Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
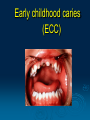
March 2012 Most common dental conditions in children Done by: Dr Lina Sarkis Abi Doumit Specialist in pediatric dentistry Learning objectives: To identify the most common conditions seen in pediatric dentistry. To learn about the importance of earlier diagnosis & earlier interventions. demineralization & remineralisation. To describe the new concept of TX. To discuss the fluoride use in caries prevention. To discuss the new recommendation for prevention. Introduction Healthy teeth & gums are essential to any child’s overall health and common dental problems can result in very painful & dangerous infections, speech development problems or delay and poor self image. Dental problems should receive home care and clinical care to avoid becoming a more serious issue later. Early childhood caries (ECC) Definition Severe tooth decay in young children has long been recognized as a clinical syndrome and has been referred to by various names, including “nursing caries,” “nursing bottle syndrome,” “night bottle mouth,” and “baby bottle tooth decay.” Terminology The Centers for Disease Control and Prevention recently suggested that the terms for this clinical syndrome be replaced with “Early Childhood Caries (ECC)” because the latest research showed that the use of bottles is not the only cause of ECC. What is early childhood caries? Early childhood caries is a “virulent” form of dental caries that can destroy the teeth of preschool children and toddlers. Early childhood caries can also be defined as the occurrence of any sign of dental caries on any tooth surface during the first 3 years of a child’s life. ECC is an infectious disease, and the Streptococcus mutans bacteria is the main causative agent, which does not only produce acid, but also thrives in it. In children with ECC, oral SM levels routinely exceed 30% of the cultivable dental plaque flora. Transmission The most common source, from which infants acquire MS, is their mother (vertical transmission). ECC begins with bacteria, especially mutans streptococci (MS). Plaque is a film of bacteria on teeth. Sugar (fermentable carbohydrates) is food for the bacteria which then produce acids. These acids attack the tooth enamel for 20 minutes or longer! This happens every time your baby drinks a sugary liquid and after multiple acid attacks teeth can begin to decay. Consumption of juice Sucrose, Glucose & Fructose contained in fruit juices are easily metabolized by S. mutans to form acids that dissolve enamel. How are dental caries produced? Dental caries in children is typically observed clinically as a “white spot lesion”. If the tooth surface remains intact and non-cavitated, then remineralization of the enamel is possible. If the subsurface of the demineralization of enamel is extensive, it eventually causes the collapse of the overlying tooth surface, resulting in a cavity. Pathology process The caries process is thought of as a dynamic alteration between demineralization and remineralization phases. The process of demineralization and dental caries formation begins when cariogenic microorganisms are present in large numbers and dietary fermentable carbohydrates become available in the dental biofilm. Pathologic factors Bacteria Carbohydrates Protective factors Saliva Calcium Phosphate Fluoride Photomicrographs, dental histology pictures, SEM, microscope Demineralisation of enamel Risk factors for dental caries Frequent intake of carbohydrate-rich or sugary foods a low pH on the surfaces of the teeth. Night- time bottle feeding, or prolonged use of a Sippy cup. The earlier that a child’s mouth is infected with Mutans streptococci, the greater the risk for future caries development. A low fluoride level on the surface of the teeth reduces the remineralization process and increases the risk for caries. When the saliva flow is below 0.7 ml/minute, the saliva cannot wash carbohydrates off the dental surface. Finally, a low socioeconomic status can reduce interest in oral hygiene and a healthy diet. Risk factors Test revealed statistically significant differences (p<0.05) regarding to age group, duration of the habit of drinking milk before bedtime, and age at which oral hygiene started. Higher prevalence of ECC was associated with the older age group, higher duration of the bedtime feeding habit (>12 months of age), and later start of oral hygiene (>12 months of age). J. Appl. Oral Sci. vol.17 no.1 Bauru Jan./Feb. 2009 Associated risk factors Multiple risk factors are involved in the development of early childhood caries. Ones of particular importance are demographic (e.g., child's age), social (e.g., annual household income), and psychosocial factors (e.g., parental/caregiver depression) that are indirectly linked to ECC. J Contemp Dent Pract. 2010 Oct 14;11(5):001-8d High risk patient Children with disabilities and special needs are at greater risk for health problems. Children with behavioral problems, impaired mobility, neuromuscular problems. Children with Gastro esophageal reflux. 3 year-old patients with already 4 teeth with carious lesions. Low socioeconomic status… Complications of earlier extractions Drifting / tipping of teeth. Delay of eruption of permanent teeth. Loss of arch length. Midline shift. Crowding of permanent teeth. Impactions. 3 year-old patient 4 year-old patient 4year-old patient 6year-old patient Role of saliva Neutralizing acid challenges. Flushing food and bacteria from the oral cavity. Acting as lubricant. Delivering calcium phosphate and fluoride to the tooth surface. Saliva needs to be at neutral ph (around 7), for teeth to mineralize properly. Dry mouth increase cavity risk. Stookey GK,J Am Dent Assoc.2008 May;139:11S-17S Dry mouth Side effects of many drugs as: -anxiety. -depression -allergies,cold,antihistaminic asthma. Side effects of some disease as HIV, hypertension. Damage of salivary gland. Mouth breather. Concept of Treatment In the past the treatment for dental caries was to “drill and fill.” Restorative dentistry unfortunately has little long-term impact on oral S. mutans levels. Control of disease PREVENTION TX back up Before TX 4 year-old patient: TX under GA After TX Fissure sealant To apply a plastic material to one or more teeth. To prevent rapid penetration of caries. Evidence based cohrane library studies (involving 3 897 children/adolescents) from 1966–2003, with follow-up time at least two years. T he risk reduction: decayed surfaces in sealed teeth divided by the number of decayed surfaces in the controls) was 33% for the fi rst permanent molars for resin-based sealants after 2–5 years follow-up Evidence based Placement of resin-based sealants on the permanent molars of children and adolescents is effective for caries reduction (Ahovuo-Saloranta et al. 2004, 2008). Reduction of caries ranged from 86% at 12 months to 57% at 48 to 54 months (Ahovuo-Saloranta et al. 2004). EFFICACITY Cooperative issue operculum Excellent Marginal seal Moisture control issue No leakage 2) Reduction of risk levels Reduction of sugar intake,diet advices, Increasing Fl use at home. Awareness health program. 3) Remineralization of teeth Fluoride toothpaste twice daily. Recommendations for fluoride supplementation can be made based on Fluoride content of water. Xylitol gum is recommended. Other source of Ca (cheese). Fluorosis Defect in the enamel. Teeth impacted by fluorosis have visible discoloration. White spots to brown and black stains. Increase in enamel porosity. Severe fluorosis Due to exposure of water naturally fluoridated.with level above the limit. From shallow well & hand pumps. The severity of fluorosis depends on the amount of fluoride exposure. A common source of extra fluoride is unsupervised use of toothpaste in very young children. Level of Fluoride in toothpaste 500 ppm. 1000 ppm. 1040 ppm. 1450 ppm. 1500 ppm. fluoride cereals, baby cereals. deboned chicken. canned fish and shellfish ,sardine all fruit juices, including apple, grape. others, soft drinks of all kinds, teas and tea mixes, beers, wines, some alcoholic drinks. Fruits and vegetables cultivated in countries with fluoridated water. Fluorization process • Enamel is composed mainly of a mineral known as "calcium hydroxyapatite", and its crystal structure is somewhat porous. This characteristic makes enamel vulnerable to dissolution in acids, as well as to deposits of stain-producing compounds. Long term follow-up Follow up at home. Office recall frequency every 3 months for high risks patients. 6 months for low risk patients. Tips for the parents The American Academy of Pediatric Dentistry, the American Dental Association, and the Academy of General Dentistry recommend: That children visit a dentist within six months of the eruption of the first tooth, and no later than 12 months of age. Infants should not be put to sleep with a bottle. Breast-feeding at night should be avoided after 12 months of age. Infants should be weaned from the bottle at 12-14 months of age. Juice should be offered to a child only in a cup. Infants and toddlers should drink no more than 6 ounces of juice per day. Cleansing of the baby teeth should be started by the time of eruption of the first primary tooth. For school age children Sweets should be eaten with meals, instead of as a stand alone snack. Milk and water better then soft drinks. Cheese is a helpful snack. Limit snacking. Pathological/ Protective factors. Participation of the parents. Preventive activities at early ages. References 1- World Health Organization. The World Oral Health report 2003. Geneva: WHO; 2003. http://www.who. int/oral_health. 2-Community Dentistry and Oral Epidemiology Volume 27, Issue 6, pages 442–448, March 2007. 3- Dominick P. Nutrition Reviews Volume 60, Issue 4, pages 97– 103, April 2002. 4- Ribelles M,Eur J Paediatr Dent.2010 Mar;11(1):9-14. 5- Angus C cameron ,Richard P Widmer .Handbook of pediatric dentistry .third edition 6- J.Timothy, Dimensions of Dental Hygiene. February 2010; 8(2): 40, 42, 44. 7- Angus C cameron ,Richard P Widmer .Handbook of pediatric dentistry .third edition. 8- Community Dentistry and Oral Epidemiology Volume 27, Issue 6, pages 442–448, March 2007. 9-Daniel Ravel,Pediatric Dental Health. Nov 2004 ;1-20 10- Marinho VC, Higgins JP, Logan S, Sheiham A. Fluoride toothpastes for preventing dental caries in children and adolescents (Cochrane review). In: The Cochrane Library, Issue 1, 2004. Chichester, UK: John Wiley & Sons Ltd. 11- Guideline on Fluoride therapy (AAPD ) ,REVISED 2014