Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
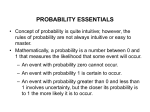
Inside Physio The Science Behind Defibrillation Energy The Physio-Control team develops all of our defibrillators with escalating energy up to 360 joules, because clinical evidence shows that higher energy gives patients the best chance of surviving cardiac arrest. There are many conflicting claims regarding defibrillation energy, but Physio-Control relies on science to guide our products’ clinical capabilities. Physio-Control products have been studied in twice as many cardiac arrest patients as all other manufacturers’ combined (as of April 2011). We turned to Fred Chapman, director of research at Physio-Control, for a look at the science behind defibrillation energy. He holds a PhD. in biomedical engineering and a master’s degree in electrical engineering. He has worked at Physio-Control since 1993. Fred Chapman Director of Research, Physio-Control Electricity and the Heart How Defibrillators Deliver Energy Understanding defibrillation energy starts with an understanding of electricity in the heart. A healthy heart has a built-in natural pacemaker that fires off synchronized electrical impulses. Electrical conduction choreographs the contractions of muscle fibers, resulting in coordinated rhythmic contractions of the heart to pump blood throughout the body. The energy a defibrillator delivers is measured in joules. The amount of energy in a shock depends on voltage, current and duration of the shock. Both peak current and how current levels rise and fall during the shock matter. Delivery of a shock can defibrillate the heart, stopping the electrical chaos and allowing the heart to resume a coordinated rhythm. Electrode pads are positioned on the chest on either side of the heart. A defibrillator supplies the electrical charge to create an electrical circuit between the electrodes. Current passes through the chest, and some of it passes through the heart. “A successful shock makes everything go quiet for a moment,” says Chapman. Stopping the lethal rhythm gives the cells of the heart a chance to reset. “For defibrillation to be successful,” he explains, “you have to expose the majority of the myocardium to an electrical field that is strong enough and you have to maintain that field long enough to extinguish the chaotic electrical activity. “That aspect of defibrillation is known as the critical mass theory,” he continues. “There’s a whole field of study trying to understand physiologically how the heart fibrillates and defibrillates. There’s no one theory that stands up to all the data. But the critical mass theory is one that guides the thinking of this science.” 30 20 Current (A) In ventricular fibrillation (VF), one of the most common causes of sudden cardiac arrest (SCA), the normally organized rhythm becomes chaotic, resulting in erratic, ineffective contraction of muscle fibers. How the flow of electrical current changes during the defibrillation shock is shown on a graph as a waveform. It depicts the level of current (measured in amps) at each millisecond during the shock, the peak current, how abruptly the current rises and falls and the duration of the shock. 10 0 -10 -20 -2 0 2 4 6 8 10 12 14 16 18 20 Time (ms) This graph compares waveforms of 200-joule shocks from different manufacturer devices: Physio-Control and ZOLL. Despite different waveforms, shocks of the same energy provide the same success rate (96%) in terminating VF. 1,2,3 PHYSIO-CONTROL® ZOLL® 200J 96% Efficacy (184/192) 200J 96% Efficacy (188/195) The portion of the waveform below the baseline indicates the current flow is reversed, as happens in a biphasic shock (more on that in a moment). Chapman points out that there are two different ways to increase the peak current of a shock: • Increase the amplitude of the whole waveform by increasing the energy setting of the defibrillator; this will increase the defibrillation efficacy, or • Change the shape of the waveform so that the high point of the current waveform “sticks up” higher; this could result in higher, equal or lower efficacy. Defibrillators from different manufacturers deliver the electrical current during a shock in different ways, so their waveforms have different shapes. “In theory,” says Chapman, “different shape waveforms could have different efficacy at the same energy settings. But when you actually look at the clinical data for the leading biphasic waveforms, you see that for the same energy you get the same efficacy up to 200 joules.” Five independently conducted, peer-reviewed clinical studies1-5 comparing biphasic waveforms on the market found that shocks of the same energy provide the same success rate in terminating shockable heart rhythms. The flow of electricity can be compared to water flowing through a pipe. Think of current (measured in amperes) as the flow of water, and voltage (measured in volts) as the pressure that pushes that water along. Power (measured in watts) is equal to the product of current and voltage at each point in time. The total energy of the shock is calculated by adding up that power over the duration of the shock. One joule equals one watt times one second. Shock Success Although a single shock works for the majority of patients, many others need more than one shock. “When we look at the scientific literature, we see that some studies report a first shock success rate in the 90% range, while others are in the 70% range,” Chapman says. “If it’s in the 70% range, that means one out of four times you’re not terminating VF and you have to go back and try it again.” Unfortunately, there’s currently no way to know which patients are going to need more than one shock. For example, you might expect worse shock success in heavily muscled or obese patients, who have high impedance or resistance to current flow. But that’s not necessarily the case. “It’s one of those things you can only learn by gathering a lot of data,” Chapman says. “We have looked at large sets of clinical data, and in patients with high, low or average impedance, shock success rates are the same. That’s counter to what we expected and we don’t completely understand it. Perhaps our impedance compensation technology is working even better than we expected. Bottom line: there are patients that are more difficult to defibrillate and we now know that impedance cannot predict which ones those will be.” Delivering a Therapeutic Dose of Energy The charged particles flowing in an electric current seek the easiest path between electrodes on the patient’s chest. Ideally, that path deliv- ers enough current through the heart to stop VF—to deliver a therapeutic dose. Sometimes too much of the current flows around the heart however, as happens if electrodes are positioned poorly. Current flow to the heart may also be reduced, Chapman explains, due to the shape of the patient’s chest, a large amount of air in the lungs or fluid leaking into interstitial space, creating very conductive tissue. Continuing research is shedding light on other factors that make some patients harder to defibrillate. For example, Chapman points to a recent study with internal pacemakers that found chronic cocaine users are harder to defibrillate. It may be that drug use affects the properties of the cells themselves, making them harder to depolarize. “Many of these factors you don’t have much control over,” notes Chapman. “You do have control over energy settings and how well you place the electrodes.” If a Shock Fails “The single most effective way to increase your chance of successful defibrillation after a shock fails is to make the next shock a higher energy shock,” says Chapman. “Changing energy setting changes the amplitude of the wave form. With higher energy, at every point during that shock you get higher current amplitude. You also get a higher chance of success. Dose response is an important way to think of it,” he says. “For a given device, as you turn up the setting (joules) you are increasing the probability that you’ll successfully terminate VF.” Because the scientific evidence shows that defibrillation probability increases with each energy dose, all Physio-Control defibrillators have default escalating settings of 200J-300J-360J. The Switch to Biphasic Energy Biphasic waveforms are now the standard of care, but when external defibrillators were first introduced, energy was delivered in monophasic waveform. Biphasic waveforms reverse the direction of current flow partway through the shock, Chapman explains, while monophasic shocks deliver all of the current in one direction (from one electrode to the other). Cells respond differently to biphasic waveforms compared to monophasic waveforms. “With biphasic, you are able to have the desired effect on myocardial cells with a less strong field,” Chapman says, “so the same strength shock has a higher success rate in terminating VF.” In transitioning from monophasic to biphasic waveforms, manufacturers had a choice of two approaches, says Chapman: “Apply less energy to hopefully get the same success rate as with monophasic waveforms or keep the same energy level (360J, the standard monophasic dose) and know your shock success rate will increase.” Physio-Control chose to maintain energy capability up to 360J, leveraging both the known improved efficacy of biphasic waveforms and their significantly lower risk of shock-related injury compared to monophasic waveforms. Other manufacturers chose instead a lower energy capability for their defibrillators, and they made that choice without clinical data from the type of patients typically treated with these devices, notes Chapman. The clinical data subsequently gathered bear out Physio-Control’s approach, showing that increasing the dose of subsequent shocks is more effective for terminating VF than simply repeating a failed dose. High Energy Without Higher Risk There’s no clinical evidence behind claims that biphasic shock energies higher than 200J will damage the heart—claims made by manufacturers who limit their defibrillation energy to 200J. Although studies in the 1980s with monophasic shocks found some evidence of injury with shocks over 300J, it is important to recognize that biphasic shocks expose the heart to much less current than monophasic shocks. For example, a 360J biphasic shock from a Physio-Control device exposes the patient to roughly the same peak current intensity as a 100J monophasic shock. “A good body of clinical evidence has failed to show injury from shocks all the way up to 360J biphasic,” says Chapman. Clinical studies of both atrial fibrillation (AF)3 and VF6 show no evidence of cardiac damage with 360J biphasic shocks, even when researchers specifically looked for it, as evidenced by cardiac enzyme levels, heart ejection fractions and ECG ST-segment elevation. “Cardiac arrest itself causes injury,” Chapman explains. “Anyone who has been through minutes without blood flow to the heart tissue has injury to the heart. To measure the damage that might be from delivery of electric current is really difficult. But the best evidence we have is that the injury to the heart is much more related to how long the heart was without blood flow or oxygen. By defibrillating effectively, we hope to decrease the length of that interval.” REFERENCES 1. Alatawi F, et al. Heart Rhythm. 2005; 2(4): 382-87. 2. Kim ML, et al. Am J Cardiol. 2004; 94(11): 1438-40. 3. Neal S, et al. Am J Cardiol. 2003; 92(7): 810-14. 4. Deakin CD, et al. Circulation. 2011; 124(21 Suppl): A244. 5. Santomauro M, et al. Ital Heart J Suppl. 2004; 5(1): 36-43. 6. Stiell IG, et al. Circulation. 2007; 115: 1511-1517. For further information, please contact Physio-Control at 800.442.1142 (U.S.), 800.895.5896 (Canada) or visit our website at www.physio-control.com. Physio-Control Headquarters Redmond, WA 98052 www.physio-control.com Customer Support P. O. Box 97006 Redmond, WA 98073 Toll free 800 442 1142 Fax 800 426 8049 ©2012 Physio-Control, Inc. GDR 3312661_A Physio-Control Canada Physio-Control Canada Sales, Ltd. 7111 Syntex Drive, 3rd Floor Mississauga, ON L5N 8C3 Canada Toll free 800 895 5896 Fax 866 430 6115