Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
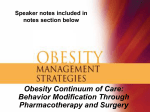
DN McKay.qxp 11/11/09 11:02 Page 1 D RUG N OTES Sibutramine H Venkataraman, G McKay* Introduction Sustained weight loss of 5–10% in the obese individual confers health benefits. Current strategies in the management of obesity include lifestyle interventions and pharmacotherapy. At present, two drugs have been approved for the medical management of obesity: sibutramine and orlistat. Sibutramine (Meridia, Reductil) belongs to a group of drugs called seratonin norepinephrine re-uptake inhibitors (SNRIs) which includes other drugs such as the antidepressant venlafaxine. Sibutramine was initially investigated for its antidepressant properties but a serendipitous discovery in 1995 showed that this novel antidepressant had effects on weight loss, leading to its development as an anti-obesity drug. Pharmacology Figure 1 outlines the pharmacological action of sibutramine. Sibutramine hydrochloride monohydrate is a centrally acting SNRI. It inhibits neuronal re-uptake of the neurotransmitters 5HT (5-hydroxytryptamine, serotonin), norepinephrine and dopamine. Its action on weight loss is mainly through inhibition of 5HT and norepinephrine re-uptake in the hypothalamus which controls hunger and satiety. It increases 5HT and norepinephrine levels in the synaptic cleft without stimulating an increased release from neurons, so avoiding neuronal depletion of these neurotransmitters. It is well absorbed from the gastrointestinal tract and undergoes extensive first pass metabolism into two active amine metabolites M1 and M2 which are about 100 times more potent and longer acting, allowing for once-daily dosing. About 85% is excreted in the urine and faeces. The Dr Hema Venkataraman, MRCP, Specialty Trainee (ST3), Endocrinology and Diabetes, Doncaster Royal Infirmary, Doncaster, UK Dr Gerry McKay, BSc(Hons), FRCP, Figure 1. The pharmacological action of sibutramine Sibutramine blocks Re-uptake 5HT Norepinephrine Satiety Synapse NOTES. Sibutramine inhibits neuronal re-uptake of the neurotransmitters 5HT (5-hydroxytryptamine, serotonin), norepinephrine and dopamine. Its action on weight loss is mainly through inhibition of 5HT and norepinephrine re-uptake in the hypothalamus which controls hunger and satiety. side effects of sibutramine include dry mouth, anorexia, insomnia, and increases in the pulse rate and blood pressure (BP), in part due to the peripheral sympathomimetic action. Trials of safety and efficacy Several randomised controlled trials have demonstrated the efficacy of sibutramine in combination with lifestyle measures over placebo. The LOSE Weight study recruited 588 obese patients who were undergoing a weight management programme.1 Patients were randomly assigned to participate in the programme alone, or to take part in the programme and receive sibutramine for 12 months. The mean weight loss was greater in the sibutramine treated group, being -6.8kg (95% CI -7.4 to -6.1kg) vs -3.1kg (95% CI -3.8 to -2.4kg); p<0.001. There were significantly greater decreases in the percentage weight loss, BMI, percentage body fat and waist circumference. Significantly more people showed >5% weight loss Consultant Physician, Medical Directorate, Glasgow Royal Infirmary, Glasgow UK in the drug group (47.3% vs 19.1%) at 12 months. In this study there were no significant changes in BP but there was a significant increase in heart rate (1.7bpm [95% CI 0.5–2.9bpm] vs -0.4bpm [95% CI -1.5 to 0.8bpm]; p<0.004) in the sibutramine group. The STORM study was a doubleblind, randomised controlled trial that investigated maintaining weight loss after an initial six months of treatment with sibutramine 10mg/day in conjunction with a low calorie diet in 605 obese patients (BMI 30–45).2 Of the 499 patients entering the trial, 467 (77%) showed >5% weight loss after the initial six months of treatment. Patients with >5% weight loss were randomised to receive either sibutramine or placebo for 18 months. Forty-three percent of sibutramine treated patients maintained >80% of their weight loss compared to 16% in the placebo group (odds ratio 4.64, p<0.001); 69% of the sibutramine treated group maintained at least 5% weight Glasgow Royal Infirmary, Castle Street, Glasgow G4 0SF, UK; e-mail: [email protected] *Correspondence to: Dr Gerry McKay, Consultant Physician, Wards 29 & 30, Pract Diab Int November/December 2009 Vol. 26 No. 9 Copyright © 2009 John Wiley & Sons 381 DN McKay.qxp 11/11/09 11:02 Page 2 D RUG N OTES Sibutramine loss and 46% maintained a 10% weight loss. Therefore the STORM study showed that sibutramine was efficacious in maintaining weight loss for up to two years after the start of therapy. Twenty (3%) patients were withdrawn because of increases in BP; in the sibutramine group, systolic BP (SBP) rose from baseline to two years by 0.1mmHg (SD 12.9), diastolic BP (DBP) by 2.3mmHg (9.4), and pulse rate by 4.1bpm (11.9). The ongoing SCOUT trial is a large-scale, randomised, doubleblind comparison of sibutramine vs placebo to specifically assess the cardiovascular risks in obese subjects who are at increased risk of cardiovascular disease, including patients with diabetes.3 The trial recruited 10 742 patients with cardiovascular risks – including hypertension, diabetes, coronary artery disease and strokes. In the six-week lead in period normotensive patients with little weight loss had moderate increases in both SBP and DBP, while in those who had most weight loss and who were hypertensive the SBP and DBP decreased. The mean increase in heart rate was 4–7bpm. rate increased significantly more with sibutramine, being ≥10bpm higher in 42% of treated patients vs 17% with placebo (p<0.01). A 24-week double-blind, multicentre trial of 175 obese, poorly controlled patients with type 2 diabetes showed significantly greater weight loss (p<0.01) in those randomised to sibutramine.5 Weight loss (>5% and >10%) was achieved in 33% and 8% of patients on sibutramine but not in placebo patients. Improvement in glycaemic control correlated with weight loss (p<0.001). In 5% and 10% weight-loss responders the HbA1c differences were -0.53% and -1.65% respectively (p≤0.05). Sibutramine also showed favourable differences in HDL, triglycerides, insulin and fasting blood glucose. Sibutramine treatment was associated with small mean increases in BP and pulse, although an increase in BP was not seen in sibutramine treated patients who lost ≥5% of their weight. In the SCOUT trial,3 BP reductions were greater for those with diabetes who were hypertensive and/or lost the most weight (>5%). Specific evidence for use in diabetes A randomised, prospective, placebocontrolled, double-blind study was conducted over 12 months in 195 obese patients with type 2 diabetes on metformin.4 Sibutramine was shown to produce significant weight loss (p<0.01). More than 10% weight loss was seen in 14% and 27% of those receiving 15 and 20mg respectively, but none in the placebo group. Glycaemic control paralleled the decrease in weight loss. Patients with >10% weight loss had a significant decrease in HbA1c (-1.2±0.4%, p<0.0001) and fasting plasma glucose (-1.8mmol/L). HDL increased and plasma triglycerides decreased, especially in patients with >10% weight loss (p<0.01). Treatment was generally well tolerated. Sibutramine treatment raised sitting DBP by ≥5mmHg in a higher proportion of patients than did placebo (43% with 15mg/day vs 25% with placebo, p<0.05), but this effect was less evident in subjects who had a weight loss of ≥10% weight. Pulse Discussion Sibutramine has been shown to produce statistically significant weight loss, maintain long-term weight loss and produce favourable metabolic changes in obese patients with type 2 diabetes. Although sibutramine has been shown to promote weight loss, concerns over cardiovascular adverse effects have limited its market penetration. Notably, the Italian regulatory authority temporarily suspended marketing authorisation of sibutramine in 2002, citing 50 adverse reactions, including two cardiovascular-related deaths. The European Committee for Proprietary Medicinal Products and the Health Sciences Authority (UK) subsequently conducted independent reviews of sibutramine and concluded that the risk–benefit profile remains positive. NICE recommends sibutramine in those with a BMI >27 with cardiovascular risk factors, and in those with a BMI >30 without cardiovascular risk factors. Pulse and BP should be monitored regularly. Sibutramine should be continued for 382 Pract Diab Int November/December 2009 Vol. 26 No. 9 Key points • Sibutramine is a drug that can be used to facilitate weight loss in obese patients, including those with type 2 diabetes mellitus • The response to treatment should be reviewed on a regular basis and the drug discontinued if no efficacy is demonstrated • Although side effects of increased pulse and blood pressure are to be anticipated, this is not a major issue as long as the patients are carefully selected and monitored appropriately more than three months only if there is a weight loss >5%. Currently, it is not licensed for use for longer than 12 months. Conflict of interest statement There are no conflicts of interest. References 1. Porter JA, Raebel MA, Conner DA, et al. The Long-Term Outcomes of Sibutramine Effectiveness on Weight (LOSE Weight) study: evaluating the role of drug therapy within a weight management program in a groupmodel health maintenance organization. Am J Manag Care 2004; 10: 369–376. 2. James WP, Astrup A, Finer N, et al. Effect of sibutramine on weight maintenance after weight loss: a randomised trial. STORM Study Group. Sibutramine Trial of Obesity Reduction and Maintenance. Lancet 2000; 356: 2119–2125. 3. Van Gaal LF, Caterson ID, Coutinho W, et al., on behalf of the SCOUT Investigators. Weight and blood pressure response to weight management and sibutramine in diabetic and nondiabetic high-risk patients: an analysis from the 6-week lead-in period of the sibutramine cardiovascular outcomes (SCOUT) trial. Diabetes Obes Metab 2009 Sep 16. [Epub ahead of print.] 4. McNulty SJ, Ur E, Williams G; Multicenter Sibutramine Study Group. A randomized trial of sibutramine in the management of obese Type 2 diabetic patients treated with metformin. Diabetes Care 2003; 26: 125–131. 5. Fujioka K, Seaton TB, Rowe E, et al. Weight loss with sibutramine improves glycaemic control and other metabolic parameters in obese patients with type 2 diabetes mellitus. Diabetes Obes Metab 2000; 2: 175–187. Copyright © 2009 John Wiley & Sons