Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
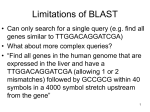
Practical guide: Medical Imaging Concepts Clinical and workflow Steven Horii, MD, FACR, FSIIM Professor of Radiology, Clinical Director , Medical Informatics Group Modality Chief, Ultrasound Hospital of the University of Pennsylvania Attending Radiologist, Children’s Hospital of Philadelphia Disclosures • My wife is a full-time employee of Cerner Corporation • Site PI, Phase III clinical trial, ultrasound contrast for liver masses, Bracco Pharmaceuticals, Inc. • Expert witness, Blakely Sokoloff Taylor & Zafman, LLP (Patent litigation) Introduction • A tiny bit about clinical stuff • The unavoidability of workflow • The complexity of workflow and multiplication of that through interacting (or colliding) workflows • The changing healthcare model • What that means for you Clinical • What we do • What do you mean “we”, kemosabe? • OK, then – what do physicians in general do; with some radiology particulars Workflow • How we do it • In twenty minutes? • OK, then – – Why workflow can seem simple – Why it generally is not – Why is workflow important? Clinical: An overview • Physicians: – Given a story or complaint by a patient, – Try to figure out what, if anything, is wrong – Figure out a treatment plan – Treat the patient – If the patient is not improving, return to bullet item 2 – Oh yeah, get paid Clinical: An overview See patient Figure out what is wrong No Treat patient Getting better? Yes Submit bill Next Notice anything? • From a description of what we do, a flow diagram (of sorts) comes out • It is difficult to separate what we do from how we do it What do radiologists do? • Image humans (and animals) to: – Diagnose diseases or anomalies – Guide and perform procedures – Help develop treatment plans – Evaluate progression or regression of disease (response to treatment) – Assist in forensic investigations Imaging • Mechanical energy (ultrasound) • Electromagnetic energy – RF (MR imaging) – Infrared (thermal) – Visible light (endoscopy, ophthalmology, dermatology) – Ultraviolet (fluorescence microscopy) – Gamma (radiographic imaging) – Protons (radiation therapy) Adult liver A 50 year old man with cirrhosis and worsening LFTs Adult liver: good news for this patient This is color flow and power Doppler: it shows that the blood vessels in the liver are not distorted by any “mass”. Obstetrical ultrasound How we do it: Workflow • I recommend review of the IHE Profiles for radiology if you are not already familiar with them • The profiles were developed largely through detailed examination of radiology workflow Scheduled Workflow Profile report report Registration report Report Repository HIS patient Diagnostic Workstation information PACS Film Lightbox images retrieved Orders Placed examination orders RIS Orders Filled procedure scheduled Image Manager Prefetch any relevant & Archive prior studies Acquisition modality images Modality worklist stored acquisition completed acquisition images in-progress completed printed Modality Film Folder Film Why are healthcare workflows so complex? • • • • Legacy procedures and systems We are idiosyncratic (Paul Chang) Interactions between departments Many personnel, each with particular tasks to perform and information needed Complex workflow: intraoperative ultrasound • We provide ultrasound in the operating room to assist the surgeons in locating structures and planning surgical approaches • About 20% of the time, the ultrasound changes the surgical plan Display during intraoperative scanning With permisson: Susan Rowling, MD, Frank Spitz, MD Display: the radiologist’s view Intraoperative ultrasound example A 41 year-old woman with colon carcinoma for resection ofa solitary liver mass The mass looks more like normal liver after compression This is NOT another metastasis – it is an hemangioma; a benign liver lesion. Intraoperative ultrasound • Often resulted in delays for both surgery and radiology • Surgeons had to wait for 20 minutes or more for us to arrive with our equipment • For radiology, it added to patient waiting time (took a radiologist and sonographer out of the Department) Basic workflow: Intraoperative liver Delays • We noted that some intraoperative ultrasound studies were subject to much greater delays than others • We thought that one difference was whether or not the study was scheduled in advance • We looked at the difference in workflow The non-scheduled workflow addition The non-scheduled workflow addition • Included more steps • Each step involved time • Once we showed how many more steps were involved, we discussed this with the surgeons and explained that scheduling ahead of time would result in shorter delays • They now routinely schedule their studies Intraoperative ultrasound • Illustrates that an already complex workflow in radiology, • Is made more complex when it involves interaction with another department’s workflow • Note that this does not even include the workflow steps done by surgery Intraoperative ultrasound • Also shows the need for standardization in the OR (hence the DICOM in Surgery WG) • There are vendor-based standards, but they are usually proprietary • There are standards (HDMI for video) that permit display on different devices, but not integration/interoperation Why is this stuff important for you? • Much of radiology workflow grew out of the film, paper, and pencil age • This includes not only processes, but organization • Radiology had been largely radiologycentric – This in a time when “patient centered” has become a goal Opportunities • Our workflow tends to be supported by thick client, customized software • It is neither agile nor adaptable • The rapid changes in healthcare have meant much more difficult transitions for our legacy information systems Big changes are coming • Remember the bit about “getting paid”? • Much of our (meaning healthcare in general) workflow is based on a fee for service model • The service-oriented specialties (radiology and pathology in particular) are effectively piece workers The approach to reducing healthcare costs • The US Government has, in response to escalating healthcare costs, attempted to fix this by reducing payments to hospitals and physicians • What is the logical response to reduced reimbursement per procedure? • Why, perform more procedures, of course! The newer model for reimbursement • Accountable care • Reimbursement is based on outcomes, cost reductions, and appropriateness rather than just what was done • How can radiology prepare for this? • It is why you are (or should be) hearing about quality measures, appropriateness criteria, and meaningful use Examples • CPOE – show that use improves appropriate requesting of imaging studies • ACR Imaging 3.0 • The Leapfrog Group - founded by large purchasers of healthcare services, mostly large corporations Importance for you (us) • We need to be agile and adaptable enough to provide the informatics and information technology resources to support changes in the way healthcare is practiced and reimbursed The emphasis • The emphasis will be (and is) on: – Rapid data mining – Increased patient involvement – Improved communication between healthcare providers – Demonstrating improvements in outcome – Proving increased efficiency Think about how these things can be accomplished • Do you want to continue to write monolithic thick client applications with numerous customizations? • And then have to debug, support, and update them? • This meeting gives me hope that there is a better way and you folks are practicing it