Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
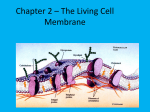
Bioscience Reports, Vol. 18, No. 2, 1998 The Effects of pH and Intraliposomal Buffer Strength on the Rate of Liposome Content Release and Intracellular Drug Delivery Robert J. Lee,1,2 Susan Wang,1,3 Mary Jo Turk,1 and Philip S. Low1,4 Received March 4, 1998; accepted March 31, 1998 Targeted liposomal drug formulations may enter cells by receptor-mediated endocytosis and then traffick by membrane flow into acidic intracellular compartments. In order to understand the impact of these intracellular pH changes on liposomal drug unloading, the effect of pH on the release from folate-targeted liposomes of three model compounds with distinct pH dependencies was examined. 5(6)-carboxyfluorescein, which titrates from its anionic to uncharged form following internalization by KB cells, displays strong endocytosis-dependent release, since only its uncharged (endosomal) form is membrane permeable. Endocytosis-triggered unloading of drugs of this sort is enhanced by encapsulating the drug in a weak buffer at neutral pH, so that acidification of the intraliposomal compartment following cellular uptake can occur rapidly. Sulforhodamine B, in contrast, retains both anionic and cationic charges at endosomal pH (~pH 5), and consequently, escapes the endosomes only very slowly. Doxorubicin, which is commonly loaded into liposomes in its membrane-impermeable (cationic) form using an acidic buffer, still displays endocytosistriggered unloading, since sufficient uncharged doxorubicin remains at endosomal pHs to allow rapid re-equilibration of the drug according to the new proton gradient across the membrane. In this case, when the extraliposomal [H+] increases 250-fold from 4x 10-8 M (pH 7.4, outside the cell) to 10-5 M (pH 5, inside the endosome), the ratio of doxorubicin inside to outside the liposome must decrease by a factor of 250. Therefore, the collapse of the transliposomal pH gradient indirectly drives an efflux of the drug molecule from the liposome. Since a change in intraliposomal pH is not required to unload drugs of this type, the intraliposomal compartment can be buffered strongly at acidic pH to prevent premature release of the drug outside the cell. In summary, pH triggered release of liposome-encapsulated drugs can be achieved both with drugs that increase as well as decrease their membrane permeabilities upon acidification, as long as the intraliposomal buffer strength and pH is rationally selected. KEY WORDS: Folate binding protein; endocytosis; drug targeting; liposomes; pH dependent drug release; drug carriers. ABBREVIATIONS: PEG, polyethylene glycol; PC, phosphatidylcholine; DSPE, distear oylphosphatidylethanolamine; PBS, phosphate-buffered saline (136.9 mM NaCl, 2.68 mM KC1, 8.1 mM Na2HPO4, 1.47 mM KH2PO4, pH 7.4). 1 Department of Chemistry, 1393 Brown Bldg., Purdue University, West Lafayette, IN 47907, USA. Present address: Division of Pharmaceutics and Pharmaceutical Chemistry, College of Pharmacy, Ohio State University, Columbus, OH 43210, USA. 3 Present address: ICOS Corporation, 22021 20th Ave. S.E., Bothell, WA 98021, USA. 4 To whom correspondence should be addressed. 69 2 0144-8463/98/0400-0069$15.00/0 © 1998 Plenum Publishing Corporation 70 Lee, Wang, Turk, and Low INTRODUCTION Liposomes are aqueous dispersions of phospholipids organized into bilayers resembling the structure of a cell membrane. Much interest has arisen in exploiting liposomes as potential vehicles for drug delivery due to their abilities to both entrap membrane impermeable hydrophilic molecules and to carry membrane soluble hydrophobic molecules within their lipid bilayers [1-3]. This interest has been heightened by breakthroughs in recent years that have greatly enhanced the potential applications of liposomal drug formulations in clinical medicine [4, 5]. These include: (1) development of long-circulating liposomes that avoid serum opsonization and the consequent rapid clearance by the reticuloendothelial system [6-9], (2) remoteloading of liposomal contents via a pH gradient, which allows the near quantitative encapsulation of drug molecules such as doxorubicin [10, 11], (3) synthesis of cationic liposomes which can serve as effective vehicles for gene delivery [12,13], and (4) design of ligand-targeted liposomes, that accumulate specifically in receptorexpressing tissues [14-17]. Taken together, these advancements predict an expanding role for liposomal drug formulations in the future treatment of human diseases. An important and usually rate-limiting step in targeted liposomal drug delivery is the unloading of the encapsulated cargo following endocytosis by the target cell. Drug release is thought to occur either by fusion of the liposome and the cell/ endosomal membrane, or by diffusion of the drug molecule across the two lipid bilayers. This liposome unloading can be followed by the dequenching of dyes such as carboxyfluorescein encapsulated in liposomes at self-quenching concentrations, or by observation of the released fluorophore's binding to cytosolic structures such as RNA [18-21]. "pH-sensitive" liposomes have also been developed to facilitate liposome "fusion" with endosomes at low endosomal pHs [22-24], However, while pH-sensitive liposomes may be effective in cytosolic drug delivery in vitro, they have been less successful in vivo, possibly due to loss of fusogenicity when exposed to serum. Consequently, strategies to develop "serum-stable" pH-sensitive liposomes have been explored [21, unpublished data], but their performance in vivo has yet to be thoroughly tested. We have recently developed the use of folic acid as a means of targeting liposomes encapsulating fluorescent dyes, anticancer drugs, genes, and antisense oligonucleotides to folate receptor-bearing cells [14, 25-27]. The membrane associated folate receptor, a glycosylphosphatidylinositol (GPI)-anchored protein with a Kd~0.1 nM for folate, has recently been identified as a marker for a variety of human tumors, especially ovarian carcinomas [28-31]. This overexpression of the folate receptor allows the specific targeting of liposomes to cancer cells via folate derivatization. Unlike most other endocytic pathways, folate receptor endocytosis occurs at "uncoated membrane invaginations" called caveolae [32], after which the receptorligand complex follows a non-degradative intracellular trafficking route. Importantly, rapid acidification occurs in early endosomal compartments leading to an average pH of the major folate-containing endosomes of 5.0 [33]. In this study, we have examined the effect of pH on the rate of drug release from stable, non-pH-sensitive liposomes using three different aqueous markers: 5(6)carboxyfluorescein, a self-quenching titratable fluorescent dye; doxorubicin, a titratable fluorescent anticancer drug; and sulforhodamine B, a non-titratable membrane Effect of pH on Liposomal Drug Release 71 impermeable fluorophore. Fluorescence dequenching assays and dual-channel laserscanning confocal microscopy have been employed to quantitate liposomal drug release both from free liposomes in buffer and from endosomal compartments following uptake by KB cells. Our analyses suggest that drugs that become either more membrane permeable or less membrane permeable at endosomal pHs can be similarly discharged from the internalized liposomes if the encapsulating buffer is chosen in a rational manner. MATERIALS AND METHODS Cell Line KB cells, a human nasopharyngeal epidermal carcinoma cell line kindly provided by the Purdue Cancer Center, were cultured in a low-folate medium (folatefree Dulbecco's modified Eagle's medium supplemented with 10% heat-inactivated fetal bovine serum) at 37°C in a humidified atmosphere containing 5% CO2 [33]. The folate content in the fetal bovine serum rendered the net folate concentration in the growth medium close to the physiological level for human adults [34]. pH-Dependence of Drug Release from Liposomes Suspended in Buffer The pH-dependent release of doxorubicin (Eastman Kodak Company, Rochester, New York) and 5(6)-carboxyfluorescein (Calbiochem Corp, San Diego, California) from liposomes was determined by a fluorescence dequenching assay. Folatetargeted liposomes composed of egg phosphatidylcholine (PC)/cholesterol/folatePEG-DSPE1 (60:40:0.1) were prepared, as described previously [25]. Remote loading of doxorubicin [10] into pre-formed vesicles containing the low pH "trapping" buffer (400 mM citrate, 5 mM phosphate, pH 4) was performed at a drug to lipid ratio of 1:10 (wt./wt.). Liposomes containing 100 mM 5(6)-carboxyfluorescein dissolved in pure water or sodium phosphate buffer (l0 mM or 50 mM, pH 7.4), were prepared by extrusion through a l00 nm pore-size polycarbonate membrane, as described previously [14]. Liposomes containing both 50 mM carboxyfluorescein and 50 mM sulforhodamine B dissolved in pure water were also prepared according to these procedures. All liposomes, eluted from a Sepharose CL-4B column (Pharmacia, Uppsala, Sweden) in phosphate buffered saline (PBS, 136.9 mM NaCl, 2.68 mM KC1, 8.1 mM Na2HPO4, 1.47 mM KH2PO4, pH 7.4), were stored at 4°C and were used within 2 weeks of preparation. To measure drug release, the liposomes were diluted to yield a final solution concentration of 20 fiM doxorubicin or 20 ^M 5(6)carboxyfluorescein in 2 ml of a universal pH buffer (120 mM NaCl, l0 mM sodium phosphate, 10 mM 2-morpholinoethanesulfonate, 10 mM sodium citrate) adjusted to a series of different pHs. The liposomes were then incubated at 37°C for various lengths of time. At each time point, 20 juL samples were removed, diluted with 2 mL PBS, and the fluorescence intensity of the samples was measured in a Perkin Elmer MPF-44A fluorescence spectrophotometer. One hundred percent dequenching was defined as the fluorescence intensity following liposome dissolution in 1% Triton 72 Lee, Wang, Turk, and Low X-100 (F\% Triton). The percent dequenching was then calculated using the equation: percent dequenching = (Ft - F0)/(F1% Triton -F0 ) x 100 where F, is the fluorescence following incubation for time t at 37°C and F0 is the fluorescence at time zero. Determination of Cytosolic Drug Delivery by Confocal Microscopy KB cells were plated in 35 mm culture dishes and grown for 24 h prior to the assay. The cells were incubated for 2 h at 37°C with folate targeted liposomes containing 20 jM carboxyfluorescein and 20 /J.M sulforhodamine B (final solution concentration). The cells were then washed 3 times in PBS and examined under a MRC600 confocal microscope. The excitation source was provided by the 488 nm and 568 nm lines of a krypton-argon mixed gas ion laser. A 1% neutral-density filter was added and the pin-hole diameter was set at 2 mm. Fluorescence signals emitted from cell-associated carboxyfluorescein fluorescence (green) and sulforhodamine B fluorescence (red) were separated with a DR560LP dichroic mirror combined with 522DF35 band-pass and 585EFLP long-pass emission filters and directed into 2 separate photomultipliers. Two 384-pixel by 512-pixel gray-level images of carboxyfluorescein and sulforhodamine B fluorescence were thus collected using a 60 x objective under the photon-counting mode and processed as described previously [25]. RESULTS Effect of Extraliposomal pH on the Rate of Drug Release in vitro Folate-PEG-liposomes have been shown to be internalized by receptor-bearing cells via folate receptor-mediated endocytosis [14]. To explore the impact of the low endosomal pH on the release of folate-targeted liposome-entrapped drug molecules, we examined the release rate of carboxyfluorescein and doxorubicin from egg PC/ cholesterol liposomes at different buffer pHs. Carboxyfluorescein is a negatively charged, membrane impermeable fluorescent dye at neutral pH. At acidic pH, however, it becomes partially protonated and membrane permeable [35, 36]. Doxorubicin is an anti-cancer chemotherapeutic agent that equilibrates across a membrane barrier according to the transmembrane pH gradient. Although it is poorly permeable in its protonated form, sufficient uncharged drug exists even at endosomal pHs to allow its rapid equilibration. Importantly, the fluorescence of carboxyfluorescein and doxorubicin are quenched at the intraliposomal concentrations used in this study, and consequently, their escape from liposomes can be monitored by fluorescence dequenching. As shown in Figs. 1 and 2, the kinetics of carboxyfluorescein and doxorubicin release display a strong pH-dependence. While the unloading rate at physiological pH (~ 7.4) is low, greater than 90% of doxorubicin is released from liposomal entrapment at a buffer pH of 5.0 within 2 h at 37°C. After 11 h incubation under identical conditions, liposomes containing carboxyfluorescein dissolved in Effect of pH on Liposomal Drug Release 73 pure water release nearly 80% of their contents. The strong pH dependence of carboxyfluorescein release probably arises from the fact that the uncharged membrane permeable population of carboxyfluorescein (CF0) increases relative to the total population (CFtotal) as the pH decreases, according to the equation: [CF°] = [CFtotal]/(l+Ka/[H+]) where Ka (~l0-4 M) is the acid dissociation constant of the dye. For this release to occur efficiently, the intraliposomal pH must be poorly buffered, so that any extraliposomal pH decrease can be rapidly transferred into the liposomes. As the intraliposomal pH buffering capacity is strengthened, intracellular unloading occurs more slowly (Fig. 1(B)). Therefore, to achieve the rapid unloading kinetics shown in Fig. 1(A), the carboxyfluorescein was dissolved in distilled water. The situation with doxorubicin is quite different, since its membrane permeant form decreases as the pH drops. In fact, retention of doxorubicin inside the liposome at neutral pH is achieved only by maintaining a strong pH gradient (inside acidic) across the liposomal membrane (Fig. 2). Thus, at equilibrium, the ratio of protonated doxorubicin inside the liposome to protonated doxorubicin outside the liposome must equal the ratio of proton concentrations in the same two compartments. Because sufficient uncharged doxorubicin is present even at endosomal pH to assure rapid equilibration across the liposomal membrane, the drug's distribution is dictated solely by the ratio of compartmental pHs. Consequently, the optimal liposomal formulation for doxorubicin will contain a strongly buffered acidic intraliposomal solution to assure retention of the drug within the liposome during transit to its target cell. Intracellular Release of Carboxyfluorescein Examined by Confocal Microscopy To further demonstrate the significance of endosomal pH on the cytoplasmic delivery of liposome-entrapped drug molecules, carboxyfluorescein and sulforhodamine B were co-encapsulated into folate-derivatized liopsomes (see Methods) and delivered into endosomal compartments by folate receptor-mediated endocytosis. Both probes are membrane impermeable at neutral or basic pH, and remain stably entrapped in their liposomal containers during storage under these pH conditions. However, at acidic pH, carboxyfluorescein becomes protonated and membrane permeable, while sulforhodamine B remains impermeable. As shown in Fig. 3, KB cells treated with these liposomes showed almost complete cytoplasmic release of the carboxyfluorescein, whereas sulforhodamine B remained sequestered within the endosomal compartments. These data indicate that neither liposome rupture nor fusion can account for carboxyfluorescein escape, but rather that the acidification encountered along the folate endocytosis pathway can lead to the selective intracellular release of drugs that achieve membrane permeability only at endosomal pHs. DISCUSSION In this study, we have examined the role of pH on the release from liposomes of two fluorescent dyes and an anticancer drug, doxorubicin. KB cells were employed in 74 Lee, Wang, Turk, and Low Fig. 1. pH dependence of carboxyfluorescein release from liposomes. A. Folate-PEGliposome-entrapped carboxyfluorescein (dissolved at l00 mM concentration in distilled water, pH 7.4) was incubated at 37°C at pH 5.0 (solid circles), 6.0 (open circles), or 7.4 (solid triangles). Drug release from the liposomes was monitored by its fluorescence dequenching (A e x , 495 nm; A™,, 520 nm), as described in Materials and Methods. B. Same as part A, except the carboxyfluorescein was dissolved in distilled water (solid circles), l0 mM sodium phosphate (open circles), or 50 mM sodium phosphate (solid triangles), pH 7.4, prior to incubation at 37°C in the universal buffer, pH 5.0. Effect of pH on Liposomal Drug Release 75 Fig. 2. pH dependence of doxorubicin release from liposomes. Folate-PEG-liposomeentrapped doxorubicin (dissolved in 400 rnM citrate, 5mM phosphate buffer, pH4) was incubated at 37°C at pH 5.0 (solid circles), 6.0 (open circles), or 7.4 (solid triangles). Drug release from the liposomes was monitored by its fluorescence dequenching (A ex ,475 nm; k em, 580 nm), as described in Materials and Methods. the study because of their high capacity for folate receptor-mediated endocytosis. A pH-insensitive lipid composition, egg PC/cholesterol/folate-PEG-DSPE (60:40: 0.1), was also used to allow us to focus solely on the effects of the pH-sensitive properties of the entrapped fluorophores or drug molecules. Following folate receptor-mediated endocytosis, liposomes are exposed to low pH. As the internal pH of the liposome gradually equilibrates with the endosomal pH, a fraction of the 5(6)-carboxyfluorescein molecules is converted to a protonated form which is membrane permeable [35]. These molecules can then diffuse through the liposomal and endosomal bilayers into the cytosol. In the cytosol, 5(6)-carboxyfluorescein molecules once again become deprotonated (negatively charged) due to the high cytoplasmic pH (near neutral) and become "trapped" inside the cytosol. During this process, the normal liposomal and/or the endosomal membrane's permeability barrier function remains intact as shown by the lack of significant release of sulforhodamine B co-encapsulated in the same vesicles. This suggests that the cytosolic release of 5(6)-carboxyfluorescein derives exclusively from the properties of the fluorophore itself in the absence of liposome-endosome fusion and/or endosome disruption. The data also indicate that if 5(6)-carboxyfluorescein is to be employed as an aqueous phase marker in membrane fusion assays, the intraliposomal pH must be strongly buffered in the alkaline range to prevent rapid titration of the marker to its membrane permeable form. The effect of pH on liposomal content efflux was also examined in an earlier study by Straubinger et al. [36]. Their experiments showed that liposomes entrapping 76 Lee, Wang, Turk, and Low Effect of pH on Liposomal Drug Release 77 carboxyfluorescein release their content into the cytosol following non-specific endocytosis by CV-1 cells. In contrast, Straubinger et al. also noted that the more highly charged calcein and a high molecular weight FITC-dextran, like the sulforhodamine B used in the current study, remain confined in endosomal compartments. They also showed that carboxyfluorescein was released from the liposomes in a pH-dependent manner, in agreement with the data presented in the current study. Our observations reaffirm the important role of pH in liposomal drug release. In addition, regulating the intraliposomal buffer strength is suggested as a method to stabilize liposomal entrapment of weakly acidic (or basic) drug molecules. Contrary to 5(6)-carboxyfluorescein, doxorubicin is more membrane permeable at basic pH than acidic pH. Therefore, the enhanced efflux of doxorubicin as the solution pH is lowered (Fig. 2) requires explanation. When liposomes entrapping doxorubicin are internalized by the cell and trafficked to acidic endosomes, the previous inward directed proton gradient required for remote loading nearly disappears. Because substantial uncharged (permeable) doxorubicin still exists at endosomal pH, this change in proton gradient now drives the release of doxorubicin in an analogous but opposite direction to the initial remote loading mechanism; i.e. at equilibrium, the concentration of doxorubicin in any membrane surrounded compartment will be directly proportional to the proton concentration in that compartment. Unfortunately, due to the additional presence of a pH gradient between the endosome and cytosol, doxorubicin may still be partially retained in the extraliposomal endosomal compartments. This suggestion is, in fact, consistent with our previous confocal microscopy data on the intracellular distribution of doxorubicin delivered by folatePEG-liposomes into KB cells [25]. In that study, a punctate pattern of doxorubicin fluorescence was still observed in the cytoplasmic regions, suggesting significant endosomal retention. Eventually, even these doxorubicin molecules will escape into the cytosol and/or the nucleus where they may be "trapped" due to binding to cytosolic/nuclear components such as RNA and DNA. Such escape may also be encouraged by the lower pH in the cytosols of some tumor cells. In summary, our results suggest that the pH titration behavior of liposomeentrapped drug molecules must be considered in the design of liposome-mediated delivery systems that enter cells by endocytosis. Where the drug is only permeable at low pHs, selective intracellular unloading can be engineered by entrapping the drug within the liposome at high pH in a poorly buffered medium. In contrast, where the drug is more membrane permeable at high pH but retains some permeability at endosomal pHs, cell specific unloading can be achieved by entrapping the agent within the liposome in a strongly buffered acidic medium. The reduced pH within the endosome will then promote the diffusional release of both types of drug molecules, despite the fact that the former loses electrostatic charge while the latter gains electrostatic charge in the lower pH environment. The low pH commonly measured in anaerobic tumor masses could further facilitate liposomal cargo unloading, as noted in a recent study by Papahadjopoulos and colleagues [37]. ACKNOWLEDGMENTS This work was supported in part by grants from the National Institutes of Health (GM08298) and from Endocyte, Inc. 78 Lee, Wang, Turk, and Low REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. Lichtenberg, D. (1988) Methods Biochem. Anal. 33:337-462. Litzinger, D. C. and Huang, L. (1992) Biochim. Biophys. Acta 1113:201-227. Betageri, G. V. (1993) Technomic Publ. Lancaster, Pennsylvania. Blume, G., Cevc, G., Crommelin, M. D. J. A., Bakker-Woudenberg, I. A. J. M., Kluft, C., and Storm, G. (1993) Biochim. Biophys. Acta 1149:180-184. Torchilin, V. P., Klibanov, A. L., Huang, L., O'Donnell, S., Nossiff, N. D., and Khaw, B. A. (1992) FASEBJ. 6:2716-2719. Papahadjopoulos, D. et al. (1991) Proc. Natl. Acad. Sci. U.S.A. 88:11460-11464. Mori, A., Klibanov, A. L., Torchilin, V. P., and Huang, L. (1991) FEBS Lett. 284:263-266. Woodle, M. C. and Lasic, D. D. (1992) Biochim. Biophys. Acta 1113:171-199. Moghimi, S. M. and Patel, H. M. (1992) Biochim. Biophys. Acta 1135:269-274. Mayer, L. D. et al. (1989) Cancer Res. 49:5922-5930. Mayer, L. D., Bally, M. B., Loughrey, H., Masin, D., and Cullis, P. R. (1990) Cancer Res. 50:575579. Feigner, P. L. and Ringold, G. M. (1989) Nature 337:387-388. Gao, X. and Huang, L. (1991) Biochem. Biophys. Res. Commun. 179:280-285. Lee, R. J. and Low, P. S. (1994) J. Biol. Chem. 269:3198-3204. Leserman, L. D., Weinstein, J. N., Blumenthal, R., and Terry, W. D. (1980) Proc. Natl. Acad. Sci. U.S.A. 77:4089-4093. Lundberg, B., Hong, K., and Papahadjopoulos, D. (1993) Biochim. Biophys. Acta 1149:305-312. Mori, A., Kennel, S. J., and Huang, L. (1993) Pharm. Res. 10:507-514. Weinstein, J. N., Yoshikami, S., Henkart, P., Blumenthal, R., and Hagins, W. A. (1977) Science 195:489-492. Szoka, F. C., Jacobson, K., and Papahadjopoulos, D. (1979) Biochim. Biophys. Acta 551:295-303. Leserman, L. D., Barbel, J., Kourilsky, F. and Weinstein, J. N. (1980) Nature 288:602-604. Vogel, K., Wang, S., Lee, R. J., Low, P. S., and Chmielewski, J. A. (1995). J. Am. Chem. Soc. 118:1581. Connor, J., Yatvin, M. B., and Huang, L. (1984) Proc. Natl. Acad. Sci. U.S.A. 81:1715-1718. Chu, C.-J., Dijkstra, J., Lai, M. Z., Hong, K., and Szoka, F. C. (1990) Pharm. Res. 7:824-834. Jizomoto, H., Kanaoka, E., and Hirano, K. (1994) Biochim. Biophys. Acta 1213:343-348. Lee, R. J. and Low, P. S. (1995) Biochim. Biophys. Acta 1233:134-144. Wang, S., Lee, R. J., Cauchon, G., Gorenstein, D. G., and Low, P. S. (1995) Proc. Natl. Acad. Sci. U.S.A. 92:3318-3322. Lee, R. J. and Huang, L. (1996) J. Biol. Chem. 271:8481-8487. Rettig, W., Garin-Chesa, P., Beresford, H., Oettgen, H., Melamed, M., and Old, L. (1988) Proc. Natl. Acad. Sci. U.S.A. 85:3110-3114. Campbell, I. G., Jones, T. A., Foulkes, W. D., and Trowsdale, J. (1991) Cancer Res. 51:5329-5338. Garin-Chesa, P., Campbell, I., Saigo, P., Lewis, J., Old, L., and Rettig, W. (1993) Am. J. Pathol. 142:557-567. Ross, J. F., Chaudhuri, P. K., and Ratnam, M. (1994) Cancer 73:2432-2443. Rothberg, K. G., Ying, Y. S., Kolhouse, J. F., Kamen, B. A., and Anderson, R. G. W. (1990) J. Cell Biol. 110:637-649. Lee, R. J., Wang, S., and Low, P. S. (1996) Biochim. Biophys. Acta 1312:237-242. Antony, A. C., Kane, M. A., Portillo, R. M., Elwood, P. C., and Kolhouse, J. F. (1985) J. Biol. Chem. 260:14911-14917. Haugland, R. P. (1992-1994) Handbook of fluorescent probes and research chemicals. Larison, K. D. (Ed.) Molecular Probes, Inc., Oregon. Straubinger, R. M., Hong, K., Friend, D. S., and Papahadjopoulos, D. (1983) Cell 32:1069-1079. Yuan, F., Leunig, M., Huang, S. K., Berk, D. A., Papahadjopoulos, D., and Jain, R. K. (1994) Cancer Res. 54:3352-3356.