Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
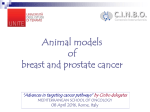
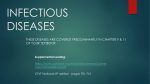
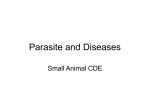
progress in orthodontics 1 3 ( 2 0 1 2 ) 42–48 Available online at www.sciencedirect.com journal homepage: www.elsevier.com/locate/pio Original article A Controlled Study on Diagnostic and Prognostic Measurements of Palatally Displaced Canines on Lateral Cephalograms Heidi M. Novak a , Tiziano Baccetti b,∗ , Lauren M. Sigler a , James A. McNamara Jr. c a Research Assistant, Department of Orthodontics and Pediatric Dentistry, School of Dentistry, The University of Michigan, Ann Arbor, USA b Assistant Professor, Department of Orthodontics, The University of Florence, Florence, Italy; Thomas M. Graber, Visiting Scholar, Department of Orthodontics and Pediatric Dentistry, School of Dentistry, The University of Michigan, Ann Arbor, USA c Thomas M. and Doris Graber, Endowed Professor of Dentistry, Department of Orthodontics and Pediatric Dentistry, School of Dentistry; and Research Professor, Center for Human Growth and Development, The University of Michigan, Ann Arbor, USA a r t i c l e i n f o a b s t r a c t Article history: Objectives: The aim of this prospective controlled study was to determine the role that the Received 12 July 2011 lateral cephalogram can play in the detection of palatally displaced canines (PDCs). Accepted 13 July 2011 Materials and methods: The study was comprised of 85 subjects in the late mixed dentition. Thirty-five subjects had PDCs (either unilateral or bilateral) identified on the panoramic Keywords: radiograph (PDC group), and 50 subjects presented with a normal pathway of upper per- Diagnosis manent canine eruption as assessed on panoramic radiographs (No-PDC group). Linear and Displaced canines angular measurements on the lateral cephalograms concurrent with panoramic radiographs Impacted canines were compared between the PDC and No-PDC group statistically. Lateral cephalogram Results: All angular measurements that incorporated the main axis of the canine (to Frankfort horizontal, to the palatal plane, or to the axis of the central incisor) were significantly smaller in the PDC group (p<0.001). In terms of linear measurements, both the distance from the tip of the canine to the vertical axis of the central incisor parallel to Frankfort horizontal and the distance from the tip of the canine to the anterior alveolar ridge parallel to Frankfort horizontal showed significantly larger values in the PDC subjects than in normal controls. On the contrary, the vertical distance from the tip of the canine to the functional occlusal plane did not reveal any significant difference between the PDC and the No-PDC group. Conclusions: Early diagnosis of PDC is essential in order to avoid the occurrence of final canine impaction. If 3-D images of a displaced canine cannot be acquired, a lateral cephalogram can be a useful tool for the early detection of PDC in the late mixed dentition. The angle between the vertical axis of the canine and the palatal plane demonstrate diagnostic value when assessing PDCs. Values for this angle smaller than 102 degrees can indicate the presence of PDC. © 2011 Società Italiana di Ortodonzia SIDO. Published by Elsevier Srl. All rights reserved. ∗ Corresponding author. Department of Orthodontics, University of Florence, Via del Ponte di Mezzo 46-48 – 50127 Florence, Italy. E-mail address: tbaccetti@unifi.it (T. Baccetti). 1723-7785/$ – see front matter © 2011 Società Italiana di Ortodonzia SIDO. Published by Elsevier Srl. All rights reserved. doi:10.1016/j.pio.2011.07.001 progress in orthodontics 1 3 ( 2 0 1 2 ) 42–48 1. Introduction Natural history studies have reported 0.2 to 2.3 percent of orthodontic populations to have at least one impacted maxillary canine tooth.1 In European populations, approximately 85% of maxillary canine impactions are oriented palatally.1,2 Palatal maxillary canine impaction is thought to have a genetic etiology.3 The pathogenesis of palatal canine impaction is characterized by an early developmental stage that can be reversed with treatment. At this stage, the canine is considered to be a “palatally displaced canine (PDC),” as it presents with an intraosseous palatal position prior to expected time of eruption.1 If left untreated, PDCs generally progress to impaction after the pubertal growth spurt and will require surgical intervention.4,5 Recent studies reported prevalence rates for impaction of PDCs ranging from 75-85%.6,7 Failure to recognize and treat maxillary canine displacement may result in root resorption of adjacent teeth8–10 and/or the formation of cysts.11–13 Furthermore, patients with PDCs that progress to impaction will incur higher treatment costs, more complex treatment plans, and delayed treatment timetables.14,15 Early interceptive treatment measures of PDCs aimed to prevent the final occurrence of maxillary canine impaction have been proven to be effective. These treatments include deciduous canine extraction that may be coupled with protocols that include molar distalization and/or treatment for Class II or Class III tendencies and/or treatment for mildto-moderate tooth-size/arch-size discrepancies.7,16–19 Early detection and adequate evaluation of the PDC condition is a necessary prerequisite for each of these treatment approaches. Currently, PDCs are detected most commonly by assessing maxillary canine position using panoramic radiographs.11 Using these radiographs, a PDC is characterized by an increased angle between the main axis of the canine and the midline and/or the cusp overlapping the ipsilateral central or lateral incisors.9 Diagnosis of PDC on panoramic radiographs is recommended in the late mixed dentition after the age of 10 years, while earlier evaluation does not appear to be reliable due to developmental processes in the eruption of the permanent canine.7,11,20 During the same age period, panoramic radiograph evaluation for PDCs can be supplemented by digital palpation of the maxillary canine region.21,22 The lateral cephalogram also is a type of radiograph that can supplement detection of palatally displaced canines. The lateral cephalogram, that are part of the standard radiographic records for orthodontic treatment planning, can provide additional information about the location and severity of displacement of upper permanent canines with an anomalous eruption pathway. However, there have been hardly any studies as to the role the lateral cephalograms can play potentially in describing the intraosseous position of PDCs. One study by Orton et al.23 used lateral cephalograms to investigate root resorption caused by unerupted palatal canines. The study included the angle of the coronal vertical axis of the canine to the Frankfort horizontal, the distance between the apex of the canine and the occlusal plane, and canine sagittal position to evaluate the ability of an ectopic canine in causing root resorption. 43 The goal of the present prospective controlled study was to evaluate the use of measurements on lateral cephalograms for overall PDC detection in the late mixed dentition. 2. Materials and methods The study included subjects from a two-center prospective clinical trial at the Department of Orthodontics and Pediatric Dentistry of the University Michigan and the Department of Orthodontics at the University of Florence, Italy, between 1985 and 2009. Enrollment criteria for subjects in the trial were as follows: • Caucasian ancestry; • age range from 9.5 to 13.0 years; • late mixed dentition stage; • stage of skeletal growth ranging from CS1 to CS4 as evaluated on lateral cephalograms according to the cervical vertebral maturation method;24 • absence of previous orthodontic treatment; and, • absence of supernumerary teeth, odontomas, cysts, craniofacial malformations, or sequelae of traumatic injuries. The study sample included 85 subjects with the listed features above. Thirty-five of them had PDCs (either unilateral or bilateral) identified on the panoramic radiograph (PDC group), while 50 subjects presented with a normal pattern of upper permanent canine eruption pathway as assessed on panoramic radiographs (No-PDC group). Informed consent was signed by the parents of all subjects enrolled in the trial in both of the research sites. 2.1. Diagnostic Measurements at T1 The following measurements proposed by Ericson and Kurol11 were performed on panoramic radiographs of all subjects (Fig. 1): • alpha angle: mesial inclination of the crown of the permanent canine to the midline (Fig. 1A); • d distance: distance of the cusp tip of the permanent canine to the occlusal line (Fig. 1B); • sector: indicating the mesial position of the crown of the displaced canine with respect to the central and lateral incisors (5 sectors, with sector 1 indicating the position of the crown of the displaced canine posterior to the distal aspect of the lateral incisor and sector 5 in correspondence with the mesial half of the upper central incisor) (Fig. 1C). As indicated by Ericson and Kurol,11 these measurements are valid diagnostic variables for PDC within the age range studied in this trial. Palatal displacement of the canine(s) was confirmed by means of Clark’s tube shift rule using multiple intraoral radiographs of the canine region.25 Lateral cephalograms of all subjects concurrent with the panoramic radiographs were analyzed. The following measurements were performed on the lateral cephalograms (Fig. 2): • Angle of the vertical axis of the canine to the Frankfort plane (VAC-FH, degrees); • Angle of the vertical axis of the canine to the palatal plane (VAC-PP, degrees); 44 progress in orthodontics 1 3 ( 2 0 1 2 ) 42–48 Fig. 1 – Measurements of canine position on a panoramic radiograph. A) alpha angle; B) d distance; C) sector. • Angle of the vertical axis of the canine and the vertical axis of the central incisor (VAC-VAI, degrees); • Distance from the tip of the canine to the vertical axis of the central incisor parallel to Frankfort horizontal (dC-VAI, mm); • Distance from tip of the canine to the anterior alveolar ridge parallel to Frankfort horizontal (dC-AAR, mm); • Distance from the tip of the canine to the functional occlusal plane (dC-FOP, mm) (Fig. 3). The magnification factor for the panoramic films in both groups was 18%, while the magnification factor of the lateral cephalograms was 8%. 2.2. Fig. 2 – Measurements of canine position on a lateral cephalogram: A. Angle of the vertical axis of the canine to the Frankfort plane (VAC-FH, degrees); B. Angle of the vertical axis of the canine to the palatal plane (VAC-PP, degrees); C. Angle of the vertical axis of the canine and the vertical axis of the central incisor (VAC-VAI, degrees); D. Distance from the tip of the canine to the vertical axis of the central incisor parallel to Frankfort horizontal (dC-VAI, mm); E. Distance from tip of the canine to the anterior alveolar ridge parallel to Frankfort horizontal (dC-AAR, mm); F. Distance from the tip of the canine to the functional occlusal plane (dC-FOP, mm). Power of the Study and Method Error The estimate of the power of the study was performed before the beginning of the clinical part of the trial. Taking into consideration the standard deviations of the diagnostic measures on the panoramic radiographs from a previous study7 and the use of non-parametric or categorical statistics, the calculated power of the study exceeded 0.90 at an alpha=0.05 with the sample sizes of 50 subjects and 35 subjects in the 2 examined groups, respectively. Accuracy of measurements on panoramic radiographs was calculated using the Dahlberg’s formula26 on measures repeated on 15 subjects selected randomly from the two groups. The method error was smaller than 1.5◦ for angular measures, and smaller than 1 mm for the linear distances. The appraisal of the sector of canine displacement showed a reproducibility of 100%. 2.3. Statistical analysis The descriptive statistics for demographic data (age and gender) as well measurements on panoramic films and lateral cephalograms comparisons were carried out with progress in orthodontics 1 3 ( 2 0 1 2 ) 42–48 45 10 years 3 months ± 10 months. The No-PDC group was comprised of 26 female subjects and 24 male subjects, and the PDC group was comprised of 24 female subjects and 11 male subjects. The descriptive statistics for the measurements on panoramic films in the 2 groups is reported in Table 2. There was a statistically significant difference in both alpha angle and sector between the No-PDC group and PDC group, with the PDC group showing greater values for the angle and more severe sectors of displacement. No statistically significant difference between the 2 groups was found for the d distance. The descriptive statistics for the measurements on lateral cephalograms in the 2 groups. The VAC-FH and the VAC-PP angles were significantly smaller in the PDC group (about -6 degrees and -12.8 degrees, respectively). The VAC-VAI angle was significantly smaller in PDC subjects as well (-4.8 degrees difference). The dC-VAI and the dC-AAR distances showed significantly greater values in the PDC group (5.4 mm and 3.9 mm) than in the No-PDC group. No significant difference was assessed for the dC-FOP distance between the 2 groups. 4. Fig. 3 – Graphical illustrations of the average intraosseous position of the upper permanent canine in the PDC group (A) and in the No-PDC group (B). Mann-Whitney U tests (p<0.05) for metric measures and with chi-squared tests (p<0.05) for categorical measures. Statistical analysis was performed with statistical software (Statistical Package for the Social Sciences, SPSS, Version 16.0.1 Chicago, IL). 3. Results The mean age (Table 1) for the No-PDC group was 10 years 2 months ± 6 months. The mean age for the PDC group was Discussion Early diagnosis of PDC is required in order to plan adequate interceptive approaches that may prevent the occurrence of final canine impaction. PDCs are detected most commonly by assessing maxillary canine position using panoramic radiographs,11 and this assessment is usually supplemented by digital palpation of the maxillary canine region.21,22 Although lateral cephalograms are needed regularly for orthodontic treatment planning, the literature is lacking studies on the role of this diagnostic tool in describing the intraosseous position of PDCs, with the exception of Orton et al.23 who used lateral cephalograms to investigate root resorption caused by palatally impacted canines. The study included the angle of the coronal vertical axis of the canine to the Frankfort horizontal, the distance between the apex of the canine and the occlusal plane, and canine sagittal position to evaluate the ability of an ectopic canine in causing root resorption. The aim of the current study was to evaluate the information derived from lateral cephalograms for overall PDC detection in the late mixed dentition. Both the alpha angle and sector measurements on a panoramic radiograph in the late mixed dentition confirmed their diagnostic value in detecting PDCs.20 There was an average difference in alpha angle between PDC and No-PDC subjects of about 20 degrees, with the angle significantly greater in the PDC group. In terms of sector of intraosseous position, the No-PDC group did not present any maxillary canine in sectors 3 or 4, while the percentage of PDC cases showing displacement of the canine in these sectors was 34%. The measures on the lateral cephalograms corresponding to the panoramic radiographs provided significant information regarding the palatal displacement of the canines in the PDC subjects. All angular measures describing the inclination of the main axis of the canine to the Frankfort plane, or to the palatal plane, or to the axis of the central incisor were significantly smaller in the PDC group. The values derived from the No-PDC group can be used as reference values when assessing the relative position of the canine on a lateral cephalogram 46 progress in orthodontics 1 3 ( 2 0 1 2 ) 42–48 Table 1 – Descriptive statistics for the measurements on panoramic films and between-group comparisons PDC Group n =35 Panoramic Radiographic Measures Mean Alpha angle d distance SD 27.5 17.0 9.7 3.6 Number of Cases Sector 1 Sector 2 Sector 3 Sector 4 No-PDC Group n = 50 Percentage 8 15 8 4 PDC vs No-PDC Mean SD MW-Test 7.6 14.1 3.9 3.1 *** NS Number of Cases Percentage 46 4 0 0 92% 8% 0% 0% 23% 43% 23% 11% Chi-squared test *** *** p<0.001; NS=not significant. during the mixed dentition. It should be pointed out, however, that the measures of canine inclination that include the main axis of the central incisor may be strongly influenced by the relative inclination of this tooth to the craniofacial structures. Similar considerations can be made with regard to the inclination of the maxillary canine to FH, as this variable can be influenced by the relationships between FH and the maxillary bone. More reliable information regarding the position of the upper permanent canine within the maxillary bony structures can be derived from the analysis of the inclination of the canine to the palatal plane. Subjects showing PDC exhibit, on average, a VAC-PP angle which is about 13 degrees smaller than subjects with a normal eruption pattern of the canine. The decreased angulation of the canine relative to the palatal plane indicates the palatal displacement of the crown of the tooth. The “effect size” (the ratio between the mean betweengroup difference and the mean of the standard deviations of the two groups)27 for the comparison between PDC and No-PDC subjects as to the VAC-PP angle was highly significant (>2). This means that the between-group difference was significantly greater than the individual variability within the groups when assessing the value for the angular measure, thus demonstrating the diagnostic validity of this variable. The findings of the present study can be compared with those of the report by Orton et al.23 limited to the use of the angle between the vertical axis of the canine and the Frankfort horizontal. In the previous study, the authors identified as normal eruption pathway an inclination of the canine relative to FH of 100 to 115 degrees. These values are similar to the findings of the current investigation, as we found the canine to be normally located within the bony structures when the VAC-FH angle was between 99.7 to 116.3 degrees. As for the distances, both the dC-VAI and the dC-AAR measures showed significantly larger values in the PDC subjects than in normal controls. However, these results were expected on the basis of the between-group differences in the previously reported angular measurements. On the contrary, the vertical distance dC-FOP did not reveal any significant difference between PDC and No-PDC groups. This finding confirmed also the lack of diagnostic value of the d distance on panoramic radiographs. The recent development of low-dose or cone-beam computerized tomography is improving significantly the possibility to appraise the intraosseous position of maxillary canines in growing subjects. However, in the lack of 3-D imaging locating the canine within the maxillary bony structures, Table 2 – Descriptive statistics for the measurements on lateral cephalograms PDC Group n = 35 No-PDC Group n = 50 PDC vs No-PDC Lateral Cephalogram Measures Mean SD Mean SD Vertical axis of the canine and the Frankfort plane (VAC-FH ◦ ) Vertical axis of the canine to the palatal plane (VAC-PP◦ ) Vertical axis of the canine to the vertical axis of the central incisor (VAC-VAI◦ ) Cusp tip of the canine to the axis of the central incisor, parallel to Frankfort horizontal (dC-VAI, mm) Cusp tip of the canine to the anterior alveolar ridge, parallel to Frankfort horizontal (dC-AAR, mm) Cusp tip of the canine perpendicular to the occlusal plane (dC-FOP, mm) 102.1 5.9 108.0 6.3 -5.9 *** 96.4 5.7 109.2 6.5 -12.8 *** 3.2 2.6 8.0 6.7 -4.8 *** 9.6 4.2 4.2 2.1 5.4 *** 12.8 4.3 8.9 2.3 3.9 *** 10.4 2.4 10.0 3.1 0.4 NS ***p<0.001; NS=not significant. Mean Difference MW-Test progress in orthodontics 1 3 ( 2 0 1 2 ) 42–48 the use of a lateral cephalogram appears to be a valuable adjunct for the diagnosis of PDC in late mixed dentition patients. 5. Conclusions The lateral cephalogram is able to provide useful information regarding the intraosseous position of maxillary permanent canines in the late mixed dentition that can supplement indications derived classically from panoramic radiographs. Among a series of angular and linear measures on a lateral cephalogram, the angle between the vertical axis of the canine and the palatal plane demonstrate diagnostic value when assessing PDCs. Values for this angle smaller than 102 degrees can indicate the presence of PDC. Conflict of interest The authors have reported no conflicts of interest. Riassunto Obbiettivi: L’obbiettivo di questo studio prospettico controllato è stato quello di determinare il ruolo che la teleradiografia in proiezione latero-laterale può avere nell’identificazione del dislocamento palatino dei canini (PDC). Materiali e metodi: Lo studio ha analizzato 85 soggetti in fase di dentatura mista tardiva. Trentacinque soggetti presentavano PDC (mono- o bilaterale) identificato sulla ortopantomografia (gruppo PDC) e 50 soggetti presentavano un percorso eruttivo normale dei canini superiori permanenti valutato sulla ortopantomografia (gruppo No-PDC). Misurazioni lineari ed angolari sulle teleradiografie latero-laterali corrispondenti alle ortopantomografie sono state confrontate statisticamente tra i due gruppi. Risultati: Tutte le misurazioni angolari che comprendevano l’asse del canino (rispetto al piano di Francoforte, al piano palatino, e all’asse dell’incisivo centrale) erano significativamente minori nel gruppo PDC (p<0.001). Per quanto riguarda le misurazioni lineari le distanze parallele al piano di Francoforte dalla cuspide del canino all’asse dell’incisivo centrale e dalla cuspide del canino al margine alveolare anteriore erano significativamente maggiori nei soggetti con PDC. La distanza verticale dalla cuspide del canino al piano occlusale funzionale non mostrava differenze significative nei due gruppi. Conclusioni: La diagnosi precoce di PDC è fondamentale per evitare l’inclusione del canino permanente. Se non è possibile acquisire immagini tridimensionali di un canino in malposizione intraossea, una teleradiografia in proiezione latero-laterale può essere utile per identificare precocemente il dislocamento palatino del canino in fase di dentatura mista tardiva. L’angolo tra l’asse del canino e il piano palatino si è dimostrato di valore diagnostico nella valutazione del dislocamento palatino del canino permanente. In particolare, valori per quest’angolo inferiori a 102 gradi possono indicare la presenza di PDC. Résumé Objectifs: Cette étude contrôlée prospective vise à préciser le rôle que le céphalogramme latéral peut jouer dans la détection de canines incluses en palatin (PDCs). 47 Matériels et méthodes: L’étude a porté sur 85 patients en denture mixte tardive. Trentecinq sujets avaient des canines incluses en palatin (uni ou bilatérales) identifiées à l’aide de radiographies panoramiques (groupe PDC) et 50 sujets présentaient une evolution normale de l’éruption de la canine permanente supérieure comme le montrent les radiographies panoramiques (groupe non- PDC). Comparaison des mesures angulaires et linéaires des céphalogrammes latéraux et en même temps des radiographies panoramiques entre le groupe PDC et le groupe non-PDC, à des fins statistiques. Résultats: Toutes les mesures angulaires qui comprenaient l’axe principal de la canine (plan horizontal de Francfort, plan palatin, ou bien l’axe de l’incisive centrale) faisaient état de valeurs nettement plus faibles dans le groupe PDC (p. <0,001). En termes de mesures linéaires, la distance de l’apex de la canine à l’axe vertical de l’incisive centrale parallèle au plan horizontal de Francfort et la distance de l’apex de la canine au bord alvéolaire antérieur parallèle au plan horizontal de Francfort faisaient état de valeurs nettement plus élevées chez les sujets PDC que dans le groupe de contrôle. Par contre, la distance verticale de l’apex de la canine au plan occlusal fonctionnel ne montrait aucune différence significative entre le groupe PDC et le groupe non-PDC. Conclusions: Un diagnostic précoce de canine incluse en palatin est fondamental dans le but d’éviter l’apparition d’une inclusion de canine. Si l’imagerie en 3D d’une canine incluse ne peut être obtenue, un céphalogramme latéral peut s’avérer un bon outil pour une détection précoce de PDC dans la denture mixte tardive. L’angle entre l’axe vertical de la canine et le plan palatin ont une valeur de diagnostic lorsqu’on aborde des situations de canines incluses en palatin. A cet effet, des valeurs inférieures à 102 degrés peuvent indiquer la présence de canines incluses en palatin. Resumen Objetivos: Se realizó este estudio controlado prospectivo para determinar el papel que el cefalograma lateral puede jugar en la detección de caninos impactados por palatino (PDCs). Materiales y métodos: el estudio abarcó a 85 sujetos en la fase de dentición mixta tardía. Treinta y cinco sujetos tenían caninos impactados por palatino (unilateral o bilateral), identificados por radiografias panorámicas (Grupo PDC) y 50 sujetos presentaban un camino normal de la erupción del canino superior permanente como se desprendía de las radiografías panorámicas (grupo no-PDC). Se llevó a cabo la comparación de las mediciones lineales y angulares de los cefalogramas laterales y al tiempo de las radiografías panorámicas entre el grupo PDC y el grupo no-PDC a fines estadísticos. Resultados: Todas las mediciones angulares que abarcaban el eje principal del canino (plano horizontal de Frankfort, plano palatal, o eje del incisivo central) resultaron tener valores netamente inferiores en el grupo PDC (p<0.001). En términos de mediciones lineales, tanto la distancia del tip del canino al eje vertical del incisivo central paralelo al plano horizontal de Frankfort y la distancia del tip del canino al margen alveolar anterior paralelo al plano horizontal de Frankfort experimentaron valores significativamente más altos en los sujetos con caninos impactados por palatino que en el grupo de control. En cambio, la distancia vertical del tip del canino al plano oclusal funcional no experimentó diferencia significativa entre el grupo PDC y el grupo no-PDC. Conclusiones: Un diagnóstico precoz de PDC es básico para evitar la aparición de una impactación de canino. Si no es posible conseguir imágenes en 3D de un canino impactado, un cefalograma lateral 48 progress in orthodontics 1 3 ( 2 0 1 2 ) 42–48 puede ser una buena herramienta para una detección temprana de PDC en la dentición mixta tardía. El ángulo entre el eje vertical del canino y el plano palatino demuestra que tiene valor de diagnóstico cuando se valoren situaciones de caninos impactados por palatino. Valores inferiores a 102 grados pueden indicar presencia de PDC. references 1. Peck S, Peck L, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod 1994;64:249–56. 2. Jacoby H. The etiology of maxillary canine impactions. A clinical and radiologic study. Am J Orthod 1983;84:125–32. 3. Baccetti T. A controlled study of associated dental anomalies. Angle Orthod 1998;68:267–74. 4. Peck S, Peck L, Kataja M. Site-specificity of tooth maxillary agenesis in subjects with canine malpositions. Angle Orthod 1996;66:473–6. 5. Baccetti T, Franchi L, De Lisa S, Giuntini V. Eruption of the maxillary canines in relation to skeletal maturity. Am J Orthod Dentofacial Orthop 2008;133:748–51. 6. Baccetti T, Mucedero M, Leonardi M, Cozza P. Interceptive treatment of palatal impaction of maxillary canines with rapid maxillary expansion: A randomized clinical trial. Am J Orthod Dentofacial Orthop 2009;136:657–61. 7. Sigler LM, Baccetti T, McNamara Jr JA. Effect of rapid maxillary expansion and transpalatal arch treatment associated with deciduous canine extraction on the eruption of palatally displaced canines: A 2-center prospective study. Am J Orthod Dentofacial Orthop 2011;139:e235–44. 8. Ericson S, Kurol J. Resorption of incisors after ectopic eruption of maxillary canines. A CT study. Angle Orthod 2000;60:415–23. 9. Ericson S, Bjerklin K, Falahat B. Does the canine dental follicle cause resirption of permanent incisor roots? A computed tomographic study of erupting maxillary canines. Angle Orthod 2002;72:95–104. 10. Rimes RJ, Mitchell CNT, Willmot DT. Maxillary incisor root resorption in relation to the ectopic canine: A review of 26 patients. Eur J Orthod 1997;19:79–84. 11. Ericson S, Kurol J. Radiographic examination of ectopically erupting maxillary canines. Am J Orthod Dentofacial Orthop 1987;91:483–92. 12. Bishara SE. Impacted maxillary canines: A review. Am J Orthod Dentofacial Orthop 1992;101:159–71. 13. McSherry PF. The ectopic maxillary canine: A Review. Brit J Orthod 1998;25:209–16. 14. Barlow ST, Moore MB, Sheriff M, Ireland AJ, Sandy JR. Palatally impacted canines and the modified index of orthodontic treatment need. Eur J Orthod 2009; 31:362–6. 15. Baccetti T, Crescini A, Nieri M, Rotundo R, Pini Prato GP. Orthodontic treatment of impacted maxillary canines: an appraisal of prognostic factors. Prog Orthod 2007; 8:6–15. 16. Ericson S, Kurol J. Early treatment of palatally erupting maxillary canines by extraction of the primary canines. Eur J Orthod 1988;10:283–95. 17. McConnell TL, Hoffmann DL, Forbes DP, Janzen EK, Weintraub NH. Maxillary canine impaction in patients with transverse maxillary deficiency. ASDC J Dent Child 1996;63:190–5. 18. Olive RJ. Orthodontic treatment of palatally impacted maxillary canines. Aust Orthod J 2002;18:64–70. 19. Baccetti T, Leonardi M, Armi P. A randomized clinical study of two interceptive approaches to palatally displaced canines. Eur J Orthod 2008;30:381–5. 20. Ericson S, Kurol J. Radiographic assessment of maxillary canine eruption in children with clinical signs of eruption disturbance. Eur J Orthod 1986;3:133–40. 21. Kettle MA. Treatment of the unerupted maxillary canine. Trans Brit Soc Study Orthod 1957:74–84. 22. Ericson S, Kurol J. Longitudinal study and analysis of clinical supervision of maxillary canine eruption. Comm Dent Oral Epid 1986;14:172–6. 23. Orton HS, Garvey MT, Pearson MH. Extrusion of the ectopic maxillary canine using a lower removable appliance. Am J Orthod Dentofacial Orthop 1995;107:349–59. 24. Baccetti T, Franchi L, McNamara Jr JA. The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Semin Orthod 2005;11:119–29. 25. Bishara SE, Kommer DD, McNeil MH, Montagano LN, Oesterle LJ, Youngquist W. Management of impacted canines. Am J Orthod 1976;69:371–87. 26. Dahlberg G. Statistical Methods for Medical and Biological Students. New York: Interscience Publications; 1940. 27. Cohen J. A power primer. Psychol Bullet 1992; 112:155–9.