Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
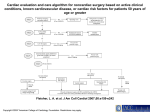
Focusing on the Surgical Patient with Cardiac Problems By Kate J. Morse, RN, ACNP-BC, CCRN Nursing2009, March 2009 2.1 ANCC contact hours Online: www.nursingcenter.com © 2009 Lippincott Williams & Wilkins. All world rights reserved. Significance Baby boomers born 1946-1964 will be increasingly greater consumers of healthcare in the coming decades 39% of these patients will have cardiovascular disease American College of Cardiology/American Heart Association (ACC/AHA) have established guidelines for perioperative cardiovascular evaluation Preoperative evaluation Determines cardiovascular risk Additional testing may be done Surgeon and anesthesiologist will examine patient Nurse can perform health history and physical assessment Questions to ask patient Do you experience chest pain? Do you take nitroglycerin? Do you need to rest between taking a shower and dressing? Can you walk up a flight of stairs? Have you stopped an activity due to symptoms? Do you have swelling or pain in your feet, legs? Does anyone in your family have heart trouble? Physical assessment Take BP in both arms, checking for artery stenosis Assess carotid pulses for bruits Auscultate lungs and heart sounds Examine extremities for edema and signs of peripheral vascular disease Conditions to treat Active cardiac conditions, which should be treated before noncardiac surgery, include: acute coronary syndromes decompensated heart failure significant dysrhythmias (high-grade atrioventricular blocks and symptomatic ventricular dysrhythmias), supraventricular dysrhythmias (poorly controlled atrial fibrillation, symptomatic bradycardia, ventricular tachycardia) severe valvular heart diseases (severe aortic stenosis or symptomatic mitral stenosis) Guidelines Make a distinction between: - history of myocardial infarction (MI) - abnormal Q waves on a 12-lead ECG - an acute MI Irreversible myocardial necrosis (history of MI or abnormal Q waves) is considered a clinical risk factor Guidelines Active cardiac condition is defined as: - an acute MI 7 days or less before the exam - a recent MI occurring more than 7 days ago but less than or equal to a month ago with evidence of ischemic risk by clinical symptoms or noninvasive study Low cardiac risk Patient with recent MI but no further risk with stress test Elective surgery may still be postponed 4 to 6 weeks after the MI Body systems linked to increased cardiac risk Pulmonary: lung disease increases patient risk of complications Evaluate risk with: - accurate smoking history - pulmonary function tests (PFTs) - arterial blood gas analysis - chest X-ray Diabetes Most common metabolic disease Can complicate surgery These patients often have undiagnosed coronary artery disease (CAD) Tight glycemic control is key - glucose below 200 is target Kidney disease Can be associated with cardiac disease Preoperatively patient’s renal function will be assessed with lab tests: - blood urea nitrogen - creatinine clearance - glomerular filtration rate Fluid and electrolyte levels will be monitored and balanced in someone who’s renally impaired Hematologic disorders Anemia places stress on cardiovascular system If complete blood cell count reveals anemia, blood transfusion risk will be assessed by surgeon Hypercoagulability conditions (polycythemia, thrombocytopenia) put patient at risk for clotting and should be addressed preoperatively Step-by-step approach for surgical risk Determine urgency of surgery - emergent surgery, cardiologist will make recommendations - if elective, may be delayed or postponed Evaluate patient for active cardiac conditions Step-by-step approach for surgical risk Evaluate surgical risk - is the procedure low, intermediate, or high risk? Evaluate patient’s functional capacity - done subjectively by asking patient questions regarding activities of daily living - stress test Step-by-step approach for surgical risk Evaluate clinical risk factors - patient has symptoms - unknown functional capacity Clinical risk factors include - history ischemic heart disease - history heart failure - history cerebral vascular disease - diabetes - renal disease Recommendations If no clinical risk factors, surgery can proceed If one or two clinical risk factors, surgery can proceed with beta-blocker therapy; additional testing should be considered If three or more clinical risk factors, consider cardiac risk; additional testing shouldn’t be done if it won’t change plan of care Cardiac risks in noncardiac surgery The guidelines stratify surgical risk according to three levels: Vascular (cardiac risk greater than 5%) - Major vascular procedures such as aortic repair - Peripheral vascular surgery Cardiac risks in noncardiac surgery Intermediate risk (1% to 5%) - Intraperitoneal and intrathoracic surgery - Head and neck surgery - Carotid endarterectomy - Orthopedic surgery - Prostate surgery Cardiac risks in noncardiac surgery Low risk (less than 1%) - Endoscopic procedures - Superficial procedures - Cataract surgery - Breast surgery - Ambulatory surgery Diagnostic tests Exercise stress test is first choice unless contraindicated Pharmacologic stress test if unable to walk or exercise Coronary arteriograph - invasive test evaluates coronary anatomy Cardiac revascularization May be done prior to elective noncardiac surgery For severe multivessel disease or significant left main CAD Two options - coronary artery bypass graft or percutaneous coronary intervention (PCI) with bare-metal or drug-eluting stents Surgery post PCI Elective surgery should be delayed 4 to 6 weeks after PCI with bare-metal stents Delay 12 months after drug-eluting stents Medications post PCI (aspirin, Plavix) put patient at risk for bleeding If patient underwent balloon angioplasty, elective noncardiac surgery isn’t recommended for 4 weeks Medications and surgery Aspirin and Plavix therapy increase risk of bleeding Beta-blockers should be continued If patient has one or more clinical risk factors, beta-blockers should be started preoperatively if not taking already Medications and surgery A patient having vascular surgery should be started on a statin Statins may also be considered in patients in patients with one clinical risk factor having an intermediate risk procedure Uncontrolled hypertension or CAD patients may need a alpha-agonist Other presurgical considerations Patients with implanted pacemakers or cardioverters should alert anesthesiologist/ surgeon so appropriate safety precautions are taken