Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
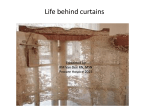
Authors: Lisa A. Lombard, MD Ross D. Zafonte, DO Brain Injury Affiliations: From the Department of Physical Medicine and Rehabilitation, University of Pittsburgh, The University of Pittsburgh Medical Center–Institute for Rehabilitation and Research, Pittsburgh, Pennsylvania. Correspondence: All correspondence and requests for reprints should be addressed to Ross D. Zafonte, DO, University of Pittsburgh, Rehabilitation, Kaufmann Medical Building, 3471 Fifth Avenue, Suite 201, Pittsburgh, PA 15213. 0894-9115/05/8410-0797/0 American Journal of Physical Medicine & Rehabilitation Copyright © 2005 by Lippincott Williams & Wilkins DOI: 10.1097/01.phm.0000179438.22235.08 INVITED REVIEW Agitation After Traumatic Brain Injury Considerations and Treatment Options ABSTRACT Lombard LA, Zafonte RD: Agitation after traumatic brain injury: Considerations and treatment options. Am J Phys Med Rehabil 2005;84:797– 812. Posttraumatic agitation is a challenging problem for acute and rehabilitation staff, persons with traumatic brain injury, and their families. Specific variables for evaluation and care remain elusive. Clinical trials have not yielded a strong foundation for evidence-based practice in this arena. This review seeks to evaluate the present literature (with a focus on the decade 1995–2005) and employ previous clinical experience to deliver a review of the topic. We will discuss definitions, pathophysiology, evaluation techniques, and treatment regimens. A recommended approach to the evaluation and treatment of the person with posttraumatic agitation will be presented. The authors hope that this review will spur discussion and assist in facilitating clinical care paradigms and research programs. Key Words: Traumatic Brain Injury, Agitation, Delirium, Behavior O ne of the more frustrating aspects of care of persons with traumatic brain injury (TBI) is in the management of the agitated patient; agitated patients may resist direct care, be disruptive on the unit, or even pose a physical risk to themselves, family, or staff. A specific definition of agitation remains elusive; some have described it as a variation of delirium. It may include inappropriate vocalizing, intolerance of medical management or equipment, and directed or diffuse aggressive behaviors. Careful consideration of environmental factors should be given before medicating a person with agitation. When medications are eventually pursued to modulate behavior, measurement of agitation with an objective tool is highly recommended in determining the success of treatment. DEFINITIONS/SCOPE The Rancho Los Amigos scale1 describes agitation as a component of the fourth stage of recovery; however, some patients are noted to progress from localized responses to confusion and consciousness without any stage of aggression. Agitation does seem to correlate with lower cognitive status, as found by Corrigan and Mysiw2 in an examination of 18 persons with TBI. Ten of the 18 patients were found to be agitated. In a study of 28 persons with brain injury due to stroke, trauma, or anoxia in a rehabilitation facility, 39% were found to October 2005 Agitation After Traumatic Brain Injury 797 demonstrate some aggressive behaviors within the first week of admission. There was a significant correlation between these behaviors and severity of injury and disorientation to time and place.3 In a study that used a strict definition of agitation, only 11 of 100 rehabilitation inpatients with severe TBI were found to be agitated, and 35 were determined to experience restlessness. In the majority of persons with agitation, the symptoms resolved within a week.4 In contrast, a more recent study5 examined agitation in a cohort of 158 persons with TBI in an inpatient rehabilitation setting; 50% of their sample experienced agitation, but it typically lasted ⬍10 days. No difference was noted in agitation with regard to sex. Some of the variation in the reports of frequency of posttraumatic agitation may be a result of a lack of consensus of the specific definition of the term. A group in 1997 attempted to determine clinicians’ definitions of agitation; a survey was performed of members of the Brain Injury Special Interest Group of the American Academy of Physical Medicine and Rehabilitation.6 The factors of physical aggression, explosive anger, increased psychomotor activity, impulsivity, verbal aggression, disorganized thinking, perceptual disturbances, and reduced ability to maintain or appropriately shift attention were noted by ⱖ50% of respondents to be either “very important” or “essential” to the definition of agitation. There was no consensus as to whether agitation was, by its nature, limited to the period before clearing posttraumatic amnesia or if it could extend past that time and thus be a chronic issue. The unification of the definition of agitation is highly recommended; the ability to compare or replicate studies depends on a common language describing this condition. We suggest that posttraumatic agitation be defined as a state of aggression during posttraumatic amnesia. This state occurs in the absence of other physical, medical, or psychiatric causes. It can be manifested by intermittent or continuous verbal or physical behaviors and can be identified by a score of ⱖ22 on the Agitated Behavior Scale.7 Akathisia, which can be seen during recovery from TBI, carries a more standardized definition.8 It describes a constant sense of inner restlessness, which may or may not be manifested in motor activity, ranging from bouncing legs and fidgeting hands to pacing behaviors. It is not limited to brain injury specifically; it has been reported as an extrapyramidal side effect from ingestion of neuroleptic medications.9 As akathisia does not require the presence of aggression, it is thus not synonymous with agitation, although certainly could be a component of it. 798 Lombard and Zafonte PATHOPHYSIOLOGY Like definitions of agitation, the specific pathophysiology of posttraumatic aggression remains poorly understood. In determining anatomic areas associated with this behavior, three specific subtypes of aggression have been defined: social aggression, predatory aggression, and defensive aggression.10 In contrast with social and predatory aggressions, which are associated with more goaldirected acts, defensive aggression is most similar to behaviors seen in persons with TBI, in which the response is to a perceived threat, real or otherwise. In cats, the hypothalamus, periaquaductal gray, and limbic structures, such as the amygdala, hippocampus, and septal area, have been associated with this defensive rage.11 In one case report, a 14-yr-old boy with a history of aggression who had murdered was found to have a cystic lesion lateral to the right amygdala.12 Temporal lobe epilepsy has been, on rare occasions, associated with interictal aggression; a radiographic survey of persons with a history of both temporal lobe epilepsy and aggression revealed a subgroup of patients with significant amygdala and peri-amygdala atrophy.13 The importance of subclinical seizures in disorders of aggression may be underappreciated.14 From a neurochemical perspective, regulation of aggression seems to be primarily dependent on the balance of serotonin and dopamine. Exposure to a confrontational situation results in increased dopamine and decreased serotonin in normal rats.15 5HT-1b knockout mice demonstrate disinhibition and increased aggression toward other mice.16 Apomorphine, a dopamine agonist, can induce aggression in nonaggressive mice, and administration of a D2 inhibitory agent decreases aggressive behaviors in high-aggressive strains of mice.17 However, we do not suggest regular use of potent D2 inhibitors in the treatment of posttraumatic agitation, as it is fraught with the potential to slow neural recovery (see section on antipsychotic agents below). In humans, particularly low cerebrospinal fluid levels of 5-hydroxyindolacetic acid, a major metabolite of serotonin, were found in male prisoners incarcerated for impulsive, aggressive crimes.18 Nitric oxide seems to have effects on aggression, as well; male mice that lack the neuronal nitric oxide synthase gene have significantly decreased serotonin turnover and clinically demonstrate greater intraspecies aggression.19 Dopamine is also implicated in akathisia, which, as stated above, often accompanies posttraumatic agitation. Dopamine transporter gene knockout mice (DAT⫺/⫺) demonstrate increased extracellular dopamine and locomotion but show no increase in aggression.20 In a positron emission Am. J. Phys. Med. Rehabil. ● Vol. 84, No. 10 tomographic study in humans, administration of a potent D1 receptor antagonist resulted in transient akathisia in both normal controls and schizophrenic patients when receptor occupancy reached 45–59%. Similar results were seen after administration of a D2 receptor antagonist.21 To our knowledge, no study has identified a specific site or mechanism to account for posttraumatic agitation in humans; it is likely a complicated combination of structural lesions, biochemical deficits, and external factors that lead to this condition. MONITORING OF AGITATION When determining a treatment plan for an agitated patient, it is necessary to have a measurement tool to determine objectively the effectiveness of treatment. In 1989, Corrigan7 described an instrument named the Agitated Behavior Scale. This scale uses a rating of severity from 1 (absent) to 4 (present to an extreme degree) on 14 different behaviors and can be completed in 10 mins of observation. A patient with a score of ⱖ21 is defined to be agitated (Table 1). In follow-up study, the Agitated Behavior Scale was shown to have good intrarater and interrater reliability when used by research assistants and trained nursing staff in the evaluation of persons with brain injury or dementia.22 Another measurement tool described is the Overt Aggression Scale (OAS). It was originally developed in 1986 and proposed to be used as an evaluation tool for behavioral disturbance in psychiatric patients.23 The OAS focuses on recording aggressive behavior in four domains of verbal aggression and aggression against self, objects, and people. A variant of the OAS was designed in 1997 to be more appropriate for neurorehabilitation.24 The OAS-Modified for Neurorehabilitation (OASMNR) added three intervention categories, and included the ability to select from 18 events preceding the aggressive behavior. OAS-MNR was used to measure the efficacy of treatment in a case series of three persons in a neurobehavioral program.25 Unfortunately, according to a 1997 survey, less than half the brain injury specialists use objective measures of agitation in their practice.26 The potential benefit of quantitative assessment of agitation was highlighted in a study by Angelino et al.27 As a 16-yr-old boy emerged from a vegetative state to consciousness, an increase in his serial Agitated Behavior Scale scores was observed; subsequently, a decrease was noted as his cognitive status improved. A study of 46 persons in a neurobehavioral program whose aggression was measured with the OAS-MNR found that those with poor language function had more severe aggressive outbursts that were more difficult to control.28 DIFFERENTIAL DIAGNOSIS Before initiating environmental or pharmacologic management of agitation, it is essential to TABLE 1 Agitated Behavior Scale Behaviors scored as: 1. Absent: the behavior is not present 2. Present to a slight degree: the behavior is present but does not prevent the conduct of other, contextually appropriate behavior. (The individual may redirect spontaneously, or the continuation of the agitated behavior does not disrupt appropriate behavior). 3. Present to a moderate degree: the individual needs to be redirected from an agitated to an appropriate behavior, but benefits from such cuing. 4. Present to an extreme degree: the individual is not able to engage in appropriate behavior due to the interference of the agitated behavior, even when external cuing or redirection is provided. Behaviors observed: 1. Short attention span, easy distractibility, and inability to concentrate 2. Impulsive, impatient, low tolerance for pain or frustration 3. Uncooperative, resistant to care, demanding 4. Violent and/or threatening violence toward people or property 5. Explosive and/or unpredictable anger 6. Rocking, rubbing, moaning, or other self-stimulating behavior 7. Pulling at tubes, restraints, etc. 8. Wandering from treatment areas 9. Restlessness, pacing, excessive movement 10. Repetitive behaviors, motor and/or verbal 11. Rapid, loud, or excessive talking 12. Sudden changes of mood 13. Easily initiated or excessive crying and/or laughter 14. Self-abusiveness, physical and/or verbal Total score ranges from 14 to 56. October 2005 Agitation After Traumatic Brain Injury 799 address other causes of acute mental status changes. Other factors may either contribute to or be misdiagnosed as posttraumatic agitation. Infections are very common in trauma patients and may lead to delirium. Rapid catecholamine release, as occurs in hypoglycemic or hypoxic states, can result in aggressive behaviors. Although its exact cause is unclear, “sundowning” may cause increased confusion in afternoons or evenings in patients with dementia. Drug and alcohol abuse are common co-morbidities with TBI. Acute alcohol withdrawal, hallmarked by hypertension, tachycardia, hallucinations, disorientation, and agitation, can occur as late as 72 hrs after the last drink.29 Delirium tremens can be managed with benzodiazepines. The timing of opioid withdrawal is dependent on the pharmacology of the agent used. Heroin withdrawal symptoms peak at 24 – 48 hrs after last ingestion, whereas methadone withdrawal can occur in 3 days. Restlessness, abdominal pain, yawning, and piloerection may be seen. Although hallucinations and other mental status changes are rare, persons experiencing these symptoms may become agitated and violent in attempts to resume their drug of abuse. Withdrawal from benzodiazepines may be recognized by hypertension, tachycardia, diaphoresis, tremors, hyperthermia, and seizures; symptoms may begin in 2–7 days and can last as long as 3 wks. A slow taper of a long-acting benzodiazepine can be helpful in reducing symptoms.30 Epilepsy can be a common complication after TBI, but focal seizures may not be easily recognized; in a study by Vespa et al.,14 22% of persons with TBI screened with electroencephalography in the intensive care unit (ICU) setting had seizures, and 52% of those were not apparent clinically. Those in a postictal state may be confused and be misdiagnosed as having intermittent agitation. As described above, epilepsy arising from the mesial temporal lobe may be associated with confusion or anxiety and is typically followed by a confused postictal period. Endocrine dysfunction is both a common and, likely, an underdiagnosed consequence of TBI.31 Hyperthyroidism alone may result in significant anxiety and agitation;32,33 however, persons with TBI are more likely to be hypothyroidal after injury.34,35 One case report describes a TBI inpatient with persistent agitation, hyponatremia, and orthostasis. The patient was diagnosed with primary adrenal insufficiency, and his ability to participate in therapies improved after treatment.36 Hyponatremia has, in a few occasions, been associated with delirium in both ICU37 and elderly hospitalized populations.37 In persons with TBI, it seems that 800 Lombard and Zafonte isolated hyponatremia can be seen with a decrease in cognitive function.38 ENVIRONMENTAL CAUSES AND TREATMENT Acute care hospitals, especially in ICU settings,39 can be very noisy, distractible environments. Constant stimulation in the form of frequent assessment of vital signs, audible alarms, around-the-clock medication administration, constant lighting, and ambient hallway noise can result in “ICU syndrome,” an acute confusional state seen even in those without primary brain pathology.40 Although many of these distractions are necessary, every attempt should be made to reduce stimulation, especially at nighttime. In the rehabilitation setting, there is often more flexibility in scheduling rest breaks, restoration of day and night patterns, and ensuring a quiet night environment. Therapies and meals may be scheduled in an isolated area. Persons with akathisia pose additional needs; many of these patients benefit from movement and may be calmed by being wheeled or walked around the unit. Direct physical restraints, such as vest or wrist restraints, and intravenous lines may create an additional source of irritation. When possible, restraints should be minimized, or changed to noncontact restraints, such as netted beds to prevent falls and one-to-one staff supervision to prevent intravenous lines, gastrostomy tubes, and cervical collars from being pulled. Protectors or binders should be considered when clinically feasible. Patients with restraints do need to be monitored closely by staff; a recent recall of a particular brand of netted beds highlights the potential dangers of equipment when patients are left unattended.41 Maximal reduction of lines, urinary catheters, and nasogastric tubes should be attempted as soon as possible, as potentially hazardous consequences may result from manipulation of lines by the patient.42 Binders and other covers for lines provide a barrier for the patient, which may allow for reduction of restraint needs. Simple environmental alterations may reduce unwanted behaviors; in one study, the initiation of a staff education program regarding agitation and the placement of patients on a scheduled toileting program resulted in fewer verbal outbursts in a heterogeneous population in a longterm care facility.43 In addition to external factors, persons with TBI have innately disturbed sleep cycles. In one survey of persons admitted to inpatient rehabilitation after TBI, 50% described difficulty sleeping.44 Interestingly, they found that the more severe the injury, the less likely the patient reported sleep disturbance. Sleep-disordered breathing seems to be the most common disturbance noted in acute Am. J. Phys. Med. Rehabil. ● Vol. 84, No. 10 TBI.45,46 Careful monitoring of sleep cycles and quality of sleep is indicated in all persons with TBI. Pain is a well-recognized cause of agitation in demented elders.47,48 Persons with TBI have many potential pain generators: musculoskeletal injuries, spasticity, heterotopic bone, and iatrogenic causes, such as lines, tracheostomies, and gastrostomy tubes. Many associated injuries may be initially undiagnosed.49 The inability to voice pain complaints may lead to frustration and agitation. Regular monitoring of pain control, either by patient reports or by observation of behaviors is an essential component of agitation management. However, as opioids can be sedating, they should be used judiciously in this population. BEHAVIORAL MODIFICATION In addition to the above environmental alterations, structured behavioral programs may also be considered. Prigatano et al.50 provided an excellent model from which to base a behavioral program in the treatment of psychiatric disorders after TBI. They introduced the “ICAR” model: information, whereby patients or families, or both, are provided with objective information regarding the patient’s cognitive status; contingencies, whereby patients may suffer ramifications from engaging in undesirable behaviors; improving self-awareness, whereby various techniques are suggested to encourage self-monitoring of performance; relationship, whereby the psychotherapeutic relationship is used in conjunction with cognitive rehabilitation. Although there are aspects of this model that certainly would be of limited utility in persons with significant cognitive or communication impairments, there are some aspects that may aide control of behaviors in persons with TBI-related agitation. MEDICATIONS As several studies suggest that agitation in most cases may be time-limited to ⱕ10 days,4,5 a convincing argument could be made to “ride the storm” of agitation and wait for the recovery process to resolve the behavioral issues without the potential risks of medication side effects. However, with potential risk of injury to the patient or staff members and the current climate of pressure to shorten rehabilitation days, pharmacologic measures can be considered in persons with agitation refractory to environmental or behavioral modifications (as mentioned in “ENVIRONMENTAL CAUSES AND TREATMENT”). A summary of the literature of the past 10 yrs (published after 1995) of medications used for TBI-related agitation can be found in Table 2. October 2005 Anticonvulsants One of the more commonly recognized anticonvulsants in the control of behavior is valproic acid; it has long been used for the treatment of mania in bipolar disorder.51 Although it has been suggested by some as a treatment for dementiarelated agitation,52–54 a recent Cochrane database review suggests that its sedative side effects outweigh any potential benefit in this population.55 Monji et al.56 reported success in the treatment of a rapid cycling affective disorder with valproic acid in a 16-yr-old patient with a history of TBI at 4 yrs of age. In a study of five patients with TBI-related aggression who failed multiple pharmacologic treatments, valproic acid did reduce the undesirable behaviors.57 Valproic acid was shown to be efficacious in the treatment of agitation within a week of administration in 26 of 29 persons admitted to an inpatient brain injury rehabilitation unit.58 Although valproic acid has been shown to have some effects on cognition in epileptics and normal controls,59 no significant effects on neuropsychological testing were seen in a double-blinded study of 279 persons with TBI who were given the medication for posttraumatic seizure prophylaxis.60 One of the benefits of valproic acid is the potential for a rapid load (10 –20 mg/kg/day). Its maximum dose is limited mainly by hepatotoxicity, thrombocytopenia, and medication toxicity. One study does suggest that persons with TBI may demonstrate increased metabolism of valproic acid, and thus this population may require higher doses.61 Another anticonvulsant used in the TBI population is carbamazepine, which although may cause some motor slowing, has effects of questionable clinical significance on cognitive tasks in one study.62 Chatham-Showalter63 described the successful use of carbamazepine in a series of seven acute inpatients with combativeness after TBI refractory to other medications. In another study, carbamazepine was found to significantly improve Agitated Behavior Scale scores without alteration of Mini-Mental Status Examination scores in eight of ten patients treated; particular areas of improvement cited were in irritability and disinhibition.64 Its major side effects include hyponatremia, renal failure, and in rare cases, aplastic anemia. Although dosing level is to therapeutic effect, serum levels should be monitored to avoid toxicity. Gabapentin has been reported to be helpful in modulating agitation related to dementia.65,66 However, a case series reported paradoxical effects in two persons with TBI treated with gabapentin for neuropathic pain.67 Other similar membrane-stabilizing agents, such as lamotrigine,68 may be of use in Agitation After Traumatic Brain Injury 801 802 Lombard and Zafonte Am. J. Phys. Med. Rehabil. ● Vol. 84, No. 10 Antidepressants Anticonvulsants Medication Class Paroxetine and citalopram Sertraline Lamotrigine Carbamazepine Valproic Acid Agent Case report Prospective open-label trial Single-blind placebo controlled Randomized placebo controlled Prospective controlled trial Pachet et al., 200368 Kant et al., 199881 Fann et al., 200077 Muller et al., 199978 Meythaler et al., 200179 Prospective, open label Randomized, case control Dikmen et al., 200060 Azouvi et al., 199964 Retrospective Chatham-Showalter et al., 200058 Case series Case report Monji et al., 199956 Chatham-Showalter, 199663 Case series Design Wroblewski et al., 199757 Study 7 patients with TBI and agitation in acute care 10 patients with TBI and significant anger outbursts A 40 yr old with severe TBI and aggression 13 persons with TBI and posttraumatic aggression and irritability 15 outpatients after TBI with severe depression 11 patients with DAI in acute inpatient rehabilitation 26 persons with TBI and pathological crying 29 persons with posttraumatic agitation in acute rehabilitation 279 persons with TBI 5 patients with TBIassociated aggression 16 yr old with history of TBI at 4 yrs old Sample Treatment with sertraline, amnesia and agitation scores Treatment with either paroxetine (n ⫽ 13) or citalopram (n ⫽ 13) Treatment with sertraline 8-wk trial of sertraline Treatment with carbamazepine, behavior testing Treatment with lamotrigine Seizure prophylaxis with valproic acid in half, neuropsychological testing Treatment with carbamazepine Valproic acid given for rapid-cycling affective disorder Treatment with valproic acid Treatment with valproic acid Intervention Outcome (Table continues) Both groups experienced improvements in symptoms No difference noted in cognition, alertness or agitation Decreased depression and aggression Decrease in aggressive behaviors, improved neurobehavioral functioning Reduced aggression and irritability, no effect on depression Good improvement seen in 5 cases, modest in 3, no response seen in 2 Reduced combativeness within 4 days of administration No significant differences in performance in neuropsychological tests 90% of sample responded with decreased agitation within 7 days Improved behavioral control Decreased aggression 1–2 days after initiation of the medication TABLE 2 Recent literature (after 1995) on the pharmacologic management of agitation in persons with traumatic brain injury (TBI) October 2005 Agitation After Traumatic Brain Injury 803 Perino et al., 200176 NA, not applicable. Multiple Database review Prospective Bellus et al., 1996125 Fleminger et al., 2003121 Case series Stanislav, 199795 Various Citalopram and carbamazepine Prospective Silver et al., 2003102 Risperidone Multiple medications Case report Maryniak et al., 200192 Methotrimeprazine NA Prospective intervention with retrospective comparison Case series Design Stanislav and Childs, 200091 Study Droperidol Agent Lithium Antipsychotics Medication Class TABLE 2 Continued 56 TBI inpatients with agitation in comparison with 64 TBI patients without agitation Adolescent patient with anoxic brain injury and significant motor restlessness Persons with TBI chronically on antipsychotic medications 2 persons with chronic aggressive behaviors in a state psychiatric facility 20 persons with TBI referred for treatment of depression and behavioral disturbance Evaluation of randomized, controlled trials performed 1980–2002 27 persons with TBI and significant agitation Sample NA Treatment with both agents, follow-up at 12 wks Treatment with lithium Administration of risperidone in addition to amantadine and methylphenidate Neuropsychological testing before and after taper off medications Treatment of agitation with methotrimeprazine Episodic agitation treated with intramuscular droperidol Intervention Beta-blockers have the best evidence for efficacy in the treatment of agitation in TBI patients Reduction in depression and behavioral disturbance Decreased aggression and need for behavioral control techniques Improvement in performance after discontinuation of antipsychotics Reduced restlessness, allowing for wound healing 2 cases of extrapyramidal symptoms, longer lengths of stay with treated group Time to calming shorter with droperidol in comparison with other medications Outcome TBI-related agitation; however, no studies beyond case reports have been reported. Antidepressant Agents Before the advent of selective-serotonin reuptake inhibitors (SSRIs), tricyclic antidepressants were the most commonly used medication in the pharmacological treatment of both idiopathic depression and mood disorders related to organic brain disease.69,70 In TBI, specifically, tricyclic antidepressants with predominantly noradrenergic action (e.g., protriptyline and desipramine) have shown some efficacy in the treatment of hypoarousal.71,72 Other tricyclic antidepressants that demonstrate greater affinity for serotonergic receptors (e.g., amitriptyline and imipramine) have a significant sedative side effect profile and thus have some potential to reduce aggression. An early case report described the successful treatment of a patient with frontal lobe damage and aggression with amitriptyline.73 It seems that the cause of the agitation may determine success with this medication; in a study by Mysiw et al.,74 12 out of 17 agitated persons with TBI in posttraumatic amnesia responded well to amitriptyline, whereas two of three patients out of posttraumatic amnesia failed to respond. Despite these successes, due to its sedative and cardiac effects and potential reduction of seizure threshold,75 its utility is limited in the TBI population. SSRIs offer the appeal of a more benign sideeffect profile than with tricyclic antidepressants. They have been shown to be efficacious in the treatment of depression in persons with TBI.76,77 An additional use for this class is in the treatment of emotional lability.78 Equivocal results were obtained in a small study of sertraline for hypoarousal in TBI patients.79 A case series of two patients with agitation associated with Huntington’s disease showed that sertraline was helpful in reducing irritability and aggressive behaviors.80 In 13 outpatients with TBI, treatment with sertraline for 8 wks reduced irritability and aggression, but it had no effect on depressive symptoms.81 One major drawback of this class is that, at least for its antidepressant effects, ⱖ2 wks is needed for effectiveness; this would be an unacceptable amount of time to wait for the control of severe agitation. Unlike the tricyclic agents, it seems that SSRIs may not have as significant of an effect on seizure frequency; in a study of 100 persons with epilepsy, five developed increased seizure frequency, but all returned to baseline with adjustments in seizure medications.82 A newer phenylpiperazine serotonergic agent commonly used for sleep-cycle regulation in TBI is trazodone. It has been shown in some studies to decrease agitation and aggressive behaviors in both 804 Lombard and Zafonte persons with dementia83,84 and progressive supranuclear palsy.85 However, a recent Cochrane Database Study questions its efficacy in elderly demented patients.86 Starting dose can be 50 –100 mg, with results of increased sleep usually seen by 150 mg. Care must be given when using this medication in those who are also taking SSRIs to avoid potential serotonin syndrome. Other side effects attributed to this medication include anticholinergic symptoms and priapism.87 Buspirone, as a serotonergic and weak dopaminergic agent, is known to have significant anxiolytic properties without sedation. Levine88 initially reported incidental findings of improvement in agitation in three persons with TBI who were given this medication; this has been supported in later studies.89,90 As buspirone may induce seizures, care should be taken in its use with persons with TBI. Antipsychotic Agents Typical antipsychotic agents have often been used for the immediate control of aggression or agitation in TBI patients; in the case of haloperidol, it can be given intravenously, intramuscularly, or orally, and it has a rapid onset of action. Intramuscular administration of droperidol, another member of the butyrophenone class, was found to be faster and superior in controlling acute episodes of agitation when compared with haloperidol, diphenhydramine, or lorazepam.91 Maryniak et al.92 describe their successful use of scheduled oral methotrimeprazine, from the older phenothiazine class of antipsychotics, in persons with TBI admitted to their inpatient rehabilitation unit; it had been used in almost half of their agitated inpatients (n ⫽ 56), with only two persons experiencing side effects of extrapyramidal symptoms and paradoxical akathisia. Although those treated with methotrimeprazine had longer periods of posttraumatic amnesia and lengths of stay, the authors assert that the patients with agitation as a group are typically more seriously injured than those without behavioral issues. There is, however, some concern with the use of typical antipsychotic agents in persons with TBI. Research by Feeney et al.93 showed that haloperidol slowed motor recovery in an animal model of TBI. In a study of humans, although haloperidol did not change eventual rehabilitation outcome, its use was associated with a longer period of time in posttraumatic amnesia.94 Improvements in neuropsychological test results were seen in a population of adults with TBI after a taper off chronic typical antipsychotic agents.95 As with any patient group, neuroleptic malignant syndrome has been reported in the administration of antipsychotic agents to persons with TBI;96 –98 presenting symptoms can Am. J. Phys. Med. Rehabil. ● Vol. 84, No. 10 include significant fever, leukocytosis, and muscle stiffness and can carry a mortality rate of ⬎10%.99 Treatment is with dantrolene and beta-blockers. Persons receiving these medications are also subject to extrapyramidal side effects of tardive dyskinesia and Parkinsonism, which could form lifelong sources of disability. The source of these adverse effects seems to be the typical antipsychotics’ particular affinity for blocking the D2 dopamine receptor; a newer generation of neuroleptics, termed atypical antipsychotics, has less D2 receptor activity and more 5HT-2a activity, theoretically reducing some of the undesirable effects and alpha adrenergic blockade. In an animal study evaluating the effects of antipsychotic agents on cognitive function after TBI, haloperidol was shown to increase Morris water maze time, whereas olanzapine did not.100 In an early study of the oldest atypical antipsychotic, clozapine, nine persons with TBI demonstrating rage and aggression were given this medication; three responded favorably and three had mild improvements in behavior, but two patients developed seizures.101 Frequent blood draws for evaluation of agranulocytosis are required for patients on clozapine. Risperidone, in combination with methylphenidate and amantadine, was shown to decrease restlessness in a 15-yr-old patient with anoxic brain injury.102 However, the powerful adrenergic and D2 blockade of this agent may raise concerns. In addition, a recent study in an animal model of TBI has suggested that at high doses, risperidone has a cognitive effect similar to haloperidol (A. Kline, personal communication, unpublished data, 2005). Benzodiazepines Benzodiazepines remain a core medication for sedation in the ICU and for surgical procedures. Short-acting agents (e.g., midazolam, lorazepam) and long-acting agents (e.g., diazepam, clonazepam) exist in both enteral and parenteral forms, allowing for a range of administrations. Shortacting benzodiazepines are commonly used in the treatment of acute mania and other psychiatric emergencies and, in one study, have been shown to be superior to haloperidol in the treatment of motor agitation in this population.103 Their utility in the treatment of acute alcohol withdrawal has been discussed earlier. In addition, benzodiazepines have been shown to be efficacious in the treatment of neuroleptic-induced akathisia.104,105 In brain injury, the effects of benzodiazepines are more complex. Early and daily administration of diazepam significantly impaired motor recovery in rats with cortical lesions; later administration in diazepam-naı̈ve injured rats produced a transient October 2005 reoccurrence of hemiparesis.106 In eight persons with a distant history of stroke, light sedation with midazolam resulted in reemergence of stroke symptoms.107 Benzodiazepines are thus considered by some to be in the group of potentially detrimental medications in persons with stroke108 and brain injury.109,110 Benzodiazepine administration may result in paradoxical agitation in a small subpopulation of patients, particularly in the elderly; it can be successfully treated with flumazneil.111,112 Elderly patients who take benzodiazepines regularly have lower functional status than those who do not.113 By its nature, this class of medications causes an amnestic effect and may increase confusion in those emerging from posttraumatic amnesia. It is not without any utility in this population; as an agent that potentiates the GABAA receptor, it also can be used as a treatment for spasticity. In addition, a case report by Caradoc-Davies114 suggested it has potential use in the treatment of mutism in persons with TBI. It is the authors’ opinion that, outside of their utility in the treatment of alcohol withdrawal, benzodiazepines should be used in emergency situations only and not be utilized in frequent dosing for the treatment of agitation. Beta-Blockers As a frequently used medication for the treatment of hyperadrenergic states after TBI, betablockers may also help in the reduction of agitation. Early studies suggest that atenolol can be helpful in the treatment of alcohol withdrawal, with reduction of agitation and anxiety and in more rapid normalization of vital signs.115 Beta-blockade has also been shown to be efficacious in managing akathisia due to either neuroleptic agents116 –118 or to Parkinson’s disease;116 lipophilic beta-blockers, such as propranolol and metoprolol, were particularly effective, suggesting a central mode of action.116,118 In persons with dementia, low-dose propranolol monotherapy was shown to decrease agitation, aggression, and wandering behaviors.119 Pindolol was reported to reduce violent behaviors in 8 of 13 inpatients with TBI in a double-blind, placebo-controlled trial, and in some, it reduced care needs due to improved behavioral management.120 A Cochrane database review of studies examining medications in the treatment of posttraumatic agitation found that beta-blockers had the best evidence for efficacy.121 The major limiting factor in the administration of beta-blockers is hypotension and bradycardia, but as many patients may present with aspects of hyperadrenergia, these medications may serve to treat two clinical problems at once. Agitation After Traumatic Brain Injury 805 Lithium Lithium carbonate has long been a mainstay treatment of mania and bipolar disease.122 Although specific details of its method of action are unknown, it is recognized to primarily alter sodium transport and increase intracellular metabolism of catecholamines. However lithium does seem to have some dopamine blocking effects, as it seems to inhibit the response to apomorphine in an animal model.123 Cohn et al.124 published one of the earliest reports of its use in persons with brain injury; they successfully treated a 12-yr-old boy who exhibited agitated and hypomanic behaviors with a 6-mo course of lithium. Two adults with brain injury–related aggression so severe they were admitted to a state psychiatric facility displayed reductions in frequency of outbursts and in other medication needs when placed on lithium.125 In the rehabilitation setting, a group of ten TBI patients with severe aggression were administered lithium; although five of these persons had significant improvement measured by improved participation in rehabilitation, three had significant side effects that required discontinuation.126 Silver et al.127 have suggested that lithium use in TBI be reserved for those whose aggression is related to manic effects and for those whose recurrent irritability is related to cyclic mood disorders. Lithium should be started at 300 mg twice a day and titrated by serum levels and side effects. Its toxicity level (⬎1.4 mEq/liter) is very close to its therapeutic range (0.6 –1.2 mEq/liter), and thus, levels should be closely monitored. Significant adverse reactions to lithium are often related to high serum levels and may include movement disorders, ranging from tremor to dystonia, seizures, hypothyroidism, bradycardia, and vomiting. Those with central nervous system dysfunction may be uniquely sensitive to lithium’s side effects;128 thus, the difficulties in managing this medication often detract from its potential utility in the treatment of agitated TBI patients. Neurostimulants Although it would seem that the administration of neurostimulant medications might be counterproductive in the management of agitated TBI patients, it seems that they do have a role. In humans, dopaminergic agents, such as amantadine and bromocriptine, have been shown to be efficacious in the treatment of low-level states129,130 and in increasing the rate of both motoric and cognitive recovery.131,132 Bromocriptine has been suggested as a treatment of TBI-induced akathisia in two case reports;133,134 however, it may cause movement disorders as a side effect. In an early study, amantadine was shown to reduce agitation in 7 of 19 persons with dementia. However, adverse 806 Lombard and Zafonte effects of overactivity, anxiety, and visual hallucinations were seen in eight of the test subjects.135 Studies performed on the brain injury population have demonstrated its utility in the treatment of severe impairments of consciousness129,136,137 and in the enhancement of higher-level cognitive function.131,138,139 Amantadine’s utility as a mood-stabilizing agent was shown in several small case series in persons with agitation due to TBI.137,140,141 Because of this potential to both enhance recovery and control undesirable behaviors, it has been identified by experts in brain injury rehabilitation as a preferred agent for the treatment of agitation.26 Methylphenidate has been shown to help with concentration and processing deficits after TBI.142,143 In one randomized, placebo-controlled study of 38 persons with chronic TBI-related anger, 30 mg daily of methylphenidate significantly reduced these behaviors.144 Other Agents and Modalities There are a number of promising treatment avenues that merit further study. As stated above, there is a paucity of literature examining the potential benefits of newer anticonvulsant agents, such as lamotrigine and levetiracetam. As a combination SSRI and norepinephrine reuptake inhibitor, duloxetine may also have benefits as both a neurostimulant and a mood-stabilizing agent. A 1995 case report described the successful treatment of severe agitation unresponsive to pharmacologic measures with electroconvulsive therapy. A course of six brief-pulse treatments resulted in improved participation in self-care skills and response to medication.145 Although this treatment certainly should not be first-line management, further studies to investigate its potential use in intractable posttraumatic agitation are in order. An additional treatment that has demonstrated promise in other arenas is magnesium. It has been shown as an effective treatment for mania in persons with bipolar disorder.146 –148 It may have benefits beyond behavioral management; magnesium has been shown to have neuroprotective properties in acute TBI. Three studies in rats showed improved behavioral149 and motoric150,151 recovery when magnesium was administered acutely after injury. A potential mechanism was suggested by Ustun et al.;152 magnesium reduced the typical decline of the antioxidants superoxide dismutase and glutathione peroxidase in a model of brain injury in rabbits. Alternative medications also remain under-examined treatments in persons with TBI. Lavender oil as aromatherapy has been suggested as an agent to reduce anxiety and agitation. In one study of normal subjects in a randomized, controlled deAm. J. Phys. Med. Rehabil. ● Vol. 84, No. 10 sign, lavender oil added to bath water reduced anger and frustration levels.153 In persons with agitation related to dementia, the literature examining lavender has been equivocal; although one study found modestly positive results,154 two others found no improvement in behavior.155,156 APPROACH TO AGITATION ICU As we have now introduced the substantial array of medications investigated in the treatment of agitation in persons with TBI, we suggest a systematic approach to the problem. The patient’s general treatment goals and location often dictate initial management. With a person in the ICU setting who may have unstable fractures, endotracheal intubation, and increased intracranial pressure, use of significantly sedating medications such as the lipid-soluble agent propofol are indicated (Fig. 1). Agents that address the person’s pain are also of importance during this time frame. Shortacting benzodiazepines may be needed to accomplish required testing once more generally sedating agents have been weaned. As the patient becomes more stable, and the treatment goals move toward increased mobility and participation in therapies, behavioral management is necessary. We advocate for an early approach to the patient who may need longer-term therapy for his or her agitation, thus beginning potential evaluations and treatment regimens as previously described. Systematic Evaluation in the Post-ICU and Rehabilitation Setting The assessment of an agitated patient starts with an evaluation of the safety of the patient and staff members. Those persons who pose a significant and immediate risk of harm to themselves or FIGURE 1 Agitation management flow sheet. ABS, Agitated Behavior Scale; SSRI, selective-serotonin reuptake inhibitor. October 2005 Agitation After Traumatic Brain Injury 807 others and who cannot be redirected will need to be managed with rapidly acting pharmacologic agents, such as lorazepam. If there is no urgent safety issue, some consideration can be given to the possible differential diagnosis of the behavioral disturbance. A detailed patient history should be performed, with special attention to drug and alcohol use and psychiatric conditions. Vital signs, laboratory values, electroencephalograms, and radiologic evaluation should be performed as appropriate. The importance of reducing sensory stimulation in an acutely agitated patient cannot be overemphasized; excess staff members should be excused from the nearby area, television sets should be turned off, and lighting should be dimmed as possible. Evaluation of sleep-cycle regulation should be given careful consideration; in our acute inpatient TBI unit, the nursing staff records the number of hours slept for all patients. If the sleep cycle is disrupted, and environmental interventions (such as reducing caffeine intake and minimizing naps during the day) are ineffective, trazodone should be considered. Adequate pain medication should be given as appropriate. Treatment in the Post-ICU and Rehabilitation Setting In the absence of response to behavioral and environmental modification, pharmacology for the management of agitation may be considered. The class of medication initially selected partially depends on potential secondary benefits. If the patient is also experiencing hyperadrenergia, betablockers are likely to be a good choice. Persons with deficits in attention and concentration may benefit from amantadine. Anticonvulsants, particularly carbamazepine and valproic acid, are effective for severe agitation. Other agents, such as atypical antipsychotics and SSRIs also may be considered, particularly if the patient has additional psychiatric co-morbidities. Frequent use of “emergency” medications is an indication of poor general control of agitation. Lastly, it is important to use objective measures, such as the Agitated Behavior Scale, to monitor success of treatment. CONCLUSIONS This review represents the thoughts of the authors based on their experiences and review of the literature. Additional research is certainly needed to elucidate many aspects of agitation after TBI. The pathophysiology of agitation in both an anatomic and a neurochemical basis remains largely a mystery. Likewise, more investigation into the safety of atypical antipsychotic agents needs to be pursued, starting with further animal studies. As mentioned above, several other medications, such as newer antiepileptics and antidepres- 808 Lombard and Zafonte sant therapies, show some initial promise for the treatment of agitation. There is a general paucity of randomized, controlled clinical trials even for the most commonly used medications. Finally, the validity and applicability of human studies depend on a common language describing agitation and common objective measurement tools. The importance of effective management of persons with agitation after TBI has the potential to reduce morbidity and staffing needs and to improve safety, participation in rehabilitation, and overall function. REFERENCES 1. Gouvier WD, Blanton PD, LaPorte KK, et al: Reliability and validity of the Disability Rating Scale and the Levels of Cognitive Functioning Scale in monitoring recovery from severe head injury. Arch Phys Med Rehabil 1987;68:94–7 2. Corrigan JD, Mysiw WJ: Agitation following traumatic head injury: Equivocal evidence for a discrete stage of cognitive recovery. Arch Phys Med Rehabil 1988;69: 487–92 3. Galski T, Palasz J, Bruno RL, et al: Predicting physical and verbal aggression on a brain trauma unit. Arch Phys Med Rehabil 1994;75:380–3 4. Brooke MM, Questad KA, Patterson DR, et al: Agitation and restlessness after closed head injury: A prospective study of 100 consecutive admissions. Arch Phys Med Rehabil 1992;73:320–3 5. Kadyan V, Mysiw WJ, Bogner JA, et al: Gender differences in agitation after traumatic brain injury. Am J Phys Med Rehabil 2004;83:747–52 6. Fugate LP, Spacek LA, Kresty LA, et al: Definition of agitation following traumatic brain injury: I. A survey of the Brain Injury Special Interest Group of the American Academy of Physical Medicine and Rehabilitation. Arch Phys Med Rehabil 1997;78:917–23 7. Corrigan JD: Development of a scale for assessment of agitation following traumatic brain injury. J Clin Exp Neuropsychol 1989;11:261–77 8. Sachdev P: The development of the concept of akathisia: A historical overview. Schizophr Res 1995;16:33–45 9. Miller CH, Fleischhacker WW: Managing antipsychoticinduced acute and chronic akathisia. Drug Saf 2000;22: 73–81 10. Albert DJ, Chew GL: The septal forebrain and the inhibitory modulation of attack and defense in the rat: A review. Behav Neural Biol 1980;30:357–88 11. Siegel A, Schubert KL, Shaikh MB: Neurotransmitters regulating defensive rage behavior in the cat. Neurosci Biobehav Rev 1997;21:733–42 12. Martinius J: Homicide of an aggressive adolescent boy with right temporal lesion: A case report. Neurosci Biobehav Rev 1983;7:419–22 13. van Elst LT, Woermann FG, Lemieux L, et al: Affective aggression in patients with temporal lobe epilepsy: A quantitative MRI study of the amygdala. Brain 2000;123(pt 2):234–43 14. Vespa PM, Nuwer MR, Nenov V, et al: Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring. J Neurosurg 1999;91: 750–60 15. van Erp AM, Miczek KA: Aggressive behavior, increased accumbal dopamine, and decreased cortical serotonin in rats. J Neurosci 2000;20:9320–5 16. Bouwknecht JA, Hijzen TH, van der Gugten, J, et al: Absence of 5-HT(1B) receptors is associated with impaired Am. J. Phys. Med. Rehabil. ● Vol. 84, No. 10 impulse control in male 5-HT(1B) knockout mice. Biol Psychiatry 2001;49:557–68 delirium in the surgical intensive care unit. Crit Care 2001;5:265–70 17. Nikulina EM, Kapralova NS: Role of dopamine receptors in the regulation of aggression in mice: Relationship to genotype. Neurosci Behav Physiol 1992;22:364–9 38. Atchison JW, Wachendorf J, Haddock D, et al: Hyponatremia-associated cognitive impairment in traumatic brain injury. Brain Inj 1993;7:347–52 18. Linnoila M, Virkkunen M, Scheinin M, et al: Low cerebrospinal fluid 5-hydroxyindoleacetic acid concentration differentiates impulsive from nonimpulsive violent behavior. Life Sci 1983;33:2609–14 39. Kahn DM, Cook TE, Carlisle CC, et al: Identification and modification of environmental noise in an ICU setting. Chest 1998;114:535–40 19. Chiavegatto S, Nelson RJ: Interaction of nitric oxide and serotonin in aggressive behavior. Horm Behav 2003;44: 233–41 20. Spielewoy C, Roubert C, Hamon M, et al: Behavioural disturbances associated with hyperdopaminergia in dopamine-transporter knockout mice. Behav Pharmacol 2000;11:279–90 21. Farde L: Selective D1- and D2-dopamine receptor blockade both induces akathisia in humans: A PET study with [11C]SCH 23390 and [11C]raclopride. Psychopharmacology (Berl) 1992;107:23–9 22. Bogner JA, Corrigan JD, Stange M, et al: Reliability of the Agitated Behavior Scale. J Head Trauma Rehabil 1999;14: 91–6 23. Yudofsky SC, Silver JM, Jackson W, et al: The Overt Aggression Scale for the objective rating of verbal and physical aggression. Am J Psychiatry 1986;143:35–9 24. Alderman N, Knight C, Morgan C: Use of a modified version of the Overt Aggression Scale in the measurement and assessment of aggressive behaviours following brain injury. Brain Inj 1997;11:503–23 25. Alderman N, Davies JA, Jones C, et al: Reduction of severe aggressive behaviour in acquired brain injury: Case studies illustrating clinical use of the OAS-MNR in the management of challenging behaviours. Brain Inj 1999;13:669– 704 26. Fugate LP, Spacek LA, Kresty LA, et al: Measurement and treatment of agitation following traumatic brain injury: II. A survey of the Brain Injury Special Interest Group of the American Academy of Physical Medicine and Rehabilitation. Arch Phys Med Rehabil 1997;78:924–8 27. Angelino E, Miglioretti M, Zotti AM: Agitation assessment in severe traumatic brain injury: Methodological and clinical issues. Brain Inj 2002;16:269–75 28. Alderman N, Knight C, Henman C: Aggressive behaviour observed within a neurobehavioural rehabilitation service: Utility of the OAS-MNR in clinical audit and applied research. Brain Inj 2002;16:469–89 29. Bayard M, McIntyre J, Hill KR, et al: Alcohol withdrawal syndrome. Am Fam Physician Mar 15, 2004;69(6):1443–50 30. Olmedo R, Hoffman RS: Withdrawal syndromes. Emerg Med Clin North Am 2000;18:273–88 31. Dimopoulou I, Tsagarakis S, Theodorakopoulou M, et al: Endocrine abnormalities in critical care patients with moderate-to-severe head trauma: Incidence, pattern and predisposing factors. Intensive Care Med 2004;30:1051–7 32. Burger AG, Philippe J: Thyroid emergencies. Baillieres Clin Endocrinol Metab 1992;6:77–93 33. Demet MM, Ozmen B, Deveci A, et al: Depression and anxiety in hyperthyroidism. Arch Med Res 2002;33:552–6 34. Tenedieva VD, Potapov AA, Gaitur EI, et al: Thyroid hormones in comatose patients with traumatic brain injury. Acta Neurochir Suppl 2000;76:385–91 35. Agha A, Rogers B, Mylotte D, et al: Neuroendocrine dysfunction in the acute phase of traumatic brain injury. Clin Endocrinol (Oxf) 2004;60:584–91 36. Webster JB, Bell KR: Primary adrenal insufficiency following traumatic brain injury: A case report and review of the literature. Arch Phys Med Rehabil 1997;78:314–8 37. Aldemir M, Ozen S, Kara IH, et al: Predisposing factors for October 2005 40. Granberg Axell AI, Malmros CW, Bergbom IL, et al: Intensive care unit syndrome/delirium is associated with anemia, drug therapy and duration of ventilation treatment. Acta Anaesthesiol Scand 2002;46:726–31 41. Food and Drug Administration announcement. March 25, 2005 42. Zafonte RD, Hammond FD, Rahimi R: Air embolism in the agitated traumatic brain injury patient: An unusual complication. Brain Inj 1996;10:759–61 43. Engst C, Chhokar R, Robinson D, et al: Implementation of a scheduled toileting program in a long term care facility: Evaluating the impact on injury risk to caregiving staff. AAOHN J 2004;52:427–35 44. Clinchot DM, Bogner J, Mysiw WJ, et al: Defining sleep disturbance after brain injury. Am J Phys Med Rehabil 1998;77:291–5 45. Castriotta RJ, Lai JM: Sleep disorders associated with traumatic brain injury. Arch Phys Med Rehabil 2001;82: 1403–6 46. Webster JB, Bell KR, Hussey JD, et al: Sleep apnea in adults with traumatic brain injury: A preliminary investigation. Arch Phys Med Rehabil 2001;82:316–21 47. Buffum MD, Miaskowski C, Sands L, et al: A pilot study of the relationship between discomfort and agitation in patients with dementia. Geriatr Nurs 2001;22:80–5 48. Zieber CG, Hagen B, Armstrong-Esther C, et al: Pain and agitation in long-term care residents with dementia: Use of the Pittsburgh Agitation Scale. Int J Palliat Nurs 2005;11: 71–8 49. Irving MH, Irving PM: Associated injuries in head injured patients. J Trauma 1967;7:500–11 50. Prigatano GP, Borgaro S, Caples H: Non-pharmacological management of psychiatric disturbances after traumatic brain injury. Int Rev Psychiatry 2003;15:371–9 51. Bowden CL: Valproate. Bipolar Disord 2003;5:189–202 52. Narayan M, Nelson JC: Treatment of dementia with behavioral disturbance using divalproex or a combination of divalproex and a neuroleptic. J Clin Psychiatry 1997;58: 351–4 53. Porsteinsson AP, Tariot PN, Erb R, et al: Placebo-controlled study of divalproex sodium for agitation in dementia. Am J Geriatr Psychiatry 2001;9:58–66 54. Porsteinsson AP, Tariot PN, Jakimovich LJ, et al: Valproate therapy for agitation in dementia: Open-label extension of a double-blind trial. Am J Geriatr Psychiatry 2003;11: 434–40 55. Lonergan ET, Cameron M, Luxenberg J: Valproic acid for agitation in dementia. Cochrane Database Syst Rev 2004; 2:CD003945 56. Monji A, Yoshida I, Koga H, et al: Brain injury-induced rapid-cycling affective disorder successfully treated with valproate. Psychosomatics. 1999;40:448–9 57. Wroblewski BA, Joseph AB, Kupfer J, et al: Effectiveness of valproic acid on destructive and aggressive behaviours in patients with acquired brain injury. Brain Inj 1997;11: 37–47 58. Chatham-Showalter PE, Kimmel DN: Agitated symptom response to divalproex following acute brain injury. J Neuropsychiatry Clin Neurosci 2000;12:395–7 59. Massagli TL: Neurobehavioral effects of phenytoin, carbamazepine, and valproic acid: Implications for use in Agitation After Traumatic Brain Injury 809 traumatic brain injury. Arch Phys Med Rehabil 1991;72: 219–26 treatment of severe aggressiveness in Huntington’s disease. J Neuropsychiatry Clin Neurosci 1996;8:338–40 60. Dikmen SS, Machamer JE, Winn HR, et al: Neuropsychological effects of valproate in traumatic brain injury: A randomized trial. Neurology 2000;54:895–902 81. Kant R, Smith-Seemiller L, Zeiler D: Treatment of aggression and irritability after head injury. Brain Inj 1998;12: 661–6 61. Anderson GD, Awan AB, Adams CA, et al: Increases in metabolism of valproate and excretion of 6beta-hydroxycortisol in patients with traumatic brain injury. Br J Clin Pharmacol 1998;45:101–5 82. Kanner AM, Kozak AM, Frey M: The use of sertraline in patients with epilepsy: Is it safe? Epilepsy Behav 2000;1: 100–5 62. Smith KR Jr, Goulding PM, Wilderman D, et al: Neurobehavioral effects of phenytoin and carbamazepine in patients recovering from brain trauma: A comparative study. Arch Neurol 1994;51:653–60 63. Chatham-Showalter PE: Carbamazepine for combativeness in acute traumatic brain injury. J Neuropsychiatry Clin Neurosci 1996;8:96–9 64. Azouvi P, Jokic C, Attal N, et al: Carbamazepine in agitation and aggressive behaviour following severe closedhead injury: Results of an open trial. Brain Inj 1999;13: 797–804 65. Herrmann N, Lanctot K, Myszak M: Effectiveness of gabapentin for the treatment of behavioral disorders in dementia. J Clin Psychopharmacol 2000;20:90–3 66. Roane DM, Feinberg TE, Meckler L, et al: Treatment of dementia-associated agitation with gabapentin. J Neuropsychiatry Clin Neurosci 2000;12:40–3 67. Childers MK, Holland D: Psychomotor agitation following gabapentin use in brain injury. Brain Inj 1997;11:537–40 68. Pachet A, Friesen S, Winkelaar D, et al: Beneficial behavioural effects of lamotrigine in traumatic brain injury. Brain Inj 2003;17:715–22 84. Sultzer DL, Gray KF, Gunay I, et al: A double-blind comparison of trazodone and haloperidol for treatment of agitation in patients with dementia. Am J Geriatr Psychiatry 1997;5:60–9 85. Schneider LS, Gleason RP, Chui HC: Progressive supranuclear palsy with agitation: Response to trazodone but not to thiothixine or carbamazepine. J Geriatr Psychiatry Neurol 1989;2:109–12 86. Martinon-Torres G, Fioravanti M, Grimley EJ: Trazodone for agitation in dementia. Cochrane Database Syst Rev 2004;4:CD004990 87. Saenz de Tejada I, Ware JC, Blanco R, et al: Pathophysiology of prolonged penile erection associated with trazodone use. J Urol 1991;145:60–4 88. Levine AM: Buspirone and agitation in head injury. Brain Inj 1988;2:165–7 89. Gualtieri CT: Buspirone for the behavior problems of patients with organic brain disorders. J Clin Psychopharmacol 1991;11:280–1 69. Lipsey JR, Robinson RG, Pearlson GD, et al: Nortriptyline treatment of post-stroke depression: A double-blind study. Lancet 1984;1:297–300 90. Ratey JJ, Leveroni CL, Miller AC, et al: Low-dose buspirone to treat agitation and maladaptive behavior in brain-injured patients: Two case reports. J Clin Psychopharmacol 1992;12:362–4 70. Wroblewski BA, Joseph AB, Cornblatt RR: Antidepressant pharmacotherapy and the treatment of depression in patients with severe traumatic brain injury: A controlled, prospective study. J Clin Psychiatry 1996;57:582–7 91. Stanislav SW, Childs A: Evaluating the usage of droperidol in acutely agitated persons with brain injury. Brain Inj 2000;14:261–5 71. Wroblewski B, Glenn MB, Cornblatt R, et al: Protriptyline as an alternative stimulant medication in patients with brain injury: A series of case reports. Brain Inj 1993;7: 353–62 72. Reinhard DL, Whyte J, Sandel ME: Improved arousal and initiation following tricyclic antidepressant use in severe brain injury. Arch Phys Med Rehabil 1996;77:80–3 73. Jackson RD, Corrigan JD, Arnett JA: Amitriptyline for agitation in head injury. Arch Phys Med Rehabil 1985;66: 180–1 74. Mysiw WJ, Jackson RD, Corrigan JD: Amitriptyline for post-traumatic agitation. Am J Phys Med Rehabil 1988;67: 29–33 75. Wroblewski BA, McColgan K, Smith K, et al: The incidence of seizures during tricyclic antidepressant drug treatment in a brain-injured population. J Clin Psychopharmacol 1990;10:124–8 76. Perino C, Rago R, Cicolini A, et al: Mood and behavioural disorders following traumatic brain injury: Clinical evaluation and pharmacological management. Brain Inj 2001; 15:139–48 77. Fann JR, Uomoto JM, Katon WJ: Sertraline in the treatment of major depression following mild traumatic brain injury. J Neuropsychiatry Clin Neurosci 2000;12:226–32 78. Muller U, Murai T, Bauer-Wittmund T, et al: Paroxetine versus citalopram treatment of pathological crying after brain injury. Brain Inj 1999;13:805–11 79. Meythaler JM, Depalma L, Devivo MJ, et al: Sertraline to improve arousal and alertness in severe traumatic brain injury secondary to motor vehicle crashes. Brain Inj 2001; 15:321–31 80. Ranen NG, Lipsey JR, Treisman G, et al: Sertraline in the 810 83. Lebert F, Stekke W, Hasenbroekx C, et al: Frontotemporal dementia: A randomised, controlled trial with trazodone. Dement Geriatr Cogn Disord 2004;17:355–9 Lombard and Zafonte 92. Maryniak O, Manchanda R, Velani A: Methotrimeprazine in the treatment of agitation in acquired brain injury patients. Brain Inj 2001;15:167–74 93. Feeney DM, Gonzalez A, Law WA: Amphetamine, haloperidol, and experience interact to affect rate of recovery after motor cortex injury. Science 1982;217:855–7 94. Rao N, Jellinek HM, Woolston DC: Agitation in closed head injury: Haloperidol effects on rehabilitation outcome. Arch Phys Med Rehabil 1985;66:30–4 95. Stanislav SW: Cognitive effects of antipsychotic agents in persons with traumatic brain injury. Brain Inj 1997;11: 335–41 96. Kadyan V, Colachis SC, Depalma MJ, et al: Early recognition of neuroleptic malignant syndrome during traumatic brain injury rehabilitation. Brain Inj 2003;17:631–7 97. Vincent FM, Zimmerman JE, Van Haren, J: Neuroleptic malignant syndrome complicating closed head injury. Neurosurgery 1986;18:190–3 98. Wilkinson R, Meythaler JM, Guin-Renfroe S: Neuroleptic malignant syndrome induced by haloperidol following traumatic brain injury. Brain Inj 1999;13:1025–31 99. Persing JS: Neuroleptic malignant syndrome: An overview. S D J Med 1994;47:51–5 100. Wilson MS, Gibson CJ, Hamm RJ: Haloperidol, but not olanzapine, impairs cognitive performance after traumatic brain injury in rats. Am J Phys Med Rehabil 2003;82:871–9 101. Michals ML, Crismon ML, Roberts S, et al: Clozapine response and adverse effects in nine brain-injured patients. J Clin Psychopharmacol 1993;13:198–203 102. Silver BV, Collins L, Zidek KA: Risperidone treatment of motor restlessness following anoxic brain injury. Brain Inj 2003;17:237–44 Am. J. Phys. Med. Rehabil. ● Vol. 84, No. 10 103. Wyant M, Diamond BI, O’Neal, E, et al: The use of midazolam in acutely agitated psychiatric patients. Psychopharmacol Bull 1990;26:126–9 104. Hirose S, Ashby CR: Immediate effect of intravenous diazepam in neuroleptic-induced acute akathisia: An openlabel study. J Clin Psychiatry 2002;63:524–7 105. Bartels M, Heide K, Mann K, et al: Treatment of akathisia with lorazepam: An open clinical trial. Pharmacopsychiatry 1987;20:51–3 106. Schallert T, Hernandez TD, Barth TM: Recovery of function after brain damage: Severe and chronic disruption by diazepam. Brain Res 1986;379:104–11 107. Lazar RM, Fitzsimmons BF, Marshall RS, et al: Reemergence of stroke deficits with midazolam challenge. Stroke 2002;33:283–5 108. Goldstein LB: Common drugs may influence motor recovery after stroke: The Sygen In Acute Stroke Study Investigators. Neurology 1995;45:865–71 109. Goldstein LB: Prescribing of potentially harmful drugs to patients admitted to hospital after head injury. J Neurol Neurosurg Psychiatry 1995;58:753–5 110. Goldstein LB: Basic and clinical studies of pharmacologic effects on recovery from brain injury. J Neural Transplant Plast 1993;4:175–92 111. Rodrigo CR: Flumazenil reverses paradoxical reaction with midazolam. Anesth Prog 1991;38:65–8 112. Weinbroum AA, Szold O, Ogorek D, et al: The midazolaminduced paradox phenomenon is reversible by flumazenil: Epidemiology, patient characteristics and review of the literature. Eur J Anaesthesiol 2001;18:789–97 113. Ried LD, Johnson RE, Gettman DA: Benzodiazepine exposure and functional status in older people. J Am Geriatr Soc 1998;46:71–6 114. Caradoc-Davies TH: Traumatic mutism in severe head injury relieved by oral diazepam. Disabil Rehabil 1996;18: 482–4 115. Gottlieb LD: The role of beta blockers in alcohol withdrawal syndrome. Postgrad Med 1988;Spec No:169–74 116. Adler LA, Angrist B, Weinreb H, et al: Studies on the time course and efficacy of beta-blockers in neuroleptic-induced akathisia and the akathisia of idiopathic Parkinson’s disease. Psychopharmacol Bull 1991;27:107–11 117. Dumon JP, Catteau J, Lanvin F, et al: Randomized, doubleblind, crossover, placebo-controlled comparison of propranolol and betaxolol in the treatment of neurolepticinduced akathisia. Am J Psychiatry 1992;149:647–50 drome in an adolescent treated with lithium carbonate: Case report. Dis Nerv Syst 1977;38:630–1 125. Bellus SB, Stewart D, Vergo JG, et al: The use of lithium in the treatment of aggressive behaviours with two braininjured individuals in a state psychiatric hospital. Brain Inj 1996;10:849–60 126. Glenn MB, Wroblewski B, Parziale J, et al: Lithium carbonate for aggressive behavior or affective instability in ten brain-injured patients. Am J Phys Med Rehabil 1989; 68:221–6 127. Silver J, Youdofsky S, Anderson K : Textbook of Traumatic Brain Injury. Washington, DC, American Psychiatric Publishing, 2005 128. Moskowitz A, Altshuler L: Increased sensitivity to lithiuminduced neurotoxicity after stroke: A case report. J Clin Psychopharmacol 1991;11;272–3 129. Zafonte RD, Watanabe T, Mann NR: Amantadine: A potential treatment for the minimally conscious state. Brain Inj 1998;12:617–21 130. Passler MA, Riggs RV: Positive outcomes in traumatic brain injury-vegetative state: Patients treated with bromocriptine. Arch Phys Med Rehabil 2001;82:311–5 131. Meythaler JM, Brunner RC, Johnson A, et al: Amantadine to improve neurorecovery in traumatic brain injury-associated diffuse axonal injury: A pilot double-blind randomized trial. J Head Trauma Rehabil 2002;17:300–13 132. Powell JH, al-Adawi, S, Morgan J, et al: Motivational deficits after brain injury: Effects of bromocriptine in 11 patients. J Neurol Neurosurg Psychiatry 1996;60:416–21 133. Stewart JT: Akathisia following traumatic brain injury: Treatment with bromocriptine. J Neurol Neurosurg Psychiatry 1989;52:1200–1 134. Silver BV, Yablon SA: Akathisia resulting from traumatic brain injury. Brain Inj 1996;10:609–14 135. Muller HF, Dastoor DP, Klingner A, et al: Amantadine in senile dementia: Electroencephalographic and clinical effects. J Am Geriatr Soc 1979;27:9–16 136. Edby K, Larsson J, Eek M, et al: Amantadine treatment of a patient with anoxic brain injury. Childs Nerv Syst 1995; 11:607–9 137. Rosati DL: Early polyneuropharmacologic intervention in brain injury agitation. Am J Phys Med Rehabil 2002;81: 90–3 138. Arciniegas DB, Frey KL, Anderson CA, et al: Amantadine for neurobehavioural deficits following delayed post-hypoxic encephalopathy. Brain Inj 2004;18:1309–18 118. Zubenko GS, Lipinski JF, Cohen BM, et al: Comparison of metoprolol and propranolol in the treatment of akathisia. Psychiatry Res 1984;11:143–9 139. Wu TS, Garmel GM: Improved neurological function after Amantadine treatment in two patients with brain injury. J Emerg Med 2005;28:289–92 119. Shankle WR, Nielson KA, Cotman CW: Low-dose propranolol reduces aggression and agitation resembling that associated with orbitofrontal dysfunction in elderly demented patients. Alzheimer Dis Assoc Disord 1995;9: 233–7 140. Chandler MC, Barnhill JL, Gualtieri CT: Amantadine for the agitated head-injury patient. Brain Inj 1988;2:309–11 120. Greendyke RM, Berkner JP, Webster JC, et al: Treatment of behavioral problems with pindolol. Psychosomatics 1989; 30:161–5 142. Whyte J, Hart T, Schuster K, et al: Effects of methylphenidate on attentional function after traumatic brain injury: A randomized, placebo-controlled trial. Am J Phys Med Rehabil 1997;76:440–50 121. Fleminger S, Greenwood RJ, Oliver DL: Pharmacological management for agitation and aggression in people with acquired brain injury. Cochrane Database Syst Rev 2003; 1:CD003299 141. Nickels JL, Schneider WN, Dombovy ML, et al: Clinical use of amantadine in brain injury rehabilitation. Brain Inj 1994;8:709–18 143. Whyte J, Hart T, Vaccaro M, et al: Effects of methylphenidate on attention deficits after traumatic brain injury: A multidimensional, randomized, controlled trial. Am J Phys Med Rehabil 2004;83:401–20 122. Geddes JR, Burgess S, Hawton K, et al: Long-term lithium therapy for bipolar disorder: Systematic review and metaanalysis of randomized controlled trials. Am J Psychiatry 2004;161:217–22 144. Mooney GF, Haas LJ: Effect of methylphenidate on brain injury-related anger. Arch Phys Med Rehabil 1993;74: 153–60 123. Fazli-Tabaei S, Yahyavi SH, Zarrindast MR: Effects of lithium carbonate on apomorphine-induced sniffing behaviour in rats. Pharmacol Toxicol 2002;91:135–9 145. Kant R, Bogyi AM, Carosella NW, et al: ECT as a therapeutic option in severe brain injury. Convuls Ther 1995; 11:45–50 124. Cohn CK, Wright JR, DeVaul RA: Post head trauma syn- 146. Heiden A, Frey R, Presslich O, et al: Treatment of severe October 2005 Agitation After Traumatic Brain Injury 811 147. 148. 149. 150. 151. 812 mania with intravenous magnesium sulphate as a supplementary therapy. Psychiatry Res 1999;89:239–46 Chouinard G, Beauclair L, Geiser R, et al: A pilot study of magnesium aspartate hydrochloride (Magnesiocard) as a mood stabilizer for rapid cycling bipolar affective disorder patients. Prog Neuropsychopharmacol Biol Psychiatry 1990;14:171–80 Giannini AJ, Nakoneczie AM, Melemis SM, et al: Magnesium oxide augmentation of verapamil maintenance therapy in mania. Psychiatry Res 2000;93:83–7 Hoane MR, Barth TM: The behavioral and anatomical effects of MgCl2 therapy in an electrolytic lesion model of cortical injury in the rat. Magnes Res. 2001;14:51–63 Heath DL, Vink R: Magnesium sulphate improves neurologic outcome following severe closed head injury in rats. Neurosci Lett 1997;228:175–8 Vink R, O’Connor, CA, Nimmo AJ, et al: Magnesium attenuates persistent functional deficits following diffuse traumatic brain injury in rats. Neurosci Lett 2003;336: 41–4 Lombard and Zafonte 152. Ustun ME, Duman A, Ogun CO, et al: Effects of nimodipine and magnesium sulfate on endogenous antioxidant levels in brain tissue after experimental head trauma. J Neurosurg Anesthesiol 2001;13:227–32 153. Morris N: The effects of lavender (Lavendula angustifolium) baths on psychological well-being: Two exploratory randomised control trials. Complement Ther Med 2002; 10:223–8 154. Holmes C, Hopkins V, Hensford C, et al: Lavender oil as a treatment for agitated behaviour in severe dementia: A placebo controlled study. Int J Geriatr Psychiatry 2002; 17:305–8 155. Gray SG, Clair AA: Influence of aromatherapy on medication administration to residential-care residents with dementia and behavioral challenges. Am J Alzheimers Dis Other Demen 2002;17:169–74 156. Snow LA, Hovanec L, Brandt J: A controlled trial of aromatherapy for agitation in nursing home patients with dementia. J Altern Complement Med 2004;10:431–7 Am. J. Phys. Med. Rehabil. ● Vol. 84, No. 10