a sunscreen, does it reduce or increase the adverse effects of ultraviolet radiation on the skin? If it is a metallic particle to be used in medical imaging, does the toxicological testing include consideration of the possibility that it might have adverse effects on the endothelium and heart? At present the most likely scenarios of risk from nanoparticles are as follows: • Accidental inhalation episodes from commercial products • Inhalation episodes among production workers/fitters in pilot plants • Insidious inhalation of nanotubes by production workers • Skin damage from careless use of new particles in cosmetics • Explosion/fire in pilot operations • Unexpected reactions to nanomedicines or imaging agents injected intravenously. The role of the occupational physician The training of occupational physicians traditionally includes consideration of diseases regarded as of largely historic interest. But at one time the use of lead and mercury, the hewing of stone and the mining of precious metals and coal were at the very forefront of the technologies of industrialization. We continue to learn hard lessons from unrecognized hazards associated, for example, with PVC production, use of solders in electronics and the introduction of cheap latex for unnecessary use of rubber gloves in the National Health Service. With the introduction of nanotechnologies we have had the opportunity, perhaps uniquely, to make a guess at what problems may lie ahead and take steps to reduce any risks. But where do we start? There are many uncertainties with respect to the toxicity of new nanoparticles and those producing them have an obligation to take seriously the possibility that they may be more dangerous than more mundane materials. Many such people are in universities, where there has traditionally been a rather lax attitude to health and safety. Occupational physicians and safety officers now A. SEATON: NANOTECHNOLOGY AND THE OCCUPATIONAL PHYSICIAN 315 responsible for such institutions should investigate what is going on and what precautions are being taken to protect researchers and workers in spin-off companies. In general, nanoparticles in air behave like gases and people can be protected against them by traditional methods. This includes consideration of what happens during process breakdown or cleaning operations. Their measurement is an issue however. The normal background of particles in an indoor environment may be several thousand nanoparticles per millilitre—how may emissions of manufactured nanoparticles from a process be quantified against this? And what is the best way of measuring them? The small companies involved in manufacture are in particular need of help and such companies rarely have the resources to employ specialist advisors. Here there is a role for government, probably through the Department of Trade & Industry, to ensure that appropriate help is available. If the product is intended for the market-place, expert advice is needed on its toxic potential. How far an occupational physician is responsible for ensuring the safety of a product outside the workplace is questionable, but managers may look to us for general advice on toxicity and anyone aware of such a product made by their employer has an ethical obligation to point out possible unrecognized hazards. It is well to know where to go for advice on these matters. For those physicians involved in advising regulators, there are particular difficulties. It is usual to regulate particulate aerosols by reference to exposure limits, but this is not usually practicable since devices for quantifying nanoparticles in air are not yet readily available and in any case it is not clear what metric would provide the most relevant index of toxic hazard. Where do we go from here? At the time of the Working Group report, it was reasonable to be optimistic that possible risks had been foreseen and that the recommendations made to prevent serious problems would ensure as far as practicable that adverse consequences would be avoided. However, one crucial recommendation was that there was a need for research into metrication, toxicology, workplace exposures to nanoproducts and life cycles of nanoproducts. Another was that the relevant regulators should consider the particular issues arising from nanoproducts in their specialist areas. Unfortunately, the latter depends to some extent on the results of the former, and the UK response has been slower than one would have wished. In particular, no new money for research has been identified. As the German episode illustrates, the market is racing ahead of governmental responses. It will be clear, from this and the preceding papers, that nanoparticles differ from the same material at a larger scale, in chemical, physical and biological properties. They are therefore new chemicals, and need to be regulated as such. At present and in the near future, most will be produced in small quantities, outwith the REACH regulations. But they clearly need specific regulations. We need to understand the toxicology of nanoparticles aimed at the market, the ways to protect workers and customers from adverse effects, how best to measure them in air and other media, how they should be labelled in products and whether disposal is likely to produce any problems for the environment or people. Regulators, industry and academic researchers involved in nanotechnology need a multidisciplinary resource to which they can go for help in these matters, as recommended by the Working Group. At present in the UK, this only exists as an informal, unfunded collaboration, the Safety of Nanomaterials Interdisciplinary Research Consortium, which is however available for help with research and advice (www.snirc.org). Conflicts of interest None declared. References 1. Royal Society and Royal Academy of Engineering. Nanoscience and Nanotechnologies: Opportunities and Uncertainties. London: The Royal Society, 2004. 2. Mossman BT, Bignon J, Corn M, Seaton A, Gee JBL. Asbestos: scientific developments and implications for public policy. Science 1990;247:294–301. 3. Oberdörster G, Ferin J, Lehnert BE. Correlation between particle size, in vivo particle persistence and lung injury. Environ Health Perspect 1994;102(Suppl. 5):173–179. 4. Schwartz J, Morris R. Air pollution and hospital admissions for cardiovascular disease in Detroit, Michigan. Am J Epidemiol 1995;142:23–35. 5. Seaton A, MacNee W, Donaldson K, Godden D. Particulate air pollution and acute health effects. Lancet 1995; 345:176–178. 6. Donaldson K, Stone V, Seaton A, MacNee W. Ambient particles and the cardiovascular system: potential mechanisms. Environ Health Perspect 2001;109(Suppl. 4):523–527. 7. Geiser M, Rothen-Rutishauser B, Kapp N et al. Ultrafine particles cross cellular membranes by non-phagocytic mechanisms in lungs and in cultured cells. Environ Health Perspect 2005;113:1555–1560. 8. Oberdorster G, Sharp Z, Atudorei V et al. Translocation of inhaled ultrafine particles to the brain. Inhal Toxicol 2004;16:537–545. 9. Brown DM, Wilson MR, MacNee W, Stone V, Donaldson K. Size-dependent pro-inflammatory effects of ultrafine polystyrene particles: a role for surface area and oxidative stress in the enhanced activity of ultrafines. Toxicol Appl Pharmacol 2001;175:191–199. 316 OCCUPATIONAL MEDICINE 10. Dick CAJ, Brown D, Donaldson K, Stone V. The role of free radicals in the toxic and inflammatory effects of four different ultrafine particle types. Inhal Toxicol 2003;15: 39–52. 11. Gilmore PS, Morrison ER, Vickers MA et al. The procoagulant effects of environmental particles (PM10). Occup Environ Med 2005;62:164–171. 12. Weiss R. Nanotech product recalled in Germany. Washington Post, 14 April 2006. 13. Lam CW, James JT, McCluskey R, Hunter RL. Pulmonary toxicity of single-wall carbon nanotubes in mice 7 and 90 days after intratracheal instillation. Toxicol Sci 2004; 77:126–134. 14. Maynard AD, Baron PA, Foley M, Shvedova AA, Kisin ER, Castranova V. Exposure to carbon nanotube material: aerosol release during the handling of unrefined single wall carbon nanotube material. J Toxicol Environ Health 2004;67:87–107.