Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
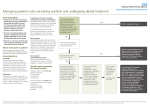
VTE Management Toolkit Objective The VTE Management Toolkit is designed as a practical resource for physicians and other healthcare professionals to facilitate the safe and efficient management of acute venous thromboembolism (VTE). This toolkit also aims to support the education of patients. Target groups This VTE Management Toolkit primarily targets the following health care professionals: ER physicians Hospitalists General internists Family physicians Pharmacists Background The VTE Management Toolkit is a succinct package of information designed for clinicians, hospitals and patients to aid in the appropriate management of acute VTE. This toolkit was developed in response to the need for evidence-based and practical guidance when making clinical decisions about VTE management. This toolkit is comprised of the following components: background information about the epidemiology and complication rates of deep vein thrombosis (DVT) and pulmonary embolism (PE) care pathways to aid in the baseline assessment of patients with acute VTE and selection of appropriate anticoagulation a sample order set, discharge checklist, monitoring algorithm patient information handouts approaches to management of anticoagulant-associated bleeding algorithms for periprocedure management of anticoagulated patients Adaptability Each component of the toolkit can be easily modified for local use. Sections that are not relevant to your institution can be deleted. Authors This toolkit was compiled and reviewed by a group of physicians, pharmacists, and nurses specializing in Thromboembolic disorders at Sunnybrook Health Sciences Centre. The creation of this toolkit is in accordance with the Thromboembolism and Anticoagulant Management at Sunnybrook (TEAMS) program objectives. We welcome questions, suggested edits and enhancement of the toolkit. Table of Contents Introduction to VTE........................................................................................... Care pathway for management of acute VTE.................................................. Admission criteria for acute VTE...................................................................... Assessment of bleeding risk............................................................................. Acute DVT/PE order set................................................................................... Discharge prescription..................................................................................... Discharge checklist.......................................................................................... Anticoagulant Dosing Record.......................................................................... Pathway for long-term management of VTE: Follow-up and monitoring.......... Patient Information Forms: Venous thromboembolism (VTE) ....................................................... Rivaroxaban......................................................................................... Low molecular weight heparin (LMWH) .............................................. Subcutaneous injection technique...................................................... Warfarin................................................................. .............................. Management of bleeding in a patient receiving rivaroxaban.......................... Management of bleeding in a patient receiving warfarin................................. Periprocedure management of rivaroxaban.................................................... Periprocedure management of LMWH............................................................. Periprocedure management of warfarin.......................................................... 1 2 3 3 4 6 7 8 9 11 13 14 15 16 18 19 20 21 22 Introduction to VTE Venous thromboembolism (VTE), which includes deep vein thrombosis (DVT) and pulmonary embolism (PE), is a common cause of morbidity and mortality. It is estimated that VTE affects 1 to 3 per 1000 persons in the general population every year1. Among patients with a diagnosis of DVT, more than half will already have PE and 30-50% will develop post-thrombotic syndrome. PE can be rapidly fatal and a small proportion of patients develop thromboembolic pulmonary hypertension. Anticoagulant therapy dramatically reduces the incidence of recurrent VTE from approximately 25% to 3% during the first 6-12 months of therapy1. The latest American College of Chest Physicians (ACCP) 2012 guidelines recommend 3 main treatment options for acute DVT/PE2: 1. Low molecular weight heparin (LMWH) bridged to warfarin maintenance therapy 2. rivaroxaban (Xarelto®) 3. LMWH alone The traditional approach to the management of acute VTE is to initiate a LMWH for the first 5 to 10 days of therapy while bridging to therapeutic warfarin. Evidence has recently emerged to support an additional first line option for treatment of VTE. Rivaroxaban (Xarelto®) is an oral direct factor Xa inhibitor that has demonstrated non-inferiority to the traditional approach of LMWH bridged to warfarin in the EINSTEIN-DVT and EINSTEIN-PE studies3,4. The third option is to continue on a LMWH alone for the duration of anticoagulant therapy, particularly in patients with active malignancy, pregnancy, or anticipated short duration of therapy2. Treatment duration is generally 3 months in patients with provoked VTE when the inciting factor has resolved2. Duration should be extended and, in some cases, should be indefinite for patients at higher risk of recurrence including those with unprovoked VTE or those with ongoing major risk factors. 1 References: 1. Van Es J, Kamphuisen PW, Buller HR. How to prevent, treat, and overcome current clinical challenges of VTE. J Thromb Haemost 2011;9 (Suppl. 1):265-274. 2. Kearon C, et al. Antithrombotic Therapy for VTE Disease. ACCP 2012 guidelines. CHEST 2012; 141;2 (supplement): e419S-e496S. 3. Bauersachs, et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med 2010;363:2499-2510. 4. Buller HR, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med 2012;366:1287-1297 Continued on next page….. 2 Care Pathway for the management of acute VTE Patient with Confirmed Acute DVT/PE Consider criteria for hospital admission (see next page) Assess bleeding risk (see next page) Is LMWH alone the most appropriate choice? Patient Characteristics: Pregnancy Active malignancy High bleeding risk Baseline Assessment CBC, PT, PTT, creatinine clearance, LFTs, Consider rivaroxaban OR warfarin Contraindications? AND AND Favours rivaroxaban* Favours bridging to warfarin* Patient preference Unable/unwilling to undergo subcutaneous injections and/or INR testing + Normal renal and liver function + Expected good compliance + Willingness to pay No history of HIT1 Severe renal dysfunction (CrCl<30mL/min) ↓ LMWH dose or bridge with unfractionated heparin Important drug-drug interaction with rivaroxaban (see order set) Expected low compliance Unable to pay for rivaroxaban No severe renal dysfunction YES LMWH* Prepare for Discharge (see Discharge checklist) Follow-up (Adherence, thrombosis symptoms, bleeding, questions answered) Arrange patient contact the day after start of treatment Physician appointment e.g. in 1-3 weeks and 3 months Monthly monitoring checks: via phone/text messages/email *See dosing options in Order sets 1HIT= heparin-induced thrombocytopenia 3 Admission Criteria for Acute VTE Most patients with acute VTE do not require hospital admission Below are criteria to consider when deciding if a patient requires admission to hospital: PE DVT Hemodynamically unstable Very high bleeding risk Requires supplement O2 or parenteral narcotics Severe renal dysfunction Catheter thrombolysis Very high bleeding risk Severe renal dysfunction Assessment of Bleeding Risk Absolute contraindications to anticoagulation: Current active bleeding Heparin-induced thrombocytopenia (contraindication for heparin and LMWH) Pregnancy (for warfarin, rivaroxaban) Severe renal failure—CrCl ≤ 30 mL/min (for rivaroxaban; avoid or lower dose of LMWH) Risk factors that increase the risk of bleeding with therapeutic anticoagulation: (patients with these risk factors require a careful assessment of thrombosis and bleeding risks) Recent major bleeding Recent intracranial bleeding Recent GI bleeding Major coagulopathy Severe thrombocytopenia Advanced age Moderate renal dysfunction (CrCl 30-50 mL/min) Severe liver dysfunction Concomitant use of platelet inhibitor Alcoholism, drug abuse 4 Acute DVT/PE Treatment Order set Date:_________________ Diagnosis □ DVT □ PE Details: _____________________________________________________________ Details: _____________________________________________________________ Baseline Assessment Order (if not already done) □ CBC □ □ Creatinine Document PTT □ INR □ ALT/ALP Weight = ___________kg Calculate CrCl = __________mL/min (CrCl = [1.2 (140-age)(weight in kg)] (x 0.85 for females) SCr(umol/L) Treatment Options (Assess bleeding risk and select appropriate regimen) FOR ALL TREATMENT OPTIONS: □ Provide written prescription (see last page) □ Ensure follow-up in 1-3 weeks and 3 months □ Ensure patient follow-up the following day for monitoring/compliance Option 1: Rivaroxaban (Xarelto®) Yes No Is rivaroxaban an appropriate option? Patient preference Unable/unwilling to undergo S/C injections and/or INR testing + Adequate renal and liver function + Good compliance If YES, does the patient have any contraindications to rivaroxaban? Yes No CrCl < 30 mL/min, active bleeding, pregnant or breast feeding, clinically significant liver disease (ALT/ALP 3x ULN), concomitant use of both strong Pgp and CYP3A4 inhibitors (azole antifungals, HIV protease inhibitors) or CYP3A4 inducers (rifampin, phenytoin), active cancer (role uncertain at this time) In the absence of contraindications, □ Ensure patient has stopped antiplatelet agents (ASA, clopidogrel, prasugrel, ticagrelor) unless strongly indicated Then, ORDER □ rivaroxaban 15 mg po BID with food x 3 weeks, then 20 mg po daily with food [LU code 444] □ Educate patient on importance of compliance and provide handouts on VTE and rivaroxaban Option 2: LMWH bridge to warfarin Yes No Is bridging LMWH to warfarin an appropriate option? Significant drug-drug interaction with rivaroxaban (see above) Massive obesity Expected low compliance Unable to pay for rivaroxaban NOTES: If patient has severe renal dysfunction (CrCl <30 mL/min), dose reduce LMWH or use IV unfractionated heparin to bridge to warfarin 5 If YES, select applicable LMWH regimen: (NOTE: There is no max dose! Do NOT cap dose for weight!) Refer to Option 3: LMWH alone for available pre-filled syringe options enoxaparin 1.5 mg/kg SC OD or 1 mg/kg SC BID for at least 5 days and until therapeutic INR (2.0-3.0) ≥ 24h. □ enoxaparin ____________mg SC OD x at least 5 days and until INR 2.0-3.0 for at least 24h □ enoxaparin ____________mg SC BID x at least 5 days and until INR 2.0-3.0 for at least 24h dalteparin 200 units/kg SC OD or 100 units/kg SC BID for at least 5 days and until therapeutic INR (2.0-3.0) ≥ 24h. □ dalteparin _________units SC OD x at least 5 days and until INR 2.0-3.0 for at least 24h □ dalteparin _________units SC BID x at least 5 days and until INR 2.0-3.0 for at least 24h tinzaparin 175 units/kg OD for at least 5 days and until therapeutic INR (2.0-3.0) ≥ 24h. □ tinzaparin _________units SC OD x at least 5 days and until INR 2.0-3.0 for at least 24h AND Initiate Warfarin on the same day: Factors that affect warfarin dose: Day 1 1½ x the estimated maintenance dose Day 2 1½ x the estimated maintenance dose Day 3 INR in the morning and re-assess Select starting dose: □ 2.5 mg □ 5 mg □ 7.5 mg □ 10 mg □ Referral to anticoagulant clinic □ Educate the patient and provide handouts on VTE, - age (lower dose with increasing age) patient weight race (patients of Asian descent generally require 50% less warfarin while those of, African descent require higher doses) interacting medications (e.g. amiodarone, azole antifungals, TMP-SMX, phenytoin, rifampin, etc) nutritional status & supplements (vitamin K) acute illness, fever/infection uncorrected thyroid dysfunction - the specific LMWH and warfarin. Option 3: LMWH alone Is LMWH alone the most appropriate option? Uncontrolled malignancy, pregnant, patient preference, high bleeding risk AND CrCl ≥ 30 mL/min If YES, Yes No □ Educate the patient in subcutaneous injection technique (generally have the patient do the first injection under supervision) □ Provide patient handouts on VTE and the specific LMWH AND Select most appropriate dosing regimen: (NOTE: There is no max dose! Do NOT cap dose for weight!) □ Provide patient with written prescription [LU code 188] enoxaparin (Lovenox®) dalteparin (Fragmin ® ) □ enoxaparin 1.5 mg/kg SC OD □ dalteparin 200 units/kg SC OD OR OR □ enoxaparin 1 mg/kg SC BID □ dalteparin 100 units/kg SC BID If > 100kg, use BID dosing If >90kg, use BID dosing Round to nearest available prefilled syringe (please circle) Round to nearest available pre-filled syringe (please circle) 40 mg 5,000 IU 60 mg 80 mg 100 mg 120 mg 150 mg 7,500 IU 10,000 IU 12,500 IU 15,000 IU 18,000 IU tinzaparin (Innohep ®) □ tinzaparin 175 units/kg SC OD Round to the nearest available pre-filled syringe (please circle) 3,500 IU 4,500 IU 10,000 IU 14,000 IU 18,000 IU 6 Discharge Prescription Date:________________________ Patient Information Dr. __________________________ Address: Phone: Fax: Rx LU Code (circle one): 444 rivaroxaban 186 dalteparin, enoxaparin, tinzaparin (maximum 3 weeks) 188 dalteparin, enoxaparin, tinzaparin (warfarin contraindicated Physician Name (Please Print) Pager/Phone number Signature 7 ANTICOAGULANT DOSING RECORD Indication for anticoagulation: _______________________________________________ Target INR range: □ 2.0 – 3.0 Date INR Warfarin dose (mg) □ 2.5 – 3.5 Comments 8 Discharge Checklist Has the patient received the following? A. warfarin □ Warfarin discharge prescription - Use single tablet strength; - “Sig: Take as directed” - Generally prescribe at least a one-month supply □ Anticoagulant Record (faxed to place of referral and/or given to patient) □ Warfarin counseling □ Warfarin Dosing Calendar (include patient name and tablet strength on 1st page PLUS daily number of tablets for the relevant dates until next INR) □ Warfarin (Coumadin®) Information for Patients handout □ A referral for outpatient anticoagulation supervision/management: □ Name of Anticoagulant Clinic: _________________________ □ Family Doctor/Other: ________________________________ □ Who to contact if any further questions _______________________ B. Xarelto (rivaroxaban) □ Discharge prescription (generally prescribe at least the first 3-week supply) □ Rivaroxaban counseling □ Rivaroxaban Information for the VTE Patient handout □ Arrangements for outpatient follow-up (who/date): ___________________________________________________ □ Who to contact if any further questions ________________________ C. Lovenox (enoxaparin), Fragmin (dalteparin), Innohep (tinzaparin) □ Discharge prescription (generally prescribe at least a one-week supply if bridging to warfarin or a one-month supply if continuing LMWH longer) □ □ □ □ LMWH counseling LMWH Information for Patients handout Subcutaneous Injection Technique handout and counseling Arrangements for outpatient follow-up (who/date): _____________________________________________________ □ Who to contact if any further questions _________________________ 9 Care Pathway for Long-Term Management of VTE: Follow-up and Monitoring Patient with Confirmed DVT/PE Treatment Initiated: rivaroxaban, warfarin, or LMWH Offer Determine frequency of follow-up and arrange appointments 1. Contact patient the day after start of treatment AND at: 1-3 weeks AND 3 months 2. Then, every 3 months to 12 months In case of problems, patient contacts MD Compliance tool: Blister pack/Dosette Phone call reminders Text messages Mobile app/reminder e-mail At each visit Clinical Monitoring: Efficacy (symptoms/signs of DVT/PE) Bleeding? Other adverse effects New medications? OTC, herbal supplements? Interactions? Lab Monitoring CBC, Renal, Liver function yearly If CrCl 30-50 mL/min Cr every 6 months If CrCl 15-30mL/min Cr every 3 months Compliance: Ask patient to bring remaining pills Ask patient how many doses missed Educate on how to deal with missed dose Re-emphasize importance Offer aids (blister packs, etc) Education: Answer any questions the patient has Educate re: importance of compliance 10 Patient Information 11 Venous Thromboembolism (VTE): Information for the Patient Venous thrombembolism (VTE) refers to an abnormal blood clot that develops in a vein or the lung. An abnormal blood clot in the leg is called deep vein thrombosis (DVT) and an abnormal blood clot in the lungs is called pulmonary embolism (PE). DVT and PE are serious conditions but they are treatable. DVT and PE DVT is a condition in which an abnormal blood clot, also called a “thrombus”, forms in one or more of the veins deep in the body, generally in a leg. Sometimes part of a DVT from the leg can break off and travel to the lung, where it is known as PE. Symptoms and Signs of DVT and PE Common symptoms of a DVT may include: Swelling of the leg Pain and tenderness of the leg Warmth over the affected area Changes in skin colour (e.g. turning red or purple) Symptoms of a PE may include: Chest pain that is sharp and is worse when taking a deep breath Sudden difficulty breathing Feeling light-headed, dizzy, or faint Sweating Rapid heart beat Coughing up blood What are some risk factors for DVT and PE? Certain people are more likely to develop DVT and/or PE. Risk factors include: Surgery Pregnancy Trauma Birth control pills or hormone Immobility or paralysis replacement therapy Cancer and cancer treatments Obesity Increasing age Inflammatory bowel disease Previous DVT or PE Chronic kidney disease Family history of DVT or PE Prolonged travel Medical illness such as heart failure, Abnormalities of blood clotting infection (inherited or not inherited) How are DVT and PE treated? DVT and PE are treated with medicines called anticoagulants. Anticoagulants do not dissolve existing blood clots. They keep the clot from getting bigger and prevent future clots from developing. Some of these anticoagulants come as injections and others come as pills. 12 There are three main methods to treat a DVT or PE: 1. Use of an anticoagulant called a low molecular weight heparin (LMWH), given for at least 5 days. This is an injection that is given just under the skin. A tablet anticoagulant called warfarin is usually started at the same time as the LMWH injection and is continued in the long term. The LMWH injections are usually stopped within the first week. 2. LMWH injections alone for the entire duration of treatment. 3. The newest option is to use an oral anticoagulant called rivaroxaban (Xarelto®), which is taken daily for the entire duration of treatment. Your doctor will discuss the best choice of treatment for you and how long you will need to be treated. Most patients are treated for at least three months. Some patients need to be treated for longer (and some are treated indefinitely). The main side effect of anticoagulant treatment is bleeding which is not common and is usually minor. For example, you might get: A nose bleed that lasts for less than 5 minutes Easy bruising Bleeding gums while brushing teeth. Some bleeding can be more serious; however this is rare. What happens to the DVT or PE? Some patients will experience improvement of symptoms within days or weeks while others may take longer. Some patients with DVT can develop post-thrombotic syndrome, which is leg swelling and/or discomfort caused by damage to the veins. Compression stockings will help reduce the severity of this complication. If you had a DVT, signs that we expect there will be: Reduced leg swelling Reduced pain Improved ability to walk If you had a PE, signs that we expect there will be: Improvement in shortness of breath and chest pain How long it will take to see these changes is different for each person. General tips to consider while being treated for DVT or PE: Take your medication every day, at approximately the same time. Forgetting to take your anticoagulant puts you at risk of worsening of the clot or developing a new clot. Talk to your doctor if you are taking antiplatelet medications (acetylsalicylic acid [Aspirin®], clopidogrel [Plavix®], ticagrelor [Brilinta®], prasugrel [Effient®]). These medications increase your risk for bleeding and should only be taken if strongly recommended by a doctor. Move around! The sooner you get moving, the faster you will feel better. Adopt a healthy lifestyle. Lose weight if you are overweight. Quit smoking and control your blood pressure. Maintain or start a healthy diet. Wear compression stockings if your doctor recommends them. See your doctor regularly, at least at 3 months and then every 6 to 12 months. Talk to your doctor if you notice unexpected bleeding including extremely dark stools, cough up blood, bleeding in the urine or from the rectum, large bruises on body without being injured, and nosebleeds that won’t stop. Exercise daily. There is no need to restrict your activity. 13 Low molecular weight Heparin (LMWH): Information for Patients You are being treated with a low molecular weight heparin called __________________ You should take ____________ (drug name) ____________ (dose) once daily OR twice daily. (circle one) What is a low molecular weight heparin (LMWH)? A low molecular weight heparin is an anticoagulant, a drug that prevents new blood clots from developing. Anticoagulants are sometimes called "blood thinners", but this name is misleading. These drugs do not "thin the blood" but they do make the blood less likely to clot when it shouldn’t. Why do I need to take it? Deep vein thrombosis (DVT) and/or pulmonary embolism (PE) – DVT occurs when an abnormal blood clot develops in a vein, usually of the leg or arm. A blood clot in a vein can break free and travel to the lungs – this is then called pulmonary embolism. How do LMWHs work? LMWHs lower the activity of clotting factors in the blood to a level that makes it less likely that harmful clots will form in the blood. LWMHs do NOT stop the blood from clotting completely and do NOT break down clots that are already there. How should I take this medicine? This medication is given as an injection under the skin once or twice daily. Please see the attached Subcutaneous Injection Technique handout for instructions What are some possible side effects? The main side effect of LMWHs is increased risk of bruising, especially around an injection site. Bleeding can also occur but this is uncommon Things to remember when taking a LMWH: It is important that you have the injection around the same time every day Do not stop it on your own Some bruising is common after some injections If you experience bleeding that worries you, contact your physician 14 Subcutaneous Injection Technique for Dalteparin (Fragmin®), enoxaparin (Lovenox®), tinzaparin (Innohep®), and fondaparinux(Arixtra®) Administration Wash your hands Select appropriate place where you will inject the medication (Fig.1) Wipe the site with an alcohol swab and allow it to dry Remove the needle cap Gently pinch up a 3 cm fold of skin Hold syringe perpendicular to skinfold (Fig.2) Insert needle slowly and completely into skinfold at 90˚angle (Fig.3) – keep pinching skinfold Do not pull back on plunger Inject contents of syringe Remove syringe and dispose in sharps container Let go of skinfold If injection site oozes, apply gentle pressure with gauze Do not rub site after injection Reminders Use the stomach area as a first choice of where to inject Move the place where you inject around Other places include front and sides of mid and upper thigh (Fig.1) Avoid injection into arms, unless absolutely necessary Stay about 2 cm from belly button, surgical cuts or scars, and places you have injected before Avoid bruised areas 15 Rivaroxaban (Xarelto®) Information for Patients with DVT and/or PE You are being treated with an anticoagulant called rivaroxaban. Your dose of rivaroxaban is _________mg taken Twice daily until __________________________ (date: yyyy/mm/day) AND / OR Once daily from ________________________ (yyyy/mm/day) What is rivaroxaban? Rivaroxaban is an anticoagulant, a drug that prevents new blood clots from developing. Anticoagulants are sometimes called "blood thinners", but this name is misleading. These drugs do not "thin the blood" but they do make the blood less likely to clot when it shouldn’t. Why do I need to take it? Deep vein thrombosis (DVT) and/or pulmonary embolism (PE) DVT occurs when an abnormal blood clot develops in a vein, usually of the leg or arm. A blood clot in a vein can break free and travel to the lungs – this is then called pulmonary embolism. How does rivaroxaban work? Rivaroxaban blocks one of the clotting factors in the blood to a controlled level. This makes it less likely that harmful clots will form in the blood. Rivaroxaban does NOT stop the blood from clotting completely and does NOT dissolve clots that are already there. How should I take rivaroxaban? Take rivaroxaban once daily OR twice daily (circle one) Take rivaroxaban with food at approximately the same time everyday. Try not to miss any doses. If you miss a dose o and you take rivaroxaban 2 times a day: Take the missed dose as soon as you remember on the same day. You may take 2 doses at the same time to make up for the missed dose. o and you take rivaroxaban once a day: Take rivaroxabn as soon as you remember on the same day. Take your next dose at your regularly scheduled time the next day. Do not take 2 doses on the same day. What are some possible side effects? The main side effect of rivaroxaban is a small increase in the risk of bleeding or bruising 16 Warfarin (Coumadin®) Information for Patients with DVT and/or PE You are being treated with warfarin for the following condition: deep vein thrombosis pulmonary embolism What is warfarin? Warfarin is an anticoagulant, a drug that prevents new blood clots from developing. Anticoagulants are sometimes called "blood thinners", but this name is misleading. These drugs do not "thin the blood" but they do make the blood less likely to clot when it shouldn’t. Why do I need to take it? Deep vein thrombosis (DVT) and/or pulmonary embolism (PE) – DVT occurs when an abnormal blood clot develops in a vein, usually of the leg or arm. A blood clot in a vein can break free and travel to the lungs – this is then called pulmonary embolism. How does warfarin work? Warfarin lowers the amount of clotting factors in the blood to a controlled level. This makes the blood less likely to form harmful clots. Warfarin does NOT stop the blood from clotting completely and does NOT break up or dissolve clots that are already there. How should I take this medicine? Warfarin is taken once a day. It can be taken at any time of the day but it should be taken around the same time every day. It is important to record every dose of warfarin and every INR test result in one place like a warfarin calendar. This helps to avoid mistakes in the dose. As soon as you’ve taken your dose of warfarin “check off” the dose on your calendar. It is also a good idea to put your daily doses for a week into a 7-day plastic pillbox. Why do I need blood tests? Blood tests are needed to find the right amount of warfarin that you need to keep abnormal blood clots from forming and to minimize the risk of bleeding. Anticoagulation is a delicate process. If the effect of the warfarin on your blood is too high, you increase your risk of serious bleeding. If the effect of the warfarin on your blood is too low, you are at risk for further abnormal clotting. These blood tests must continue to be done as long as warfarin is used because many things can affect your response to warfarin. 17 What blood tests do I need to have? You will have a blood test that is called INR (International Normalized Ratio). The INR helps to measure how well warfarin is working. People who are not taking warfarin have an INR value of about 1.0. The higher the INR value, the longer it takes the blood to clot. Most patients on warfarin need an INR between 2.0 and 3.0. An INR below 2.0 may lead to more abnormal clotting. An INR greater than 4.0 increases the risk of serious bleeding. A person cannot guess whether their INR is low, high or just right without doing the INR test. What are the side effects associated with taking warfarin? The main complication of taking warfarin is a somewhat increased risk of bleeding. What should I do if I forget to take a warfarin pill? If you forget to take a dose at your regular time, take it as soon as you remember and take the next dose at the usual time. If you forget to take warfarin for 2 or 3 days in a row, DO NOT take all of the missed doses, but call your doctor or clinic for instructions. How do food and alcohol affect warfarin therapy? Eating foods that have vitamin K can affect your body’s response to warfarin. Foods that have vitamin K include spinach, broccoli, brussel sprouts, lettuce, collard and turnip greens, cabbage, and kale. These foods are very good for you and you should NOT avoid them. Eating about the same amount of these foods over a week and doing INR tests regularly helps you to get the right amount of warfarin. Patients on warfarin can safely have one or two alcoholic drinks (beer, glass of wine, liquor) a day. More alcohol can make the INR go too high and can be dangerous. DO NOT binge drink. Can I take other drugs while I’m on warfarin? What if I have a headache or a ‘cold’? Many drugs and herbal remedies interact with warfarin and increase or decrease its effect. It is best to check with your doctor or pharmacist BEFORE starting or stopping any medication. You can safely take 1 or 2 tablets of acetaminophen (Tylenol®) or ibuprofen (Advil®, Motrin®). If you need more than that, you should talk to your doctor or pharmacist first. You should not take aspirin (or medications with aspirin in them) unless your doctor tells you to. 18 Management of Bleeding in a Patient receiving Rivaroxaban Pharmacologic Properties: Peak level = 2-4 hours 35% renal clearance Half-life = 8-13 hours (longer in elderly and those with renal dysfunction) Assessment of Bleeding in a Patient Receiving Rivaroxaban No proven antidote (“time is the most important antidote”) There is limited clinical data related to reversal of rivaroxaban the recommendations below may change as new evidence becomes available Patient with bleeding on rivaroxaban When was last dose? CBC, creatinine PT* (not INR) If PT > 15 sec Mild bleeding Local hemostatic measures Hold 1 dose of rivaroxaban Moderate-severe bleeding1 *Provides qualitative and partial quantitative assessment of rivaroxaban activity. Life-threatening bleeding1 Manage bleeding (compression, surgery) Fluid diuresis Transfuse RBCs or platelets if needed Oral charcoal if overdose <2 hrs before Tranexamic acid (1G IV followed by 1G infusion over 8 hours) Consider PCC2 1. DO NOT TRANSFUSE plasma or cryoprecipitate to reverse rivaroxaban 2. PCC (Octaplex / Beriplex) References: Heidbuchel H, et al – Europace 2013;15:625-651 19 Management of Bleeding in a Patient receiving Warfarin Patient with bleeding on warfarin INR ≥ 2.0 Mild bleeding e.g. epistaxis bruising hemorrhoids Severe or life threatening bleed with INR ≥ 2.0 Manage bleeding (compression, surgery) If INR supratherapeutic, hold 1-2 doses of warfarin and restart at lower dose Educate on preventative measures (e.g. avoid trauma, straining/ constipation) PCC (Octaplex / Beriplex) follow hospital guidelines AND Vitamin K 10 mg IV 20 Periprocedure Management Periprocedure Management of Rivaroxaban Planned procedure in patient taking therapeutic dose of rivaroxaban Pre-op * Low Bleeding Risk procedure Hold rivaroxaban 1 day before High Bleeding Risk procedure Hold rivaroxaban 2 days before * If CrCl ≤ 30 mL/min (rivaroxaban contraindicated), should stop rivaroxaban for longer (>2 days before). Lab Monitoring before an invasive procedure (THIS IS NOT ROUTINE) If the procedure requires complete reversal of anticoagulation, especially if renal function impaired or is unknown, consider obtaining a PT test (gives a semi-quantitative result) o If PT is normal likely little or no significant anticoagulant effect o If PT is elevated LIKELY an anticoagulant effect present high bleeding risk procedure? elevated PT may warrant delay of the procedure. Restarting rivaroxaban following an invasive procedure Patient achieves therapeutic anticoagulation approximately 2 hours after a dose. If the postoperative bleeding risk associated with full, therapeutic anticoagulation is not desirable, the following options should be considered: a) Delay resuming rivaroxaban until the bleeding risk decreases to usual b) Bridge with a prophylactic dose (rivaroxaban 10 mg po OD) or with a LMWH until the bleeding risk decreases to usual 21 Periprocedure Management of LMWH Planned procedure in patient taking therapeutic dose of LMWH Pre-op: Hold LMWH approx 24h before surgery Low risk procedure High risk procedure Resume LMWH approximately 24h post-op Consider prophylactic dose of LMWH initially Resume therapeutic dose of LMWH 48-72h post-op 22 Periprocedure Management of Warfarin Patient on warfarin who requires surgery/ invasive procedure Interruption of anticoagulant required? Yes No Criteria to NOT interrupt anticoagulant*: 1. cataract surgery 2. most dental procedures 3. thoracentesis 4. paracentesis 5. arthrocentesis 6. skin biopsies Low Risk*: Most A-fib Most VTE >3months PAD Stroke Mechanical AVR with no additional risk factors Moderate Risk*: All mechanical MVR Mechanical AVR with previous TIA/stroke or A-fib or severe LV dysfunction VTE < 3months Obtain an INR approximately one week before procedure to ensure not supratherapeutic Obtain INR approx. 1 week before procedure Hold warfarin 5 days before surgery (6 days if INR >3.0) Hold warfarin 5 days before surgery (6 days if INR >3.0) No anticoagulant bridging Consider consulting an Anticoagulant Clinic at least 10 days pre-op Bridge with a LMWH No further intervention required Provide patient with advice about anticoagulant management Yes Uncertain Risk: Consider consulting an Anticoagulant Clinic or expert OR cancelled/ delayed? No Patient undergoes procedure * Specific patient or procedure circumstances may change the patient risk profiles and recommendations 23