Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
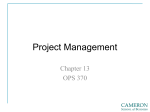
PERT Activations Per Annum 25 20 18 This chart shows all activations of the PERT program from its inception in October 2012 through December 2014 (FY13—early FY15). This encompasses 351 total activations over 26 months. Utilization of PERT has consistently exceeded 18 17 17 15 14 expectations, confirming an underlying need for such a rapid response service to treat patients with pulmonary embolism. 20 19 10 10 13 12 6 5 13 13 11 10 5 4 17 14 12 8 6 17 13 10 0 OCT Source: Massachusetts General Hospital PERT program. NOV DEC JAN FEB MAR APR MAY JUN FY13 FY14 JUL AUG SEPT FY15 101 Merrimac Street, Suite 200 Boston, MA 02114 NON-PROFIT ORG. U.S. POSTAGE PAID MASSACHUSETTS GENERAL HOSPITAL An Interdisciplinary Approach to the Treatment of Pulmonary Embolism INSIDE > > A long-term evaluation of patient outcomes will promote evidencebased treatment protocols Rapid response team offers a coordinated institutional approach across specializations For More Information ( 617-724-7739 8 [email protected] massgeneral.org/PERT Pulmonary Embolism Rapid Response Team (PERT) Computed tomography (CT) scans showing a clot in the main pulmonary trunk extending to both main pulmonary arteries that obstructs blood flow to the lungs (left), and a cross-section of a clot (arrow) in the right ventricle indicating that there is still a clot “in transit,” migrating through the heart chambers toward the pulmonary arteries (right). Pulmonary emboli (PE) are the most common reason for in-hospital deaths in the U.S., occurring at a rate of more than 100,000 per year. Yet optimal treatment has not been systematically studied. Up to 30 percent of PE have high-risk features: hemodynamic instability, right ventricular dysfunction, or evidence of myocardial necrosis. About 10 percent of PE are fatal within an hour of the onset of symptoms; untreated cases have a 30 percent mortality rate.1 A major hindrance in improving Channick, MD, director of the Pulmonary Hypertension Program and an expert outcomes is that patients may present in many hospital departments, and treatment in chronic PE; Christopher Kabrhel, MD, MPH, director of the Center for Vascular decisions are determined by clinical expertise and medical or surgical resources Emergencies in the Department of Emergency Medicine; and Rachel Rosovsky, MD, in that department, without a unified, evidence-based approach. In October 2012, an expert in clotting disorders. Massachusetts General Hospital initiated a multidisciplinary rapid response program PERT incorporates treatment perspectives from specialists in cardiology, called PERT, for Pulmonary Embolism Response Team, a collaboration focused on cardiothoracic surgery, echocardiography, emergency medicine, hematology, improving the care of patients with massive or submassive pulmonary embolism. This pulmonary/critical care, radiology, and vascular medicine and intervention. After initiative will also collect data on outcomes in order to enhance knowledge about PE two years, PERT team members report a more coordinated institutional approach and to better inform therapeutic decisions in the future. to this highly prevalent, life-threatening disease, with treatment tailored to the PROMOTING AN EVIDENCE-BASED APPROACH individual patient, based on degree of hemodynamic and cardiopulmonary instability as well as other parameters. Treatment decisions for PE include both existing therapies and novel approaches. Longer term, PERT is enabling the systematic evaluation of multiple approaches Open surgery to remove the clot is one of many treatment alternatives; others and techniques that will promote scientific learning and evidence-based research. include anticoagulation, systemic intravenous thrombolysis, locally delivered To advance the science of PE care, PERT is developing treatment protocols and thrombolytics, thrombo-aspiration and mechanical thrombectomy. Each of these is maintaining a robust registry of patients, with a database of treatments and strategies has the potential to improve patient outcomes. Comparative data outcomes. The program has begun a multidisciplinary follow-up clinic to collect regarding which therapy is best for a given patient with PE, however, is sparse, and long-term patient outcomes and is planning further studies. 2 existing guidelines provide only general advice. To address the need to streamline complex treatment decisions about individual PERT ACTIVATION AND OUTREACH patients while incorporating expertise from multiple disciplines, a Mass General team PERT is activated by a single phone call from any referring physician within Mass coalesced to create PERT. This initiative, which involves more than seven departments General. Following a "rapid response" consultation, an online meeting of the that share a common interest in PE, has been led by Kenneth Rosenfield, MD, section multidisciplinary team is convened. Team members discuss the case and treatment head for Vascular Medicine and Intervention; Michael Jaff, DO, director of the MGH options while reviewing radiographic images, lab results and clinical notes in Fireman Vascular Center, an expert in deep vein thrombosis and lead author of the real time. Referring physicians often participate in the discussion. After reaching AHA guidelines document on the subject of PE; Thoralf Sundt, MD, chief of cardiac consensus regarding the best response, the PERT system activates appropriate surgery and co-director of the MGH Corrigan Minehan Heart Center; Richard hospital resources to rapidly implement an integrated care plan. Finally, in response to the interest that PERT has generated among physicians around the country, the Mass General team is forming a collaborative national PERT Activations, October 2012 Launch–December 2014 The most common treatment after PERT activation by consensus was anticoagulation alone (60.7%). Other procedures were also provided. Long-term outcome data will enable increasingly informed decisionmaking. Source: Massachusetts General Hospital PERT program. network of Pulmonary Embolism Response teams. That consortium, to be 293 INTERVENTIONS: 60.7% Anticoagulation only 20.8% IVC filters 8.7% Catheter-direct thrombolysis 4.0% Surgery 2.7% IV lysis 2.3% ECMO launched at a spring 2015 meeting at MGH, will provide further opportunities to evaluate new treatment algorithms and ideas arising from PERT’s coordinated multidisciplinary program. PERT leaders are committed to advancing the field more rapidly to benefit patients. ■ 1 P rovias, Tim, David M. Dudzinski, Michael R. Jaff, Kenneth Rosenfield, Richard Channick, Joshua Baker, Ido Weinberg, et al. “The Massachusetts General Hospital Pulmonary Embolism Response Team (MGH PERT): Creation of a Multidisciplinary Program to Improve Care of Patients with Massive and Submassive Pulmonary Embolism.” Hospital Practice (1995), February 2014, 42 (1) : 31–37. 2 J aff, Michael R., M. Sean McMurtry, Stephen L. Archer, Mary Cushman, Neil Goldenberg, Samuel Z. Goldhaber, J. Stephen Jenkins, et al. “Management of Massive and Submassive Pulmonary Embolism, Iliofemoral Deep Vein Thrombosis, and Chronic Thromboembolic Pulmonary Hypertension: A Scientific Statement from the American Heart Association.” Circulation, no. 16 (April 26, 2011): 1788–1830. 0.7% Vortex MALE: 56.1% FEMALE: 43.9% AGE RANGE: 10–98 yrs., median 62 yrs. SURVIVAL TO DISCHARGE: 85.3%