Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiopulmonary Resuscitation
Tony Johnson, DVM, DACVECC
Clinical Assistant Professor
Veterinary Information Network & Purdue University School of Veterinary Medicine
Davis, CA & West Lafayette, IN, USA
{3 Rivers Conference Nov 2016}
KEY POINTS:
In people, post arrest/CPR has a discharge rate of 17%.
In veterinary patients the discharge rate is only 6-9%.
Ventilation at 10 breaths/minute
Chest compressions at 100/minute in lateral; recumbency
Epinephrine: 0.1ml/20lb
Atropine: 1ml/20lb
The RECOVER study:
•
Over 100 boarded veterinary specialists
•
74 specific CPR-related clinical questions
•
101 individual clinical guidelines in the study in 5 domains
Cardiopulmonary arrest (CPA), to be successfully reversed, requires prompt identification and
reaction of a well-coordinated team with availability of appropriate equipment.
Cardiopulmonary resuscitation is frequently unsuccessful. As few as 4.1% of dogs and 9.6% of
cats that suffer CPA are discharged from the hospital alive. Because of these poor odds it is
obvious that prevention of cardiopulmonary arrest is more desirable than treatment once the
arrest has occurred. Prevention requires close monitoring of critical patients, patients under
anesthesia, and those patients for which there is a high index of suspicion that CPA could occur.
Familiarity with those clinical conditions which are considered risk factors is important as well
as noting clinical signs that would potentially precede the occurrence of CPA.
In spring of 2012 the American College of Veterinary Emergency and Critical Care (ACVECC)
released the results of a large study - the Reassessment Campaign on Veterinary Resuscitation,
or the RECOVER study. Results are available free to all veterinarians through:
http://www.acvecc-recover.org/
This landmark study offers evidence based recommendations for performing CPR in veterinary
patients. It’s findings have been incorporated into the notes below.
Key Points from the RECOVER Study:
Primary respiratory arrest is more common in small animals than in
people, and early intubation and ventilation at 10 breaths/minute are important
Chest compressions at 100/minute in lateral recumbency are preferable.
1
In flatter chested dogs like English/French bulldogs compressions in dorsal
recumbency may be most effective.
Risk factors:
Cellular hypoxia
Hypercarbia
Vagal stimulation
Arrhythmias
Severe Anemia
Sepsis/SIRS
Cardiac failure
Neoplasia
Acid-base abnormalities
Electrolyte abnormalities
Anesthesia
Trauma
Coagulopathies
Toxicities
Pulmonary disease
Traumatic brain injury
Warning signs:
Changes in mental status, obtundation
Changes in respiratory depth, rate or rhythm
Weak irregular pulses
Bradycardia (usually nonresponsive to atropine)
Hypotension
Cyanosis
Hypothermia
Unfortunately, even with the best of preventative medicine and diligent monitoring CPA is
bound to occur particularly in settings such as intensive care units that are dealing with the most
critical patients. In a situation where the outcome is usually not very good, creating the best
possible circumstance to provide optimal care and increase the chances of success is important
and includes the following: prompt recognition of the arrest in a patient, a clear understanding
of which patients are to receive CPR, a designated prepared area for CPR to take place,
availability of the necessary equipment (well stocked crash cart), a clear understanding of the
procedures involved in CPR and an educated and informed support team.
Clinical recognition of arrest:
Loss of consciousness
Pupils dilated and unresponsive
LOSS OF SPONTANEOUS VENTILATION
NO PALPABLE PULSES OR AUSCULTABLE HEART SOUNDS
Who should be resuscitated?
Every patient admitted to the hospital should receive a code status. This is something that should
be discussed with owners at the time of admission. Clients should be given the benefit of the
doctor’s knowledge and provided with as much information as possible to assist them in deciding
upon a code status for their pet. The owner’s wishes should be clearly indicated in the hospital
record. The most common code status that denotes a patient which is not to receive CPR is DNR
(Do Not Resuscitate). Owners may choose this status for their pet for one of several reasons, for
example the pet with terminal disease, financial constraints or religious or philosophical beliefs.
2
Remember this should always be discussed with the owner and ultimately it is their decision. If
a client chooses to have resuscitation attempted should their pet suffer CPA it is important that
the client have appropriate expectations and be informed as performing CPR does not guarantee
successful return of spontaneous circulation or ventilation and discharge from the hospital. CPR
efforts are generally discontinued based on the patient’s disease process, the prognosis, the
client’s desires or if after 20 minutes CPR efforts are still unsuccessful.
Readiness:
Requires adequate personnel
Team effort (ideally a minimum of 3 people)
Requires appropriate equipment
Oxygen source (100%)
Appropriately stocked crash cart
Wound pack
Suction unit
Appropriate monitoring equipment
Personnel responsibilities:
Central person making decisions (DVM)
Chest compressions
Manual ventilation
Drug administration
Setting up monitoring equipment
Recording events
Crash Cart: A crash cart should be readily available, mobile, inventoried and missing items
replaced on a regular basis. The crash cart should be sealed or taped closed until such time that it
is necessary for use during the CPA of a patient. A well stocked crash cart will contain the
following:
Cuffed endotracheal tubes of various sizes
Laryngoscope
Gauzes
Syringes and needles of various sizes
Catheters: intravenous, intraosseous, red rubber
Defibrillator
Thoracocentesis set up
Small surgery pack, appropriate retractors (for open chest CPR)
Drugs: epinephrine, atropine, vasopressin, lidocaine, calcium gluconate
Basic Life Support: The ABC’s of CPR
Airway:
Check the airway and clear of any debris or objects causing obstruction. Suction airway to clear
mucous or fluid if necessary. A laryngoscope should always be utilized for placement of the
3
endotracheal tube to improve ease of placement, improve efficiency and avoid vagal induced
bradycardia from excessive manipulation of the epiglottis. Evaluation of appropriate chest
excursions during ventilation can also add to confidence of proper placement.
Breathing:
Utilization of an ambu bag or rebreathing bag connected to an anesthetic machine with the
inhalant anesthetic turned off. A source of 100% oxygen should be used while providing manual
positive pressure ventilatory support. All breaths should be given over 1-2 seconds duration with
sufficient volume to cause a visual rise in the chest wall, and then allow normal relaxation of the
chest wall. Pressures should not exceed 20cm H2O.
Rate: 10 breaths per minute
Circulation:
External chest compressions:
Chest compressions are utilized to promote forward flow of blood when the heart is not working.
Rate of compressions for veterinary patients (dogs and cats) is 100 compressions per minute.
Compressions should be delivered with a 1:1 compression to relaxation ratio (compression time
should equal relaxation time.) It is very important to allow adequate recoil of the thoracic wall
after compression. It is during this time period that blood returns to the heart (venous return).
Inadequate relaxation or recoil of the thoracic wall results in decreased venous return. Chest
compressions should be continuous with no pauses during administration of ventilatory breaths,
placement of IV catheters, endotracheal intubation, ECG assessment, palpation of pulses, or
administration of medications. To maintain the most efficient and effective compressions the
person administering chest compressions should be changed every 2 minutes.
Positioning: Patients should be placed in lateral recumbency on a firm surface. Ideally the
person administering chest compressions should be above the patient’s chest. In medium and
large dogs the hands should be positioned over the widest part of the patient’s thorax with one
hand on top of the other with the fingers interlocked, the hands should be parallel to the chest
wall. Even pressure should be applied to the thoracic wall with each compression from the palm
of the hand. For smaller patients (<7kg), the fingers of one hand should be placed on one side of
the thorax and the thumb on the other side. The flats of the fingers should be used to perform
compressions, the fingertips should be avoided.
Open Chest CPR (Internal cardiac massage):
Indications for open chest CPR include:
Thoracic wall defects or trauma
Pleural space disease
Diaphragmatic hernia
Pericardial effusion/fluid
No response to close chest CPR after 2 to 5 minutes
Chest or abdominal surgery
Hemoperitoneum
4
Basic approach to open chest CPR: With the patient in right lateral recumbency a skin incision
is made over the left fifth or sixth intercostal space, extending dorsally from the origin of the ribs
to ventrally near the sternum. A rapid clip in a long haired dog may facilitate the skin incision.
A curved Mayo scissors is used to complete the thoracotomy. Positive ventilation should be
temporarily interrupted during the penetration into the pleural space and opening of the
intercostal space to avoid trauma to the lungs. The tips of the closed scissors are thrust through
the intercostal muscle and into the pleural space ventrally near the costochondral junction. The
scissors are used in a sliding fashion to open the intercostal space. The incision is then extended
ventrally. Ventral to the costochondral junction, the scissors are centered between the ribs to
avoid the intercostal vessels that lie on the cranial and caudal edges of the ribs. The incision
should stop short of the sternum to avoid injury to the internal thoracic artery and vein, which
course longitudinally approximately 1 cm from the sternum. A Balfour abdominal retractor or a
Finochietto rib spreader can be used to improve visualization and access to the heart and
pericardium.
After successful resuscitation, the patient should be taken to the operating room for copious
irrigation and routine closure.
Advanced Life Support: The ABC’s plus D and E:
Advanced life support extends the scope of CPR beyond just the ABC’s and includes D and E;
drugs, defibrillation, ECG analysis and other techniques that have the potential to increase the
chance of success. Initiation of drug therapy allows for additional support of basic life support
techniques. ECG analysis provides the opportunity to further tailor interventions based on the
rhythm present, while defibrillation provides the only effective method of managing ventricular
fibrillation and is also indicated in patients with pulse less ventricular tachycardia.
Drugs:
Epinephrine is a mixed adrenergic agonist, acting on α and ß receptors. It is primarily
used during CPR for its α2-adrenergic receptor stimulating effects, including peripheral arteriolar
vasoconstriction, which leads to increased coronary and cerebral perfusion pressure. See the
table for dosage administration recommendations. Epinephrine administration should be
repeated every 3 to 5 minutes if indicated. If repeated doses are not successful, vasopressin can
be administered instead or the dose of epinephrine can be increased to 0.1mg/kg. Many
protocols in human medicine now call for 1 dose of epinephrine, followed by a dose of
vasopressin IV before repeating or increasing the dose of epinephrine. See table 1 for dosing.
Most recommendations are for 0.1ml per 20lb of the 1:1000 (1mg/ml) preparation.
Atropine is an anticholinergic parasympatholytic that is effective at muscarinic receptors.
Atropine reverses the cholinergic-mediated responses and parasympathetic stimulation and acts
to increase heart rate, control hypotension, and increase systemic vascular resistance. As a
vagolytic, it is most effective in the treatment of vagal-induced asystole. See table 1 for
recommended dosage. Most recommendations are for 1ml per 20lb of the 0.54mg/ml
formulation. If there is no effect after initial administration the dose can be repeated every 3-5
minutes for a maximum of 3 doses.
5
Vasopressin is a nonadrenergic endogenous pressor peptide that causes peripheral,
coronary, and renal vasoconstriction. In humans with asystole, vasopressin was superior to
epinephrine in survival to discharge from the hospital in some studies and it is recommended in
the treatment of asystole based on the 2005 guidelines. As a result of this data and because
asystole is the most common arrest rhythm in veterinary patients, the use of vasopressin is
increasing in companion animals. The recommended dose for vasopressin administration is 0.20.8 U/kg IV.
Sedatives and anesthetics:
If CPA is associated with or occurs during anesthesia the anesthetic should be discontinued
immediately. Reversal agents for any sedative drugs previously given should be reversed if
warranted.
ECG (electrocardiograph): Monitoring the ECG during CPR allows for assessment of the
electrical activity and possible response to therapy. There are 3 common cardiac arrest rhythms
that may occur.
Asystole: is the most common arrest rhythm in veterinary patients (dogs and cats).
Therapy for asystole is aimed at performing “high quality” CPR with minimal
interruptions and identifying and treating the underlying cause. Although studies have
not identified any drugs that are consistently effective in treating asystole, atropine and
epinephrine are most often administered. Vasopressin has demonstrated some promise in
recent studies when treating asystole in humans.
Pulseless Electrical Activity (PEA): (Previously referred to as electromechanical
dissociation: EMD). PEA is a rhythm in which, despite the possibly normal appearance
of the rhythm on ECG, there is actual absence of myocardial contraction. As with
asystole no medications have proven to be consistently effective however atropine and
epinephrine are often administered. The focus should be on performing high quality
CPR, identifying and treating the underlying cause.
Ventricular fibrillation: is unorganized ventricular excitation resulting in poorly
synchronized and inadequate myocardial contractions that cause cardiac pump failure.
The recommended treatment for this rhythm is defibrillation.
Defibrillation: is defined as termination of ventricular fibrillation for at least 5 seconds
after delivery of an electric shock that depolarizes myocardial cells and eliminates
ventricular fibrillation. Chest compressions should be continued while the defibrillator is
being connected and charged. Conductive gel should be used on the electrode paddles.
Alcohol, ultrasound gel or other nonconductive gels should not be used on the electrode
pads. The patient should be placed in dorsal recumbency and the paddles should be
placed with pressure on opposite sides of the chest. Once the defibrillator is charge, the
patient and paddles are positioned appropriately the word “clear” should be shouted out
to warn personnel to cease any contact with the patient and anything connected to the
patient. The person administering the shock should avoid contact with the patients limbs,
6
the table, the ECG leads and everything connected to the patient. See the table 1 for the
appropriate recommended energy level that should be administered.
Chest compressions should be immediately resumed for 2 minutes before reassessing the
cardiac rhythm and administration of an additional shock. Resuming chest compressions
immediately after administration of a shock increases myocardial perfusion and increases
the chances of successful conversion.
IV Fluids: IV fluids should be administered if the patient is hypovolemic. IV fluids should not
be administered at shock dosages unless the patient was hypovolemic before the CPA. In the
euvolemic CPA patient, the recommended dosage for crystalloid IV fluids is a 20ml/kg bolus for
dogs and 10ml/kg bolus for cats, as rapidly as possible. The administration of excessive volumes
of IV fluids to euvolemic patients during CPR in animal studies decreased coronary perfusion
pressure because of an increase in the right atrial pressure relative to aortic pressure.
If colloids are necessary the IV dosage for hetastarch or plasma is 20ml/kg/day for dogs and 510ml/kg/day for cats. Colloids can be administered as a bolus at 5ml/kg for dogs and 2-3ml/kg
for cats. These dosages may require adjustments up or down based on the individual case.
End tidal CO2 monitor usage during CPR can aid in assessing the effectiveness of CPR effort.
The ETCO2 level should be monitored as an indication of perfusion. If ventilation during CPR
is relatively constant, changes in cardiac output are reflected by changes in ETCO2 levels. In
studies of humans patients who could not be resuscitated had significantly lower ETCO2 levels
than those who were successfully resuscitated.
Doppler unit can be used to aid in assessing cerebral blood flow during CPR by placing a well
lubricated transducer crystal on the cornea.
Post-Resuscitation care: Post CPR care is aimed at preserving cerebral blood flow, improving
hemodynamics, maximizing O2 delivery and minimizing damage from secondary changes (freeradicals, increased intracranial pressure, Ca++ release, etc). Monitoring parameters include:
pulse, EKG, blood pressure, body To, urine production, blood gasses and electrolytes, and
neurological status. In many ways, post-CPR care is similar to management of head-injured
patients. Prevention of hypoxia and hypotension are critical!
Neurological status: Constricted pupils and pupillary light responses are favorable neurologic
indicators, but atropine administration during CPR may alter PLR’s. Non-responsive, dilated
pupils are a grave prognostic sign. Seizure activity is common after successful CPR, but is not
necessarily associated with a poor outcome unless status epilepticus develops. Patients who are
alert within 12 hours of arrest generally recover favorably.
Blood pressure: Mild hypertension is common for 1-5 minutes after CPR, but blood pressure
usually falls rapidly. Pressors such as dopamine and dobutamine, in combination with fluids,
colloids and hypertonic saline can all be used to maintain mean arterial blood pressure at
~90mmHg. Fluids generally should be run at 1.5 times maintenance unless volume overload is a
concern. IF CVP is being monitored, it should be maintained between 5-12cm H2O. Since
perfusion of the brain depends on blood pressure overcoming increased pressures within the
skull, any drop in systemic blood pressure is detrimental.
7
Oxygenation: Normal oxygenation should be maintained and monitored by serial blood gasses.
Oxygen can be administered via facemask, endotracheal tube, nasal insufflation etc. PaO2 of
about 100mmHg and PaCO2 of 30-40mmHg are normal. Assisted ventilation may be required.
Intracranial pressure: Since monitoring is not feasible, it can be assumed that ICP will be
elevated after CPR. Mannitol can be administered (0.5-2gm/kg) to osmotically decrease
intracranial swelling, but the old “dry out the brain” theory has bitten the dust recently, in favor
of increasing cardiac output to overcome elevated ICP. Hypertonic saline and pressors can also
be used for this purpose. Controlled ventilation to maintain a lowPaCO2 may help. Uncontrolled
elevations in ICP may be indicated by a drop in heart rate (Cushing’s response). The head
should be elevated (30o angle) and the neck extended. Compression of the jugular veins should
be avoided.
Other steps:
Steroids: No proven benefit.
Consider furosemide for pulmonary contusions and elevated ICP - controversial.
Turn Q 3-4 hours to prevent atelectasis and decubital ulcers.
Provide padded bedding and a quiet environment.
Analgesia and sedation as needed.
Dedicated technician monitoring
Airway care: tracheostomy tube care, airway secretion suctioning.
Corneal lubrication.
Monitor urine output (Normal is 1-2 ml/kg/hr)
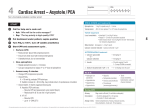
Table 1. Reprinted from www.ACVECC-RECOVER.org
8