Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
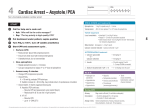
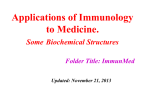
Repeated Administration of Vasopressin but Not Epinephrine Maintains Coronary Perfusion Pressure After Early and Late Administration During Prolonged Cardiopulmonary Resuscitation in Pigs Volker Wenzel, Karl H. Lindner, Anette C. Krismer, Egfried A. Miller, Wolfgang G. Voelckel and Werner Lingnau Circulation. 1999;99:1379-1384 doi: 10.1161/01.CIR.99.10.1379 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1999 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/99/10/1379 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/ Downloaded from http://circ.ahajournals.org/ by guest on March 5, 2014 Repeated Administration of Vasopressin but Not Epinephrine Maintains Coronary Perfusion Pressure After Early and Late Administration During Prolonged Cardiopulmonary Resuscitation in Pigs Volker Wenzel, MD; Karl H. Lindner, MD; Anette C. Krismer, MD; Egfried A. Miller, BS; Wolfgang G. Voelckel, MD; Werner Lingnau, MD Background—It is unknown whether repeated dosages of vasopressin or epinephrine given early or late during basic life support cardiopulmonary resuscitation (CPR) may be able to increase coronary perfusion pressure above a threshold between 20 and 30 mm Hg that renders defibrillation successful. Methods and Results—After 4 minutes of cardiac arrest, followed by 3 minutes of basic life support CPR, 12 animals were randomly assigned to receive, every 5 minutes, either vasopressin (early vasopressin: 0.4, 0.4, and 0.8 U/kg, respectively; n56) or epinephrine (early epinephrine: 45, 45, and 200 mg/kg, respectively; n56). Another 12 animals were randomly allocated after 4 minutes of cardiac arrest, followed by 8 minutes of basic life support CPR, to receive, every 5 minutes, either vasopressin (late vasopressin: 0.4 and 0.8 U/kg, respectively; n56), or epinephrine (late epinephrine: 45 and 200 mg/kg, respectively; n56). Defibrillation was attempted after 22 minutes of cardiac arrest. Mean6SEM coronary perfusion pressure was significantly higher 90 seconds after early vasopressin compared with early epinephrine (5064 versus 3463 mm Hg, P,0.02; 4265 versus 1563 mm Hg, P,0.0008; and 3765 versus 1163 mm Hg, P,0.002, respectively). Mean6SEM coronary perfusion pressure was significantly higher 90 seconds after late vasopressin compared with late epinephrine (4063 versus 2264 mm Hg, P,0.004, and 3264 versus 1564 mm Hg, P,0.01, respectively). All vasopressin animals survived 60 minutes, whereas no epinephrine pig had return of spontaneous circulation (P,0.05). Conclusions—Repeated administration of vasopressin but only the first epinephrine dose given early and late during basic life support CPR maintained coronary perfusion pressure above the threshold that is needed for successful defibrillation. (Circulation. 1999;99:1379-1384.) Key Words: cardiopulmonary resuscitation n vasopressin n epinephrine n perfusion n drugs T he role of epinephrine during cardiopulmonary resuscitation (CPR) is currently controversial. In laboratory studies, epinephrine during CPR has been associated with an increase of myocardial oxygen consumption,1 ventricular arrhythmias,2 ventilation-perfusion defect,3 and more severe postresuscitation myocardial dysfunction.4 In clinical trials, epinephrine did not result in better outcome than did saline placebo.5 Furthermore, high-dose epinephrine was not able to improve hospital discharge rates.6 – 8 In laboratory investigations of cardiac arrest from either ventricular fibrillation9 or pulseless electrical activity,10 vasopressin provided more effective vital organ blood flow9,10 and cerebral oxygen delivery11 than did epinephrine. In preliminary clinical trials, vasopressin resulted in return of spontaneous circulation after unsuccessful prolonged advanced cardiac life support with epinephrine.12 Compared with epinephrine, vasopressin significantly improved 24-hour survival rate in a small (n540) study of patients with ventricular fibrillation.13 Although the American Heart Association14 and the European Resuscitation Council15 recommend repeated administration of epinephrine during advanced cardiac life support, it is unknown whether epinephrine given repeatedly during CPR may be effective or whether this strategy may even result in inadvertent catecholamine toxicity. Moreover, it is unknown whether repeated administration of vasopressin Received July 29, 1998; revision received October 21, 1998; accepted November 3, 1998. From the Department of Anesthesia and Intensive Care Medicine, Leopold-Franzens-University of Innsbruck, Austria. This article was submitted as an abstract to the 28th Educational and Scientific Symposium of the Society of Critical Care Medicine, San Francisco, Calif, January 23–27, 1999. Correspondence to Dr Volker Wenzel, The Leopold-Franzens-University of Innsbruck, Department of Anesthesia and Intensive Care Medicine, Anichstrasse 35, 6020 Innsbruck, Austria. E-mail [email protected] Reprint requests to Dr Karl H. Lindner, The Leopold-Franzens-University of Innsbruck, Department of Anesthesia and Intensive Care Medicine, Anichstrasse 35, 6020 Innsbruck, Austria. © 1999 American Heart Association, Inc. Circulation is available at http://www.circulationaha.org 1379 Downloaded from http://circ.ahajournals.org/ by guest on March 5, 2014 1380 Repeated Vasopressin vs Epinephrine During CPR TABLE 1. Flow Chart of the Experimental Protocol Preparation, min 0 120*† VF, min 0 Cardiopulmonary Resuscitation, min 4 0 3† 4.5† Early vasopressin vs early epinephrine: 1 DA1 Late vasopressin vs late epinephrine: 8† Postresuscitation Phase, min 9.5† 13† 14.5† 1 DA2 1 DA3 1 DA1 1 18† 5† 15† 30† 60† DA2 Defibrillation 1 VF indicates ventricular fibrillation; DA, drug administration. Early vasopressin vs early epinephrine: DA1, 0.4 U/kg vasopressin vs 45 mg/kg epinephrine; DA2, 0.4 U/kg vasopressin vs 45 mg/kg epinephrine; DA3, 0.8 U/kg vasopressin vs 200 mg/kg epinephrine. Late vasopressin vs late epinephrine: DA1, 0.4 U/kg vasopressin vs 45 mg/kg epinephrine; DA2, 0.8 U/kg vasopressin vs 200 mg/kg epinephrine. *Sampling of blood gases; †measurement of hemodynamic variables. during CPR is effective and whether such a treatment regimen may result in prolonged elevated systemic vascular resistance, which may induce cardiac failure in the postresuscitation phase. Furthermore, the effects of vasopressin versus epinephrine may vary significantly when given early or late during basic life support (BLS) CPR. Accordingly, the purpose of the present investigation was to evaluate the effects of repeated administration of optimal (0.4 U/kg) and high (0.8 U/kg) dosages of vasopressin versus optimal (45 mg/kg) and high (200 mg/kg) dosages of epinephrine in a porcine cardiac arrest model simulating a short (3 minutes) and prolonged (8 minutes) duration of BLS with subsequent advanced cardiac life support. Methods Surgical Preparation and Measurements This project was approved by the Austrian Federal Animal Investigational Committee, and the animals were managed in accordance with American Physiological Society and institutional guidelines. This study was performed according to Utstein-style guidelines16 on 24 healthy, 12- to 16-week-old swine (Tyrolean domestic pigs) of either sex weighing 30 to 40 kg. The animals were fasted overnight but had free access to water. The pigs were premedicated with azaperone (neuroleptic agent; 4 mg/kg IM) and atropine (0.1 mg/kg IM) 1 hour before surgery, and anesthesia was induced with thiopental (7 to 15 mg/kg IV). After intubation during spontaneous respiration, the pigs were ventilated with a volume-controlled ventilator (Draeger EV-A) with 100% O2 at 20 breaths per minute and with a tidal volume adjusted to maintain normocapnia. Anesthesia was maintained with propofol (6 to 8 mg z kg21 z h21) and a single dose of piritramide (30 mg). We achieved muscle paralysis with 8 mg pancuronium after intubation and subsequently with repeated doses of 8 mg pancuronium as needed. Ringer’s solution (6 mL z kg21 z h21) and a 3% gelatin solution (4 mL z kg21 z h21) were administered in the preparation phase before induction of cardiac arrest and in the postresuscitation phase. A standard lead II ECG was used to monitor cardiac rhythm; depth of anesthesia was judged according to blood pressure, heart rate, and electroencephalography (Neurotrac, Engström). If cardiovascular variables or electroencephalography indicated a reduced depth of anesthesia, we increased the propofol dose, and additional piritramide was given. Body temperature was maintained with a heating blanket between 38.0°C and 39.0°C. A 7F catheter was advanced into the descending aorta via femoral cutdown for withdrawal of arterial blood samples and measurement of arterial blood pressure. A 5F pulmonary artery catheter was placed in the pulmonary artery via cutdown in the neck to measure cardiac output and to sample mixed venous blood. Cardiac output was measured with the thermodilution technique, and cardiac index was calculated by dividing cardiac output by body weight. Another 7F catheter was placed into the right atrium via femoral cutdown to measure right atrial pressure and for drug administration. Aortic, right atrial, and pulmonary artery pressures were measured with saline-filled catheters attached to pressure transducers (model 1290A, Hewlett Packard) that were calibrated to atmospheric pressure at the level of the right atrium; pressure tracings were recorded with a data acquisition system (Dewetron port 2000). Coronary perfusion pressure (CPP) was defined as the difference between aortic and right atrial diastolic pressures. Blood gases were measured with a blood gas analyzer (Chiron Diagnostics), and end-tidal carbon dioxide was measured with an infrared absorption analyzer (Sirecust 960, Siemens). Experimental Protocol Fifteen minutes before cardiac arrest, 5000 U heparin IV was administered to prevent intracardiac clot formation, a single dose of 15 mg piritramide and 8 mg pancuronium was given, and hemodynamic parameters as well as blood gases were measured. A 50-Hz, 60-V alternating current was then applied via 2 subcutaneous needle electrodes to induce ventricular fibrillation. Cardiopulmonary arrest was defined as the point at which the aortic pressure decreased profoundly to hydrostatic pressure, and the ECG showed ventricular fibrillation; ventilation was stopped at that point. After 4 minutes of untreated ventricular fibrillation, closed-chest CPR was performed manually, and mechanical ventilation was resumed at the same setting as before induction of cardiac arrest. Chest compression, guided by acoustical audiotones, was always performed by the same investigator at a rate of 80 compressions per minute. This investigator was blinded to hemodynamic and end-tidal carbon dioxide monitor tracings. The first part of the study was designed to simulate administration of vasopressors after a short period of BLS CPR. Accordingly, after 4 minutes of ventricular fibrillation followed by 3 minutes of BLS CPR, 12 animals were randomly assigned to receive either vasopressin (early vasopressin group: 0.4, 0.4, and 0.8 U/kg; n56) or epinephrine (early epinephrine group: 45, 45, and 200 mg/kg; n56) after 3, 8, and 13 minutes of CPR, respectively (Table 1). The second part of the study was designed to simulate administration of vasopressors after a prolonged period of BLS CPR. Thus, 12 animals were randomly allocated after 4 minutes of ventricular fibrillation and 8 minutes of BLS CPR to receive either vasopressin (late vasopressin group: 0.4 and 0.8 U/kg; n56) or epinephrine (late epinephrine group: 45 and 200 mg/kg; n56) after 8 and 13 minutes of CPR, respectively (Table 1). All drugs were diluted to 10 mL with normal saline and subsequently injected into the right atrium, followed by 20 mL saline flush (investigators were blinded to the drugs). Hemodynamic parameters were measured before induction of cardiac arrest, after 3 minutes of CPR, and 90 seconds and 5 minutes after each drug administration, respectively. After 22 minutes of cardiac arrest, including 18 minutes of CPR, up to 5 countershocks were administered with an energy of 3, 4, and 6 J/kg. If asystole or pulseless electrical activity was present after defibrillation, the experiment was terminated. Return of spontaneous circulation was defined as an unassisted pulse with a systolic arterial pressure of $80 mm Hg and pulse pressure of $40 mm Hg lasting for at least 5 minutes. In the postresuscitation period, Downloaded from http://circ.ahajournals.org/ by guest on March 5, 2014 Wenzel et al March 16, 1999 1381 TABLE 2. Hemodynamic Variables at Prearrest and After Return of Spontaneous Circulation (Postresuscitation Phase) Postresuscitation Phase, min Prearrest 5 15 30 60 Early vasopressin 9065 133616 129617 148612 155616 Early epinephrine 10061 Late vasopressin 9563 zzz 13269 zzz 126612 zzz 13069 zzz 13868 Late epinephrine 9766 zzz zzz zzz zzz 10667 10264 6364 7062 6864 HR, bpm MAP, mm Hg Early vasopressin Early epinephrine 9964 Late vasopressin 10666 zzz 95612 zzz 6768 zzz 6264 zzz 6463 Late epinephrine 11168 zzz zzz zzz zzz MPAP, mm Hg Early vasopressin 1862 2062 1962 2262 2162 Early epinephrine 1861 Late vasopressin 1861 zzz 2064 zzz 1963 zzz 2363 zzz 2364 1662 zzz zzz zzz zzz Early vasopressin 14762 7566 5966 7766 10468 Early epinephrine 14869 Late vasopressin 14467 zzz 94621 zzz 58615 zzz 87613 zzz 123610 Late epinephrine 14668 zzz zzz zzz zzz Early vasopressin 1604685 31546249 22636159 19886178 13616122 Early epinephrine 14796180 Late vasopressin 16016181 zzz 24046299 zzz 18316181 zzz 15376191 zzz 11156169 Late epinephrine CI, mL z kg 21 z min 21 SVR, dyne z s z cm25 Late epinephrine 17176182 zzz zzz zzz zzz Prearrest indicates measurements before induction of cardiac arrest; postresuscitation phase, after return of spontaneous circulation; HR, heart rate; MAP, mean arterial pressure; MPAP, mean pulmonary artery pressure; CI, cardiac index; SVR, systemic vascular resistance; . . ., not applicable—no return of spontaneous circulation; early vs late, first drug administration after 3 vs 8 minutes of basic life support CPR, respectively. Values are mean6SEM. hemodynamic parameters were measured at 5, 15, 30, and 60 minutes after return of spontaneous circulation. After the experimental protocol was finished, the animals were killed and necropsied to verify correct positioning of the catheters and injuries to the rib cage. Statistical Analysis The comparability of weight and baseline data were tested with the t test for continuous variables. One-way ANOVA was used to determine statistical significance between groups and was corrected for multiple comparisons by the Bonferroni method. Using Fisher’s exact test, we tested the null hypothesis that the number of surviving animals is independent of treatment. We considered a 2-tailed value of P,0.05 statistically significant. Results Before induction of ventricular fibrillation and before drug administration during CPR, there were no differences in weight, hemodynamic variables, or blood gases between groups (Table 2). When drugs were given early during BLS CPR (after 3 minutes of chest compressions), there was a strong trend toward significantly higher CPP 90 seconds after vasopressin compared with epinephrine. This trend became statistically significant between groups 5 minutes after the first vasopressin or epinephrine administration and remained significantly different for the remainder of the experiment (Figure 1). When drugs were given late during BLS CPR (after 8 minutes of chest compressions), CPP was significantly higher after vasopressin compared with epinephrine at both 90 seconds and 5 minutes after each of 2 drug administrations (Figure 2). After 22 minutes of cardiac arrest, including 18 minutes of CPR, all pigs in the early and late vasopressin group had return of spontaneous circulation (early vasopressin group, 1.360.2 countershocks; late vasopressin group, 4.260.9 countershocks) and survived the 60-minute postresuscitation phase. In the early epinephrine group, 2 animals were defibrillated into pulseless electrical activity, and 4 animals had asystole. In the late epinephrine group, all animals had asystole. Necropsy confirmed appropriate catheter positions and revealed no injuries to the rib cage or intrathoracic organs in any animals. Downloaded from http://circ.ahajournals.org/ by guest on March 5, 2014 1382 Repeated Vasopressin vs Epinephrine During CPR Figure 1. Administration of repeated doses of vasopressin (f) but not epinephrine (l) given early during BLS CPR maintained mean6SEM CPP above the threshold of '20 to 30 mm Hg (dashed lines) that is needed for successful defibrillation with return of spontaneous circulation. DA 1 indicates drug administration of 0.4 U/kg vasopressin vs 45 mg/kg epinephrine; DA 2, 0.4 U/kg vasopressin vs 45 mg/kg epinephrine; DA 3, 0.8 U/kg vasopressin vs 200 mg/kg epinephrine; *P,0.05 vs epinephrine; ROSC, return of spontaneous circulation; VF, ventricular fibrillation; and ACLS, advanced cardiac life support. Time is given in minutes (9) and seconds (0). Discussion Repeated administration of vasopressin but only the first dose of epinephrine given early and late during BLS CPR were able to maintain CPP above the threshold between 20 and 30 mm Hg that is needed for successful defibrillation.22 Furthermore, these effects lasted longer after vasopressin than epinephrine, and significantly more vasopressin than epinephrine animals had return of spontaneous circulation (6 of 6 versus 0 of 6, respectively; P,0.05). The present model closely simulates a short and prolonged duration of BLS followed by advanced cardiac life support. Although the 45-mg/kg dose of epinephrine used in our porcine study is higher than the 15-mg/kg dose recommended for clinical use,14,15 the first dosages of both vasopressin and epinephrine reflect an established optimal dose in this pig model.9,17 Furthermore, the high doses of 0.8 U/kg vasopres- Figure 2. Administration of repeated doses of vasopressin (f) but not epinephrine (l) given late during BLS CPR maintained mean6SEM CPP above the threshold of '20 to 30 mm Hg (dashed lines) that is needed for successful defibrillation with return of spontaneous circulation. Abbreviations and values as in Figure 1. sin and 200 mg/kg epinephrine are the maximum effective doses in swine.9,18 Interestingly, the effects of vasopressin versus epinephrine on CPP varied depending on the time of drug administration during advanced life support CPR. For example, the first vasopressin administration in the late model achieved an '66% increase in CPP over the first vasopressin injection in the early model ('20 mm Hg versus 30 mm Hg). Conversely, the first epinephrine dose in the late model achieved only an '35% increase in CPP over the first epinephrine dose in the early model ('6 mm Hg versus '17 mm Hg). This indicates that the effects of epinephrine given late seemed to be more attenuated compared with late administration of vasopressin during BLS CPR. In fact, arteries from rats with metabolic acidosis or uremia showed selective blunting of biochemical and contractile responses to norepinephrine but not to vasopressin.19 This may suggest that after prolonged cardiac arrest and therefore fundamental global hypoxia and hypercarbic acidosis, the pressor sensitivity to vasopressin may be normal and the effects of catecholamines may be blunted.10 The underlying mechanism for a rapid and profound tachyphylaxis of epinephrine may be desensitized myocardial and peripheral adrenergic receptors.20 Accordingly, substantially elevated plasma levels of epinephrine that are endogenously released immediately after cardiac arrest before initiation of CPR may be a possible explanation for limited effectiveness of epinephrine. This may explain that in addition to endogenous epinephrine, exogenous epinephrine is necessary to increase vital organ blood flow during CPR.21 A CPP between 20 and 30 mm Hg during CPR is one of the best predictors of return of spontaneous circulation in both animals and humans.22 The epinephrine animals reached this level only transiently 90 seconds after the first drug administration given early and late during BLS CPR, whereas CPP in the vasopressin animals was at or above this level for the entire experiment. Accordingly, all vasopressin animals in our study were successfully defibrillated after 22 minutes of cardiac arrest and survived the 60-minute postresuscitation phase, whereas all pigs resuscitated with epinephrine died. The duration of BLS and therefore of suboptimal vital organ blood flow during CPR may have a fundamental impact on resuscitability. For example, the early vasopressin pigs were successfully defibrillated with 1.360.2 countershocks, whereas the late vasopressin pigs needed 4.260.9 defibrillation attempts to achieve return of spontaneous circulation, indicating more severe cardiac ischemia. Only the first of repeated doses of epinephrine in our animals were able to increase CPP above a threshold that renders successful defibrillation likely. Subsequent doses, including a high dosage, were not able to increase CPP above a level that usually correlates with return of spontaneous circulation. This is in good agreement with a preliminary canine study showing that the first dose of epinephrine determined whether the critical CPP needed for return of spontaneous circulation was reached and the animals survived.23 In fact, with the exception of 2 animals in the early epinephrine group that we defibrillated into pulseless electrical activity, all pigs treated with epinephrine had asystole, indicating fundamental depletion of myocardial energy. This Downloaded from http://circ.ahajournals.org/ by guest on March 5, 2014 Wenzel et al may confirm previous results from laboratory investigations demonstrating that epinephrine fueled cardiac oxygen consumption, which subsequently resulted in a severe mismatch of cardiac oxygen delivery versus oxygen consumption during CPR.24 This mechanism may have been an important component in a clinical study, when a total cumulative dose of 15 mg epinephrine was found to best predict 24-hour mortality in patients with out-of-hospital cardiac arrest.25 In fact, the weight-adjusted total epinephrine dose given to our early epinephrine animals was almost identical to this lethal dose ('285 mg/kg versus '215 mg/kg). Subsequently, no epinephrine pig had return of spontaneous circulation despite the absence of underlying disease, such as severe coronary atherosclerotic disease. Thus, if our results can be extrapolated to clinical management of cardiac arrest, they are in strong disagreement with the current guidelines of both the American Heart Association14 and the European Resuscitation Council,15 which recommend “looping” an algorithm of defibrillation– epinephrine– defibrillation while performing CPR if return of spontaneous circulation cannot be achieved. If our explanation of the observed effects in the present experiment is correct, humans with coronary artery disease might have a greater benefit when being resuscitated with vasopressin than with epinephrine. For example, when a 33% stenosis in the mid left anterior descending coronary artery was induced in a porcine model, myocardial perfusion was not diminished during normal physiological conditions, but endocardial blood flow was significantly decreased during CPR.26 Given the fact that irreversible injury of ischemic myocardium was shown to develop as a transmural wave front that started in the subendocardial myocardium and moved progressively toward the subepicardial myocardium in a canine model,27 this mechanism may result in significant complications in the postresuscitation phase, such as fatal arrhythmias. Thus, this may indicate that during CPR in the presence of coronary artery disease, which is very common in humans suffering cardiac arrest, a relatively high CPP may be beneficial to supply appropriate perfusion to the entire myocardium. Accordingly, a vasopressin-mediated CPP that is significantly above the threshold that is actually needed to achieve return of spontaneous circulation in patients with coronary artery disease may represent an additional advantage with regard to resuscitability compared with epinephrine. Effects of CPR management that are beneficial during the resuscitation attempt may result in potentially deleterious effects in the postresuscitation phase, which is a critical time interval between return of spontaneous circulation and longterm survival. For example, a vasopressin-mediated increased systemic vascular resistance has been shown to be an important mechanism to increase vital organ blood flow during CPR,9 but persisting elevated systemic vascular resistance after return of spontaneous circulation may result in cardiac failure. In fact, a reversible depressant effect on myocardial function of pigs resuscitated with vasopressin was observed compared with epinephrine; however, overall cardiovascular function was not critically or irreversibly impaired after the administration of vasopressin.28 Although we did not measure left ventricular pressure pattern velocity in our pigs to determine cardiac contractility after return of spontaneous March 16, 1999 1383 circulation, cardiocirculatory parameters were stable in all animals in the postresuscitation phase. Furthermore, despite repeated administration of vasopressin during CPR, systemic vascular resistance was elevated only for '15 minutes after return of spontaneous circulation. Accordingly, we suggest that vasopressin may be superior to epinephrine to achieve return of spontaneous circulation, whereas catecholamines may be saved for careful titration of hemodynamic variables after successful defibrillation. Some limitations of this study should be noted, including different vasopressin receptors in pigs (lysine vasopressin) and humans (arginine vasopressin), which may result in a different hemodynamic response to exogenously administered arginine vasopressin. However, the circulatory effects of arginine vasopressin, as administered in the present investigation, may be even greater in humans than in pigs. In addition, we did not evaluate vasopressin plasma levels throughout the study. Furthermore, we were not able to assess whether higher return of spontaneous circulation rates as observed in the early and late vasopressin animals might have had a beneficial effect on long-term survival and neurological outcome after return of spontaneous circulation. Also, usage of potent anesthetics may have impaired cardiovascular function and autonomic control. We also used young, healthy pigs that were free of atherosclerotic disease. Furthermore, this study lacks dose-response data; therefore, we are not able to report the minimally effective vasopressin dose. Finally, we purposely omitted defibrillation attempts on starting CPR and immediately after vasopressor administration to study the hemodynamic effects of the study drugs during the resuscitation attempt. In conclusion, repeated administration of vasopressin but only the first epinephrine dose given early and late during BLS CPR maintained CPP above a threshold that is needed for successful defibrillation. Acknowledgments This study was supported in part by science project No. 7280 of the Austrian National Bank; a Dean’s grant for medical school graduates of the Leopold-Franzens-University of Innsbruck, Austria; and the Department of Anesthesia and Intensive Care Medicine, LeopoldFranzens-University of Innsbruck, Austria. We would like to thank Martin Stoffaneller, BS, and Ulrich Achleitner, MS, for skillful assistance in data acquisition and technical expertise. References 1. Ditchey RV, Lindenfeld JA. Failure of epinephrine to improve the balance between myocardial oxygen supply and demand during closed-chest resuscitation in dogs. Circulation. 1988;78:382–389. 2. Nieman JT, Haynes KS, Garner D, Renie CJ, Jagels G, Storm O. Postcountershock pulseless rhythms: response to CPR, artificial cardiac pacing, and adrenergic agonists. Ann Emerg Med. 1986;15:112–120. 3. Tang W, Weil MH, Gazmuri R, Sun S, Duggal C, Bisera J. Pulmonary ventilation/perfusion defects induced by epinephrine during cardiopulmonary resuscitation. Circulation. 1991;84:2101–2107. 4. Tang W, Weil MH, Sun S, Noc M, Yang L, Gazmuri R. Epinephrine increases the severity of postresuscitation myocardial dysfunction. Circulation. 1995;92:3089 –3093. 5. Woodhouse SP, Cox S, Boyd P, Case C, Weber M. High dose and standard dose adrenaline do not alter survival, compared with placebo, in cardiac arrest. Resuscitation. 1995;30:243–249. 6. Callaham M, Madsen CD, Barton CW, Saunders CE, Pointer J. A randomized clinical trial of high-dose epinephrine and norepinephrine vs Downloaded from http://circ.ahajournals.org/ by guest on March 5, 2014 1384 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. Repeated Vasopressin vs Epinephrine During CPR standard-dose epinephrine in prehospital cardiac arrest. JAMA. 1992;268: 2667–2672. Stiell IG, Hebert PC, Weitzmann BN, Wells GA, Ramann S, Stark RM, Higginson LA, Ahuja J, Dickinson GE. High-dose epinephrine in adult cardiac arrest. N Engl J Med. 1992;327:1045–1050. Lindner KH, Ahnefeld FW, Prengel AW. A comparison of standard and high-dose adrenaline in the resuscitation of asystole and electromechanical dissociation. Acta Anaesthesiol Scand. 1991;35:253–256. Lindner KH, Prengel AW, Pfenninger EG, Lindner IM, Strohmenger HU, Georgieff M, Lurie KG. Vasopressin improves vital organ blood flow during closed-chest cardiopulmonary resuscitation in pigs. Circulation. 1995;91:215–221. Wenzel V, Lindner KH, Prengel AW, Maier C, Voelckel W, Lurie KG, Strohmenger HU. Vasopressin improves vital organ blood flow after prolonged cardiac arrest with post-countershock pulseless electrical activity in pigs. Crit Care Med. In press. Prengel AW, Lindner KH, Keller A. Cerebral oxygenation during cardiopulmonary resuscitation with epinephrine and vasopressin in pigs. Stroke. 1996;27:1241–1248. Lindner KH, Prengel AW, Brinkmann A, Strohmenger HU, Lindner IM, Lurie KG. Vasopressin administration in refractory cardiac arrest. Ann Intern Med. 1996;124:1061–1064. Lindner KH, Dirks B, Strohmenger HU, Prengel AW, Lindner IM, Lurie KG. A randomized comparison of epinephrine and vasopressin in patients with out-of-hospital ventricular fibrillation. Lancet. 1997;349:535–537. Emergency Cardiac Care Committee and Subcommittees, American Heart Association. Guidelines for cardiopulmonary resuscitation, III: adult advanced cardiac life support. JAMA. 1992;268:2199 –2241. Robertson C, Stehen P, Adgey J, Bossaert L, Carli P, Chamberlain D, Dick W, Ekstrom L, Hapnes SA, Holmberg S, Juchems R, Kette F, Koster R, de Latorre FJ, Lindner K, Perales N. The European Resuscitation Council guidelines for adult advanced life support: a statement from the working group on advanced life support, and approved by the executive committee of the European Resuscitation Council. Resuscitation. 1998; 1998:37:81–90. Idris AH, Becker LB, Ornato JP, Hedges JR, Bircher NG, Chandra NC, Cummins RO, Dick WF, Ebmeyer U, Halperin HR, Hazinski MF, Kerber RE, Kern KB, Safar P, Steen PA, Swindle MM, Tsitlik JE, von Planta I, von Planta M, Wears RL, Weil MH. Utstein-style guidelines for uniform reporting of laboratory CPR research. Circulation. 1996;94:2324 –2336. 17. Lindner KH, Ahnefeld FW, Bowdler IM. Comparison of different doses of epinephrine on myocardial perfusion and resuscitation success during cardiopulmonary resuscitation in a pig model. Am J Emerg Med. 1991; 9:27–31. 18. Brown CG, Werman HA, Davis EA, Hobson J, Hamlin RL. The effects of graded doses of epinephrine on regional myocardial blood flow during cardiopulmonary resuscitation in swine. Circulation. 1987;75:491– 497. 19. Fox AW, May RE, Mitch WE. Comparison of peptide and nonpeptide receptor-mediated responses in rat tail artery. J Cardiovasc Pharmacol. 1992;20:282–289. 20. Insel PA. Adrenergic receptors: evolving concepts and clinical implications. N Engl J Med. 1996;334:580 –585. 21. Paradis NA, Martin GB, Rosenberg J, Rivers EP, Goetting MG, Appleton TJ, Feingold M, Cryer PE, Wortsman J, Nowak RM. The effect of standard- and high-dose epinephrine on coronary perfusion pressure during prolonged cardiopulmonary resuscitation. JAMA. 1991;265: 1139 –1144. 22. Kern KB, Niemann JT. Coronary perfusion pressure during cardiopulmonary resuscitation. In: Paradis NA, Halperin HR, Nowak RM, eds. Cardiac Arrest: The Science and Practice of Resuscitation Medicine. Baltimore, Md: Williams & Wilkins; 1996:270 –285. 23. Cairns CB, Niemann JT. Hemodynamic effects of repeated doses of epinephrine after prolonged cardiac arrest and CPR: preliminary observations in an animal model. Resuscitation. 1998;36:181–185. 24. Ditchey RV. The choice of vasopressor agents in cardiopulmonary resuscitation. Curr Opin Crit Care. 1996;2:170 –175. 25. Rivers EP, Wortsman J, Rady MY, Blake HC, McGeorge FT, Buderer NM. The effect of the total cumulative epinephrine dose administered during human CPR on hemodynamic, oxygen transport, and utilization variables in the postresuscitation period. Chest. 1994;106:1499 –1507. 26. Kern KB, Ewy GA. Minimal coronary stenoses and left ventricular blood flow during CPR. Ann Emerg Med. 1992;21:1066 –1072. 27. Reimer KA, Lowe JE, Rasmussen MM, Jennings RB. The wavefront phenomenon of ischemic cell death, I: myocardial infarct size vs duration of coronary occlusion in dogs. Circulation. 1977;56:786 –794. 28. Prengel AW, Lindner KH, Keller A, Lurie KG. Cardiovascular function during the postresuscitation phase after cardiac arrest in pigs: a comparison of epinephrine versus vasopressin. Crit Care Med. 1996;24: 2014 –2019. Downloaded from http://circ.ahajournals.org/ by guest on March 5, 2014