Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
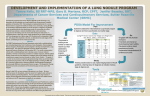
University of Groningen Optimization of nodule management in CT lung cancer screening Heuvelmans, Marjolein IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2015 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Heuvelmans, M. A. (2015). Optimization of nodule management in CT lung cancer screening [Groningen]: University of Groningen Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 17-06-2017 4 Optimization of volume-doubling time cutoff for fast-growing lung nodules in CT lung cancer screening reduces false-positive referrals Marjolein A Heuvelmans Matthijs Oudkerk Geertuida H de Bock Harry J de Koning Xiequan Xie Peter M A van Ooijen Marcel J Greuter Pim A de Jong Harry JM Groen Rozemarijn Vliegenthart Published in European Radiology 2013, vol. 23, no. 7, pp. 1836-1845. 42 4. OPTIMIZATION OF VDT FOR FAST-GROWING NODULES Abstract Objective: To retrospectively investigate whether optimization of volume-doubling time (VDT) cut-off for fast-growing nodules in lung cancer screening can reduce false-positive referrals. Methods: Screening participants of the NELSON study underwent low-dose CT. For indeterminate nodules (volume 50-500 mm3 ), follow-up CT was performed 3 months after baseline. A negative baseline screen resulted in a regular second-round examination, one year later. Subjects referred to a pulmonologist because of a fast-growing (VDT <400 days) solid nodule in the baseline or regular second-round were included in this study. Histology was the reference for diagnosis, or stability on subsequent CTs, confirming benignity. Mean follow-up of non-resected nodules was 4.4 years. Optimization of the false-positive rate was evaluated at maintained sensitivity for lung cancer diagnosis with VDT <400 days as reference. Results: 68 fast-growing nodules were included; 40% were malignant. The optimal VDT cut-off for the 3-month follow-up CT after baseline was 232 days. This cut-off reduced false-positive referrals by 33% (20 versus 30). For the regular second-round, VDTs varied more among malignant nodules, precluding lowering of the VDT cut-off of 400 days. Conclusion: All malignant fast-growing lung nodules referred after the 3-month follow-up CT in the baseline lung cancer screening round had VDT ≤232 days. Lowering the VDT cut-off may reduce false-positive referrals. Key points • • • • • Lung nodules are common in CT lung cancer screening, most being benign. Short-term follow-up CT can identify fast-growing intermediate-size lung nodules. Most fast-growing nodules on short-term follow-up CT still prove to be benign. A new volume-doubling time (VDT) cut-off is proposed for lung screening. The optimized VDT cutoff may decrease false-positive case referrals for lung cancer. Introduction In view of the prospective results of the National Lung Screening Trial (NLST) [1], and the baseline results of other trials [2–6], interest in computed tomography (CT) for lung cancer screening in high-risk individuals is increasing. A drawback of CT screening is the high prevalence of small and intermediate-sized (<10 mm diameter) lung nodules, most of which are benign [7, 8]. The nodule management strategy should allow sensitive and timely diagnosis of malignant nodules. At the same time, patient anxiety, cost and morbidity associated with unnecessary diagnostic procedures for benign nodules should be minimized. In the NLST screening rounds, the rate of positive tests, defined as the presence of one or more nodules of at least 4 mm in diameter, was 24.2% [1]. No less than 96.4% comprised false-positive results [1]. Volume-based nodule management has been suggested to be more accurate, potentially leading to lower false-positive rates [9]. The nodule management strategy of the Dutch-Belgian randomized lung cancer screening trial (Dutch acronym NELSON) is based on volume and volume-doubling time (VDT) assessment [10]. In the baseline screening round, participants with a nodule with volume >500 mm3 were referred for work-up and diagnosis. For intermediate sized nodules (50500 mm3 ) a short-term follow-up CT was performed, to evaluate growth. Because nodules with rapid growth rates are more likely to be malignant [9], nodules with volume >50 mm3 and VDT <400 days were also referred [10]. The second-round CT was based on volume measurements for newly detected nodules and growth evaluation of previously detected nodules (Figure 4.1). This strategy yielded a rather low rate of positive screening tests (2.6% in the baseline screening; 1.8% in the second-round screening) [6], while only 3 of the 7557 screening participants were diagnosed with an interval cancer (NPV 99.7%) [6]. Still, most suspicious lung nodules that resulted in referral to a pulmonologist turned out to be benign (60.4% in the baseline screening; 54.2% in the second-round screening) [6]. We hypothesized that by optimizing the VDT cut-off for fast-growing nodules, the rate of false-positive referrals can be further reduced. Therefore, our objective was to retrospectively evaluate the VDTs of fast-growing solid pulmonary nodules in order to find the optimal VDT cut-off for differentiating benign and malignant nodules in the first two screening rounds of the NELSON trial. Materials and Methods Study population The NELSON multi-center trial was approved by the Dutch Minister of Health and the ethics board at each participating center. All participants provided written informed consent. Participants were current and former smokers, aged 50-75 years, at high risk of lung cancer. Recruitment procedures and selection criteria in the NELSON trial have been published [11]. In this retrospective sub-study, participants with at least two low-dose CT examinations during the baseline round and regular second-round screening in year 2 (April 2004 to April 2007) and a small-to-intermediate-size lung nodule (volume <500 mm3 ) with fast growth (VDT <400 days) either at the short-term follow-up examination after baseline (the extra 44 4. OPTIMIZATION OF VDT FOR FAST-GROWING NODULES CT for nodules of 50-500 mm3 at baseline), or at the regular second round CT one year after baseline (for any nodule <500 mm3 at baseline) were included. Only participants who were subsequently referred to a pulmonologist because of this fast-growing lung nodule and had either a histological diagnosis or a 2-year follow-up period after negative outcome of work-up to confirm benignity were included (Figure 4.1). The reason for including only participants who were referred to a pulmonologist was because diagnosis based on histology was our aim. Work-up was left to the discretion of the pulmonologist. A total of 8,623 lung nodules were detected in the baseline round of the NELSON trail. 210 of those showed fast-growth at the 3-month follow-up CT after baseline or at the regular second-round scan (Figure 4.2). The majority (127 nodules) did not warrant referral to a pulmonologist for a variety of reasons. Of the screening participants that were referred to a pulmonologist (83 nodules), another 15 were excluded since they had less than 2 years follow-up period after a negative outcome of workup. Sixty-eight fast-growing nodules were included. Of these, 27 nodules were malignant. Of the 41 benign nodules, eight (20%) were classified benign based on histology. The mean follow-up time of the other benign nodules was 4.4 years (95% CI, 3.9-4.9 years; range 2.7-5.7 years), showing stable or decreased size over time. In three of the excluded participants who were initially not referred because of a measurement error in the volume, malignancy was confirmed after the third-round examination. Figure 4.1: Overview of the NELSON screening protocol. Nodule management and diagnostic work-up (Figure 4.1) The baseline screening result was positive if any non-calcified pulmonary nodule was larger than 500 mm3 . The result was indeterminate in case of a non-calcified nodule of 50500 mm3 [6, 10]. In the case of smaller non-calcified nodules, the screening was negative. Subjects with an indeterminate result had follow-up CT 3 months after the baseline exam- ination to assess growth. Growth was defined as a volume increase of at least 25% [12]. If a growing lesion had a VDT <400 days, the final baseline result was positive. In case of slower growing lesions, the baseline screening result was negative and the participant was invited for the regular second-round examination in year 2. Figure 4.2: Flow chart of subjects selected with fast-growing pulmonary nodules. VDT = volume-doubling time. At the regular second-round CT, either a nodule was new, and the result was based on nodule size (similar to the baseline examination), or a nodule was pre-existing [10]. For pre-existing lung nodules, the result was based on the VDT. If the VDT was <400 days, the regular second-round screening result was positive [6]. Test positive cases were referred to a pulmonologist for work-up. Work-up, staging, and treatment were standardized according to (inter-)national guidelines [10, 13, 14]. Nodules were classified as benign or malignant based on histological examination. Also, nodules could be classified benign based on stable or decreased size two years after first detection (Figure 4.3) [15, 16]. In the case of diagnosed lung cancer, the participant was treated and was no longer invited for screening examinations; otherwise the regular next-round CT was scheduled. Imaging methods and volumetric analysis Data acquisition and image analysis were reported previously [10]. In brief, low-dose, unenhanced chest CTs were performed using 16-row detector CT systems (Sensation-16, Siemens Medical Systems; Forchheim, Germany; Mx8000 IDT or Brilliance 16P, Philips Medical Systems; Cleveland, OH, USA). Spiral mode with 16x0.75 mm collimation and pitch 1.39-1.5 was used. Depending on the body weight (<50, 50-80, and >80 kg), the 46 4. OPTIMIZATION OF VDT FOR FAST-GROWING NODULES kilovolt-peak settings were 80-90, 120, and 140 kVp, respectively. The milliampere-second values were 20-30 mAs and were adjusted accordingly dependent on the machine used. This corresponds to an effective radiation dose of less than 1.6 mSv. Data sets of the lung were reconstructed at 1.0-mm slice thickness, with a 0.7-mm reconstruction increment. A reconstructed slice thickness of 1.0 mm has been found to be accurate for estimating VDT [17]. Data acquisition and imaging conditions were standard across screening centers and equal for baseline and repeat screening. Digital workstations (Leonardo; Siemens Medical Solutions; Erlangen, Germany) with software for semi-automated three-dimensional (3D) volume measurements (LungCare, version Somaris/5: VA70C-W; Siemens Medical Solutions) were used for nodule volumetric analysis. CT examinations were read twice, by independent readers. Experience for the first readers ranged from none to >20 years. Both second readers had six years of experience in thoracic CT. If the results between first and second reader were discrepant, the readers re-evaluated the examination to reach consensus. If consensus could not be reached, a third, expert thoracic radiologist arbitrated [10]. After a nodule was selected by a radiologist, the system automatically calculated nodule volume. Information was saved in the NELSON Management System, which calculated the percentage volume change and VDT. The VDT was calculated by comparing nodule volume at the latest CT with the volume at the baseline examination as a reference time point. For additional analysis, we also calculated the VDT by comparing nodule volume at the time of the positive screening result with the nodule volume at the latest CT before the positive screening for nodules detected at more than two CTs before referral after the regular second-round examination. Ko’s model for nodule growth Recently, a volumetric model for identification of malignancy in pulmonary nodules in CT lung cancer screening was introduced by Ko et al [18]. We applied this model to evaluate whether the false-positive rate in our screening study could be lowered by using this method. We compared the reduction in false-positive rate found by using Ko’s method, to the reduction found by using our own optimized VDT cut-off. Data analysis Parametric data were expressed as mean and 95% confidence interval (95%-CI), nonparametric data as median and interquartile ranges. The non-parametric Mann-Whitney U test was used for analysis of volume and VDT. In additional analysis, we compared the VDT using as a reference point the nodule volume at first detection or the volume at the latest CT before the examination with a positive screening result, with the Wilcoxon signed-rank test. To identify the optimal VDT cut-off values for differentiating growing benign and malignant pulmonary nodules at 3-month follow-up of the baseline screening round and at the regular second-round examination, the false-positive rate at different VDTs was evaluated, while maintaining 100% sensitivity, with the current cut-off value of VDT <400 days as reference. Statistical analyses were performed using PASW 18 (SPSS, Chicago, IL, USA). Pvalues <0.05 were considered significant. Figure 4.3: Growing benign lesion in a 64-year-old man. Axial computed tomography (CT) (a) shows a nodule (arrow) with a volume of 66.4 mm3 in the right upper lobe. Three months later (b), the nodule volume increased to 83.3 mm3 , the VDT was 342 days and the participant was referred to a pulmonologist. Work-up showed no malignancy. At the regular second-round examination (c) the nodule volume was 86.8 days (VDT 1104 days). In the fourth screening round (d), more than 5 years after referral, the nodule volume was 96.5 mm3 (VDT >10 000 days). The growth curve is shown in (e). Table 4.1: Characteristics of nodules with volume-doubling time <400 days observed during the first two screening rounds, at the moment of referral to pulmonologist due to positive examination. Benign nodules Nodule volume (mm) n (%) 50-500 >500 Total 37 (90) 121 (82, 171) 4 (10) 836 (693, 2207) 41 (100) 124 (84, 206) a Malignant nodules Median volume n (%) (mm3 ) (25th , 75th %a ) P-value Median volume (mm3 ) (25th , 75th %a ) 15 (56) 280 (126, 362) 12 (44) 777 (618, 1201) 27 (100) 486 (227, 774) <0.001 25th % = 25th percentile, 75th % = 75th percentile Results Sixty-eight fast-growing nodules (VDT <400 days) in 61 participants were included (Figure 4.2). Of these, 27 nodules (27 participants) were malignant. Twenty-three men (85%) and four women (15%) had a malignant nodule (mean age at positive examination 63.8 years; 95% CI, 61.6-66.0 years); 24 men (71%) and ten women (29%) had benign nodules (mean age 63.5 years; 95% CI, 61.6-65.4 years). Eighty-two % of the fast-growing nodules was of intermediate size (volume 50-500 mm3 ) at baseline, and 16% was of small size (<50 mm3 ). The remaining 2% (one nodule) was of large size (>500 mm3 ) but was initially diagnosed as non-malignant after workup in the baseline screening round, and returned into the screening regimen. Of the nodules leading 48 4. OPTIMIZATION OF VDT FOR FAST-GROWING NODULES Figure 4.4: Growing malignant lesion in a 54-year-old man. Axial computed tomography (CT) (a) shows a nodule (arrow) with a volume of 146.4 mm3 in the right lower lobe. Three months later (b), the nodule volume increased to 150.6 mm3 (volume-doubling time [VDT] = 2303 days). At the second-year examination, 1 year after baseline CT (c), the nodule volume was 553.8 mm3 . The VDT at that time was 187 days. Work-up revealed a stage IA adenocarcinoma. The growth curve is shown in (d). to referral after the 3-month follow-up CT in the baseline round, malignant nodules (median 250 mm3 ) had a significantly larger baseline volume than benign nodules (median 81 mm3 ; P<0.01). Of the malignant nodules, 52% (14/27) had shifted upward in volume category at the positive screening, compared with 24% (10/41) of the benign nodules. For example, an intermediate-sized pulmonary nodule, 151 mm3 , at the CT before the one with the positive screening result, had grown to a large size, 554 mm3 at the next examination (see Figure 4.4). Nodule characteristics at positive screening CT examination are shown in Table 4.1. No difference was found in VDTs of nodules referred after the regular second-round examination calculated by using volume at first detection or volume of the last examination before the CT with the positive screening result (median VDT 269 versus 237 days; P=NS). Histological Features The 27 lung cancers were histologically classified as follows: 15 (55%) adenocarcinomas, 6 (22%) squamous cell carcinomas, 4 (15%) large cell carcinomas, 1 (4%) small cell lung cancer, and 1 large cell neuroendocrine carcinoma (4%) (Table 4.2). Table 4.2: Histological features and volume-doubling time of malignant nodules per screening round. Moment of referral Histological type n VDT (days) Percentage (median (25th , 75th )a ) 3-month follow-up baseline Adenocarcinoma Squamous cell carcinoma Large cell carcinoma Large cell neuroendocrine carc. Total 4 5 1 36% 45% 9% 110 (63, 208) 118 (84, 187) 24 (-b , -b ) 1 9% 68 (-b , -b ) 11 100% 98 (68, 169) Regular second-round Adenocarcinoma examination Squamous cell carcinoma Large cell carcinoma Small cell lung cancer Total 11 1 3 1 16 213 (185, 327) 165 (-b , -b ) 289 (124, -b ) 84 (-b ,-b ) 205 (165, 318) Total 15 55% 6 22% 4 15% 196 (135, 250) 142 (91, 178) 207 (49, 326) 1 68 (-b , -b ) a b Adenocarcinoma Squamous cell carcinoma Large cell carcinoma Large cell neuroendocrine carc. Small cell lung cancer Total 69% 6% 19% 6% 100% 4% 1 4% 27 100% 84 (-b ,-b ) 198 (122, 264) 25th = 25th percentile, 75th = 75th percentile. Too few nodules available for the calculation. VDTs at Different Time Points of Referral Forty-one participants with 48 nodules were referred after the 3-month follow-up CT in the baseline screening round. Eleven of these were malignant (positive predictive value [PPV], 23%). Twenty participants with 20 fast-growing nodules were referred after the regular second-round examination in year 2, of which 16 were malignant (PPV, 80%) (Table 4.3). Ten of the 16 participants with malignant nodules referred after the regular second-round CT also underwent a 3-month follow-up CT after the baseline examination, showing no fast growth (VDT >400 days). The six remaining malignancies were <50 mm3 at baseline (n = 4), or were initially not considered suspicious based on CT and therefore did not receive a 3-month follow-up examination (n = 2, baseline volumes 57.6 and 117.6 mm3 ). The median VDT for malignant nodules was significantly lower than for benign nodules at the 3-month follow-up CT in the baseline screening round (98 versus 203 days; P=0.013). The difference in median VDT for malignant versus benign nodules at the regular second-round examination did not reach statistical significance (205 versus 291 days; P=NS, Figure 4.5, Table 4.3). 50 4. OPTIMIZATION OF VDT FOR FAST-GROWING NODULES Table 4.3: Nodule volume category at baseline screening and VDT at different moments of referral, with differentiation by tumor nature. Nodule Tumour Moment of volume nature referral (mm3 ) VDT (days) Percentage P N (nodules / (median (25th , a (nodules / value participants) participants)a ) 75th )a ) 3-month follow-up baseline Benign Benign Malignant Benign Malignant 5 32/28 11 37/30 11 100% 74%/72% 26%/28% 77%/73% 23%/27% 173 (112, 284) 204 (132, 264) 98 (68, 169) 203 (133, 262) 98 (68, 169) Benign Malignant Benign Malignant Benign Malignant 3 5 1 11 4 16 37% 63% 8% 92% 20% 80% 293 185 289 213 291 205 <50 50-500 Total Regular <50 secondround 50-500 examination Total (214, (104, (289, (165, (233, (165, -c ) 314) -c ) 327) 353) 318) 0.013 0.12 VDT = volume-doubling time. a When only one number is shown, the number of nodules is equal to the number of participants. b 25th = 25th percentile, 75th = 75th percentile. c Too few nodules available for the calculation. VDT cut-off Based on the VDTs of fast-growing nodules referred after the 3-month follow-up CT in the baseline round, a VDT cut-off of 232 days was determined. Fourteen benign nodules (30% of total benign nodules) in 12 subjects had higher VDTs than 232 days. Two of the 12 subjects however, had another faster-growing benign nodule, so they would still have been referred to a pulmonologist. In total, ten of the 30 participants (33%) with a benign nodule would not have been referred with the optimized VDT cut-off. At the regular second-round examination in year 2, VDTs varied more among the malignant nodules (ranging from 84 to 358 days). VDTs of the four benign nodules referred after the second-year examination ranged from 214 to 373 days. Comparison with Ko’s model When applied to our selection of fast-growing pulmonary nodules, the model introduced by Ko et al. [18] reduced false-positive tests by 4 (9%) and false-positive referrals by only 2 (7%) for the 3-month follow-up CT in the baseline round. In the second-round screening, all benign nodules showed abnormal growth according to this model, leading to false-positive test results. Figure 4.5: Box plots of volume-doubling times of malignant and benign nodules at 3-month follow-up CT in the baseline screening (A) and at the regular second-round screening (B). NS = not significant. Discussion Our results show that lowering the VDT cut-off from 400 to 232 days at the 3-month follow-up CT in the baseline lung cancer screening round led to a third fewer false-positive referrals, at maintained sensitivity for lung cancer diagnosis. This is especially important as the baseline screening was the round with the most fast-growing pulmonary nodules relatively speaking. For the regular second-round examination, the VDT cut-off of 400 days could not be lowered owing to the larger variation in VDTs of malignant nodules. In the NELSON trial, nodule management is based on volume and VDT. The only other lung cancer screening study with volume-based nodule management found a slightly higher false-positive rate at baseline (7.9%) [19]. These false-positive rates are considerably lower than those in other screening trials with diameter measurements [1–4]. In the latter trials, 13.4-28.8% false-positive results were found in the baseline round. Minimizing the false-positive rate remains important, to reduce negative psychological effects [20, 21], unnecessary invasive procedures, radiation exposure from additional CT examinations and cost. Previous research showed more rapid growth rates in new nodules found on repeat rounds. The VDTs of nodules referred after the regular second-round examination in our study were longer than the VDTs of nodules referred after the 3-month follow-up CT in the baseline screening round. This may seem counterintuitive at first glance. However, this finding can be explained by our nodule selection (not new nodules at follow-up examinations, but only nodules already visible at the baseline, prevalence screening). Nodules detected at baseline typically include more slow-growing cancers, compared with nodules first detected after the baseline screening round [22]. In our study, all 20 nodules referred after the regular second-round examination had already been detected at the baseline CT, and 14 also had a 3-month follow-up CT after baseline showing VDT>400 days. Therefore, it makes sense that nodules referred after the regular second-round examination had longer VDTs than nodules referred after the 3-month follow-up CT in the baseline screening. The higher PPV in the second-round examination indicates that the malignancy risk is 52 4. OPTIMIZATION OF VDT FOR FAST-GROWING NODULES considerable for nodules showing increased growth rates after a longer follow-up period. This is in accordance with a previous analysis in the NELSON study, in which growth was found to be an especially important risk factor for malignancy at the second-round screening [14]. Van Klaveren et al showed that the negative predictive value of the baseline CT screening of the NELSON trial, which included nodules with volume <50 mm3 or VDT >400 days, was 99.7% [6]. We excluded nodules with a VDT >400 days to avoid overdiagnosis [23]. A VDT of 500 days is regarded to be the upper limit for malignancy [24, 25]. Potentially it could be valuable to raise the VDT cut-off for CT examinations after the baseline screening round beyond 400 days, to avoid missing lung cancer cases. This was however not the topic of the current study. We recommend further research, with inclusion of nodules with longer VDTs, to determine the optimal VDT cut-off for follow-up CTs after baseline screening. Recently, Ko et al. introduced a nodule growth model, using at least two CT examinations, based on stable nodules [18]. They demonstrated abnormal growth in a handful of histologically proven malignant nodules. When applied to our selection of fast-growing pulmonary nodules, only very small reduction in false-positive referrals was found (7% for the 3-month follow-up CT after baseline, 0% for the regular second-round examination). Ko et al based their model on the study of Lindell et al, which showed no exponential growth pattern in any pulmonary nodule and thereby concluded that VDT may not be suited to pulmonary nodule management. However, Lindell et al used two-dimensional (2D) measurements for doubling time calculations. Compared with computer-aided 3D volumetric measurement, 2D measurements have been found to be unreliable in volume change detection [9, 26]. Therefore, in the NELSON study 3D volumetric measurements were used to calculate volume and VDT. The 3-month interval was based on the VDT of 400 days that was initially chosen as cutoff value to identify fast-growing lung nodules [10]. The result of the current study implies that this interval for follow-up may be shortened for the short-term follow-up examination as part of the baseline screening round. For nodules with a volume increase >25%, the newly calculated screen interval with VDT cut-off of 232 days is 75 days. The median interval of the short-term follow-up CT examination for the participants included in our study was 93 days, so this period could be slightly shortened. However, it is questionable if the difference between 3 months and 2.5 months is relevant in terms of screening organization. A limitation of our study was the relatively small number of participants referred with fast-growing nodules, despite our study representing one of the largest CT lung cancer screening studies. The number of nodules included differed from the number of nodules with VDT <400 days in a previous publication because of our inclusion criteria [6]. The number of different lung cancer types in our study did not allow in-depth analysis of VDT by histology. If no histological diagnosis was obtained, we used as standard an absence of lung cancer diagnosis within 2 years of CT, a period that is considered long enough to classify a nodule as benign [15]. Mikita et al found that nodules with VDT <400 days all turned out to be malignant within a 2-year follow-up [27]. Actually, the mean follow-up in our study was 4.4 years, so it is unlikely that a lung cancer case has been overlooked among nodules assessed as benign. The chief limitation was the lack of external validation. The optimized VDT cut-off for the 3-month follow-up CT in the baseline round should be validated in another lung cancer screening study to assess its generalizability. In conclusion, all malignant, fast-growing lung nodules referred after the 3-month followup CT in the baseline screening round of the NELSON trial had a VDT ≤232 days. Lowering the VDT cut-off for this screening round may reduce false-positive referrals. Acknowledgements The NELSON-trial was sponsored by: Netherlands Organisation for Health Research and Development (ZonMw); Dutch Cancer Society Koningin Wilhelmina Fonds (KWF); Stichting Centraal Fonds Reserves van Voormalig Vrijwillige Ziekenfondsverzekeringen (RvvZ); Siemens Germany; Rotterdam Oncologic Thoracic Steering committee (ROTS); G. Ph. Verhagen Trust, Flemish League Against Cancer, Foundation Against Cancer and Erasmus Trust Fund. The funders played no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. References [1] National Lung Screening Trial Research Team, Aberle DR, Adams AM, Berg CD, Black WC, Clapp JD, et al. (2011). Reduced lung-cancer mortality with low-dose computed tomographic screening. The New England journal of medicine, 365(5):395– 409. [2] Infante M, Lutman FR, Cavuto S, Brambilla G, Chiesa G, Passera E, et al. (2008). Lung cancer screening with spiral CT: baseline results of the randomized DANTE trial. Lung cancer, 59(3):355–363. [3] Lopes Pegna A, Picozzi G, Mascalchi M, Maria Carozzi F, Carrozzi L, Comin C, et al. (2009). Design, recruitment and baseline results of the ITALUNG trial for lung cancer screening with low-dose CT. Lung cancer, 64(1):34–40. [4] Blanchon T, Brechot JM, Grenier PA, Ferretti GR, Lemarie E, Milleron B, et al. (2007). Baseline results of the Depiscan study: a French randomized pilot trial of lung cancer screening comparing low dose CT scan (LDCT) and chest X-ray (CXR). Lung cancer, 58(1):50–58. [5] Gohagan JK, Marcus PM, Fagerstrom RM, Pinsky PF, Kramer BS, Prorok PC, et al. (2005). Final results of the Lung Screening Study, a randomized feasibility study of spiral CT versus chest X-ray screening for lung cancer. Lung cancer, 47(1):9–15. [6] van Klaveren RJ, Oudkerk M, Prokop M, Scholten ET, Nackaerts K, Vernhout R, et al. (2009). Management of lung nodules detected by volume CT scanning. The New England journal of medicine, 361(23):2221–2229. [7] Henschke CI, Yankelevitz DF, Naidich DP, McCauley DI, McGuinness G, Libby DM, et al. (2004). CT screening for lung cancer: suspiciousness of nodules according to size on baseline scans. Radiology, 231(1):164–168. 54 [8] Swensen SJ, Jett JR, Sloan JA, Midthun DE, Hartman TE, Sykes AM, et al. (2002). Screening for lung cancer with low-dose spiral computed tomography. American journal of respiratory and critical care medicine, 165(4):508–513. [9] Yankelevitz DF, Reeves AP, Kostis WJ, Zhao B, and Henschke CI (2000). Small pulmonary nodules: volumetrically determined growth rates based on CT evaluation. Radiology, 217(1):251–256. [10] Xu DM, Gietema H, de Koning H, Vernhout R, Nackaerts K, Prokop M, et al. (2006). Nodule management protocol of the NELSON randomised lung cancer screening trial. Lung cancer, 54(2):177–184. [11] van Iersel CA, de Koning HJ, Draisma G, Mali WP, Scholten ET, Nackaerts K, et al. (2007). Risk-based selection from the general population in a screening trial: selection criteria, recruitment and power for the Dutch-Belgian randomised lung cancer multi-slice CT screening trial (NELSON). International journal of cancer.Journal international du cancer, 120(4):868–874. [12] Gietema HA, Schaefer-Prokop CM, Mali WP, Groenewegen G, and Prokop M (2007). Pulmonary nodules: Interscan variability of semiautomated volume measurements with multisection CT– influence of inspiration level, nodule size, and segmentation performance. Radiology, 245(3):888–894. [13] CBO (2004). Guideline - non-small cell lung carcer: staging and treatment. Van Zuiden Communications BV, Alphen aan de Rijn, The Netherlands. [14] Xu DM, van der Zaag-Loonen HJ, Oudkerk M, Wang Y, Vliegenthart R, Scholten ET, et al. (2009). Smooth or attached solid indeterminate nodules detected at baseline CT screening in the NELSON study: cancer risk during 1 year of follow-up. Radiology, 250(1):264–272. [15] MacMahon H, Austin JH, Gamsu G, Herold CJ, Jett JR, Naidich DP, et al. (2005). Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology, 237(2):395–400. [16] Xu DM, van Klaveren RJ, de Bock GH, Leusveld A, Zhao Y, Wang Y, et al. (2008). Limited value of shape, margin and CT density in the discrimination between benign and malignant screen detected solid pulmonary nodules of the NELSON trial. European Journal of Radiology, 68(2):347–352. [17] Nietert PJ, Ravenel JG, Leue WM, Miller JV, Taylor KK, Garrett-Mayer ES, et al. (2009). Imprecision in automated volume measurements of pulmonary nodules and its effect on the level of uncertainty in volume doubling time estimation. Chest, 135(6):1580–1587. [18] Ko JP, Berman EJ, Kaur M, Babb JS, Bomsztyk E, Greenberg AK, et al. (2012). Pulmonary Nodules: Growth Rate Assessment in Patients by Using Serial CT and Three-dimensional Volumetry. Radiology, 262(2):662–671. [19] Pedersen JH, Ashraf H, Dirksen A, Bach K, Hansen H, Toennesen P, et al. (2009). The Danish randomized lung cancer CT screening trial–overall design and results of the prevalence round. Journal of thoracic oncology, 4(5):608–614. [20] van den Bergh KA, Essink-Bot ML, Bunge EM, Scholten ET, Prokop M, van Iersel CA, et al. (2008). Impact of computed tomography screening for lung cancer on participants in a randomized controlled trial (NELSON trial). Cancer, 113(2):396– 404. [21] Brewer NT, Salz T, and Lillie SE (2007). Systematic review: the long-term effects of false-positive mammograms. Annals of Internal Medicine, 146(7):502–510. [22] Wilson DO, Ryan A, Fuhrman C, Schuchert M, Shapiro S, Siegfried JM, et al. (2012). Doubling times and CT screen-detected lung cancers in the Pittsburgh Lung Screening Study. American journal of respiratory and critical care medicine, 185(1):85–89. [23] Yankelevitz DF, Kostis WJ, Henschke CI, Heelan RT, Libby DM, Pasmantier MW, et al. (2003). Overdiagnosis in chest radiographic screening for lung carcinoma: frequency. Cancer, 97(5):1271–1275. [24] Revel MP, Merlin A, Peyrard S, Triki R, Couchon S, Chatellier G, et al. (2006). Software volumetric evaluation of doubling times for differentiating benign versus malignant pulmonary nodules. American journal of roentgenology, 187(1):135–142. [25] Winer-Muram HT, Jennings SG, Tarver RD, Aisen AM, Tann M, Conces DJ, et al. (2002). Volumetric growth rate of stage I lung cancer prior to treatment: serial CT scanning. Radiology, 223(3):798–805. [26] Revel MP, Bissery A, Bienvenu M, Aycard L, Lefort C, and Frija G (2004). Are two-dimensional CT measurements of small noncalcified pulmonary nodules reliable? Radiology, 231(2):453–458. [27] Mikita K, Saito H, Sakuma Y, Kondo T, Honda T, Murakami S, et al. (2012). Growth rate of lung cancer recognized as small solid nodule on initial CT findings. European Journal of Radiology, 81(4):e548–53.