Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
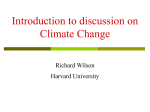
Method 500 400 300 200 Oxygen 100 20 40 60 80 Considering a metabolic production of CO2 at rest up to 250 mL/min, an effective removal should approach this value to control the breathing workload and to avoid respiratory acidosis in patients with hypercapnic respiratory failure. Alongside traditional techniques 100 pO2, pCO2 (mmHg) of respiratory assistance, a device that performs an extracorporeal CO2 removal facilitates and extends their current applications [11]. CO2 Due to the transport properties of blood, an extracorporeal CO2 removal treatment can also be efficiently performed using blood flows lower then 500 mL/min, well below the cardiac output. Pulmonary elimination In addition, an appropriate instrument and the low blood flow allow the profitable adoption of a single, small, veno-venous vascular access. Extracorporeal removal CO2 Minimally invasive extracorporeal CO2 removal system using continuous hemoperfusion. Technical characteristics Treatment mode Hemoperfusion Blood flow 100-450 mL/min Membrane type Phosphorylcholine-coated polymethylpentene Membrane surface 1.8 m2 Priming volume 220 mL Sterilization Ethylene oxyde Single circuit lasting 5 days Rinsing and priming 2L saline heparinized by 10000 UI Vascular access 13-14 Fr double lumen central venous catheter Codes Description Validity PLFLOW ESTORFLOW® CO2 removal blood pump PLMETER ProLUNG Meter® integrated module for continuous monitoring of removed CO2 and medical gas management PLLUNG5MD ProLUNG PLUS MD kit for extracorporeal CO2 removal 3 years CATFX1320 “High Flow” double lumen catheter (optional) 5 years References CO2 Peripheral methabolic intake 1. The acute respiratory distress syndrome network.Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Eng J Med 2000; 342 (18): 103-1308. 2. Hager DN, Krishnan JA, Hayden DL et al.Tidal Volume Reduction in Patients with Acute Lung Injury When Plateau Pressures Are Not High. Am J Respir Crit Care Med 2005; 172: 1241-1245. 3. Determann RM, Royakkers A, Wolthuis EK et al. Ventilation with lower tidal volumes as compared with conventional tidal volumes for patients without acute lung injury: a preventive randomized controlled trial. Crit Care 2010; 14: R1-R14. 4. Confalonieri M, Garuti G, Cattaruzza MS et al. A chart of failure risk for noninvasive ventilation in patients with COPD exacerbation. Eur Respir J 2005; 25: 348-355. 5. Conti G, Antonelli M, Navalesi P et al. Noninvasive vs. conventional mechanical ventilation in patients with chronic obstructive pulmonary disease after failure of medical treatment in the ward: a randomized trial. Int Care Med 2002; 28(12): 1701-7. 6. Prekker ME, Nath DS,Walker AR.Validation of the proposed International Society for Heart and Lung Transplantation grading system for primary graft dysfunction after lung transplantation. J Heart Lung Transplant 2006; 25(4): 371-8. 7. Brian JE. Carbon Dioxide and the Cerebral Circulation. Anesthesiology 1998; 88(5): 1365-86. 8. Kolobov T, Gattinoni L, Tomlinson TA et al. Control of breathing using an extracorporeal membrane lung. Anesthesiology 1977; 46: 138-141. 9. Baumann MH, Sahn SA. Medical management and therapy of bronchopleural fistulas in the mechanically ventilated patient. Chest 1990; 97: 721-8. 10.Schinco MA, Formosa VA, Santora TA.Ventilatory management of a bronchopleural fistula following thoracic surgery. Respir Care 1998; 43: 1064-9. 11.Gattinoni L, Carlesso E, Langer T. Towards ultraprotective mechanical ventilation. Curr Opin Anaesthesiol 2012; 25(2): 141-7. ESTOR S.P.A. Via Newton, 12 - 20016 Pero (MI) ITALY Tel. +39 (0) 23394161 - Fax +39 (0) 233912069 [email protected] • www.estor.it 60517000 03/2014 REV. 0 Gas concentration (mL/L) Blood tranports carbon dioxyde as dissolved, bound to hemoglobin and mainly under bicarbonate form. This triple mode allows to transport a huge amount of carbon dioxyde per unit of blood volume. As a consequence, a significant reduction of total blood CO2 content could be obtained by treat600 ing little amounts of blood per unit of time Carbon dioxyde when an effective device is used. 550 Minimally invasive extracorporeal CO2 removal system Indications The ProLung® System Carbon dioxide is continuously produced by cell respiration. The lungs are the organs responsible to its elimination. In cases of defect in alveolar ventilation, an acute accumulation of carbon dioxide (hypercapnia) and a subsequent significant decrease in pH (respiratory acidosis) could occur. The control of hypercapnia and respiratory acidosis allows to limit their effects on the central nervous and cardiovascular systems, as well as metabolic disorders. An adequate correction of hypercapnia and respiratory acidosis induced in various pathological conditions could be obtained by conventional techniques. However, in some cases, the conventional approach is no longer sufficient: “Exhacerbated COPD” Air flow VCO2 [ml/min] “Primary graft dysfunction” In the postoperative period of lung transplantation, in patients who develop primary graft dysfunction [6], associated with severe hypercapnia, extracorporeal CO2 removal allows to limit high pressure and volume of ventilation, otherwise harmful to the transplanted organ. CO2 “Traumatic brain injury” In patients with head injury and respiratory failure, extracorporeal CO2 removal helps to control intracranial pressure [7], added to the limitation of pressures and volumes of ventilation and the potential damage induced by mechanical ventilation on the lung. MEDICAL AIR + CO2 BLOOD RETURN ProLung In patients with ALI/ARDS and severe hypercapnia, refractory to a protective mechanical ventilation [1,2], the extracorporeal CO2 removal allows to limit pressure and volume of ventilation, otherwise necessary to control respiratory acidosis, but harmful to the lung (barotrauma and volutrauma) [3]. In presence of tissue lesions of respiratory system (bronchopleural fistula, rupture of the trachea or diaphragmatic injury), the adoption of minimum volumes and reduced ventilation pressures accelerates healing. Extracorporeal CO2 removal facilitates the adoption of minimally invasive ventilatory strategies [8-10], useful for these pathological conditions. MEDICAL AIR BLOOD UPTAKE HEPARIN 140 140 120 120 100 Removed CO2 100 60 40 4 20 2 [[mL/min] mL/min] 0 0 5 10 15 20 25 30 Time (hours) 35 40 45 50 Air temperature p 37 [[°C] °C ] TTreatment re eatment d data ata SSetpoint: etpoint: 37 The ProLung® circuit adopts the simple veno-venous hemoperfusion mode to remove CO2 within the filter. The extracorporeal support of a single circuit can last up to 5 days. The ProLung® filter made by high performance Phosphorylcholine-coated polymethylpentene, ensures CO2 removal higher than 100 mL/ min, in best usage conditions. MEDICAL AIR MEDICAL AIR + CO2 The Estorflow® hemoperfusion module adopts the volumetric control of blood flow, allowing flows of up to 450 mL/min.The pump characteristics ensure a flow rate almost constant to varying inflow and outflow blood pressures of the circuit.This optimizes blood flow also using minimally invasive catheters. PRESSURE “Tissue lesions” [[L/min] L/min] 80 • Autonomously manage medical air supplied to the ProLung® filter, by means of a feedback communica tion with the Estorflow® hemoperfusion module • Measure CO2 removed by the filter • Plot and store CO2 removal data and patients characteristics During an exacerbation of the disease, in patients with respiratory acidosis refractory to NIV support [5], the extracorporeal removal of CO2 allows to extend the application of NIV support, avoiding intubation and related infectious complications and hospital stay [5]. “ALI / ARDS” 8 The ProLung-Meter is the gas control unit of the ProLung® system, designed to: ® Volumetric pumps Centrifugal pumps FLOW RATE The Estorflow® module communicates realtime the treatment status to the gas control unit ProLung-Meter®, in order to ensure high standards of safety in the control of gas exchange.