Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
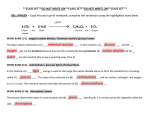
Impaired Glucose Transporter Activity in Pressure-Overload Hypertrophy Is an Early Indicator of Progression to Failure Ingeborg Friehs, MD; Adrian M. Moran, MD; Christof Stamm, MD; Steven D. Colan, MD; Koh Takeuchi, MD; Hung Cao-Danh, PhD; Christine M. Rader, BA; Francis X. McGowan, MD; Pedro J. del Nido, MD Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Background—Severe hypertrophy and heart failure are important risk factors in cardiac surgery. Early adaptive changes in hypertrophy include increased ventricular mass-to-cavity volume ratio (M/V ratio) and increased dependence on glucose for energy metabolism. However, glucose uptake is decreased in the late stages of hypertrophy when ventricular dilatation and failure are present. We hypothesized that impaired glucose uptake would be evident early in the progression of hypertrophy and associated with the onset of ventricular dilatation. Methods and Results—Ten-day-old rabbits underwent banding of the descending aorta. Development of hypertrophy was followed by transthoracic echocardiography to measure left ventricular M/V ratio. Glucose uptake rate, as determined by 31P-nuclear magnetic resonance spectroscopy measuring 2-deoxyglucose conversion to 2-deoxyglucose-6-phosphate, was measured in isolated perfused hearts obtained from banded rabbits when M/V ratio had increased by 15% from baseline (compensated hypertrophy) and by 30% from baseline (early-decompensated hypertrophy). In age-matched control animals, the rate of glucose uptake was 0.6160.08 mmol z g of wet weight21 z 30 min21 (mean6SEM). With a 15% M/V ratio increase, glucose uptake rate remained at control levels (0.660.05 mmol z g of wet weight21 z 30 min21), compared with hearts with 30% increased M/V ratios, where glucose uptake was significantly lower (0.4260.05 mmol z g of wet weight21 z 30 min21; P#0.05). Glucose transporter protein expression was the same in all groups. Conclusions—Glucose uptake rate is maintained during compensated hypertrophy. However, coinciding with severe hypertrophy, preceding ventricular dilatation, and glucose transporter protein downregulation, glucose uptake is significantly decreased. Because of the increased dependence of the hypertrophied hearts on glucose use, we speculate that this impairment may be a contributing factor in the progression to failure. (Circulation. 1999;100[suppl II]: II-187–II-193.) Key Words: hypertrophy n echocardiography n glucose n metabolism O ne of the earliest events during adaptive remodeling in pressure-overload hypertrophy is an increase in ventricular muscle mass; this is considered an initial compensatory response to maintain normal wall stress. If pressure overload persists, progressive ventricular dilatation ensues, which then leads to increased wall stress, afterload mismatch, and decreased cardiac output.1 Several adaptive mechanisms occur during the development of hypertrophy; these include the multiplication of sarcomeres,2 a switch to immature isoforms of contractile proteins,3 and greater dependence on transsarcolemmal calcium influx for excitation-contraction coupling.4 In addition, an increase occurs in glucose use as a substrate for energy production.5,6 The transition from compensated to decompensated hypertrophy with ventricular dysfunction is poorly understood. In mammalian cells, glucose is not freely permeable across the lipid bilayer; it enters the cells by facilitated diffusion. Specific membrane proteins that passively transport glucose down a concentration gradient achieve this process. In cardiac myocytes, 2 types of glucose transporters have been described (GLUT-1 and GLUT-4); they are responsible for most of the uptake of glucose under basal conditions and in response to insulin stimulation, respectively.7–14 We previously showed that the glucose uptake rate is impaired in hearts with decompensated pressure-overload hypertrophy when ventricular dilatation and contractile dysfunction have occurred in response to thoracic aortic banding.15 In light of the potential role of glucose metabolism in maintaining contractile function during the progression of pressure-overload hypertrophy, we hypothesized that im- From the Departments of Cardiac Surgery (I.F., C.S., K.T., H.C.-D., C.M.R., P.J.d.N.), Pediatric Cardiology (A.M.M., S.D.C.), and Anesthesiology (F.X.M.), The Children’s Hospital, Harvard Medical School, Boston, Mass. Correspondence to Pedro J. del Nido, MD, Department of Cardiac Surgery, Children‘s Hospital, Harvard Medical School, 300 Longwood Ave., Boston, MA 02115. E-mail [email protected] © 1999 American Heart Association, Inc. Circulation is available at http://www.circulationaha.org II-187 II-188 Circulation November 9, 1999 paired glucose transport occurs early in the progression to ventricular dilatation. In a rabbit model of thoracic aortic banding, we monitored the progression of hypertrophy using transthoracic echocardiography. In previous work with this model, we observed that after aortic banding, an initial increase occurs in the left ventricular (LV) mass to LV volume ratio (M/V ratio), which reaches a plateau '30% above prebanding levels. At this point, the rate of LV cavity volume increases faster than the rate of LV mass production, resulting in a fall in M/V ratio.16 This progression mimics the progression seen clinically with pressure overload.17 To determine the relationship between glucose uptake and progression of hypertrophy, we measured the glucose uptake rate and glucose transporter expression in control and aorticbanded rabbits during the early rise and the plateau phase of LV M/V ratio after aortic banding. modified KH solution containing 10 IU/L bovine insulin, a reduced glucose content (1 mmol/L), and a concentration of 3 mmol/L 2-deoxyglucose (2-DG; Sigma). 2-DG acts as a competitive inhibitor of glucose, and it is transported into the cell via the same mechanism (facilitative diffusion). Phosphorylation of 2-DG by hexokinase to 2-deoxyglucose-6-phosphate (2-DG-6-P) results in a distinct resonance peak. The rate of rise of this peak is proportional to glucose uptake by the cell and serves to quantify the rate of glucose uptake. The rate of degradation of 2-DG-6-P was determined in a separate group of hearts by perfusion with a KH buffer with 10 mmol/L glucose and 10 U/L insulin after the infusion of 2-DG and obtaining spectra for an additional 30 minutes. The rate of 2-DG accumulation (proportional to the rate of glucose uptake) was quantified by a second-order polynomial function. Glucose Uptake With [2-3H]Glucose Pressure-overload hypertrophy was achieved by placing a 2-0 silk suture around the descending aorta just distal to the ligamentum arteriosum in 10-day-old New Zealand White rabbits, as previously described.15 Implanting a fixed constriction in an immature animal and allowing it to grow induced pressure-overload hypertrophy by 2 to 3 weeks of age in this model. The progression of LV hypertrophy was determined by weekly transthoracic echocardiography (HewlettPackard Sonos 1500 Cardiac Imager) with a 7.5-MHz transducer. During these procedures, the animals remained unsedated to avoid the influences of anesthetics on the results. Glucose utilization was determined using the [2-3H]glucose method of Katz and Dunn.21 This method is based on the measurement of tritiated water (3H2O) production from [2-3H]glucose. 3H2O was separated from [2-3H]glucose by ion-exchange chromatography on a borate form of AG-1X8 resin (Bio-Rad Laboratories).22 Initially, the hearts were perfused with tracer-free perfusate for a stabilization period of 20 minutes; they were subsequently perfused in a nonrecirculating mode with KH buffer containing 50 mCi of [2-3H]glucose over a period of 30 minutes. The rate of 3H2O release was measured in the effluent withdrawn at 5-minute intervals, and 1 mL was dissolved in Insta-Gel Plus/XF solution (Packard Bioscience). Isotope counting was performed on a Beckman LS 6500 liquid scintillation counter (Beckman Instruments Inc). Rates of glucose uptake are reported as micromoles per grams of wet weight per minute (mmol z g of wet weight21 z min21). Echocardiography Hexokinase Activity Two-dimensional cross-sectional images and M-modes of the left ventricle were obtained by echocardiography. Simultaneous measurements of ECG and LV short-axis dimensions by M-mode were recorded on hard copy at a paper speed of 100 mm/s. These examinations were started at 3 weeks of age and performed at 1-week intervals. LV epicardial and endocardial surfaces were traced by computer-aided offline analysis on a bit-mapped digitizing tablet. End-diastolic (maximum dimension) and end-systolic (minimum dimension) LV wall thicknesses were determined using previously described methods.18 –20 The M/V ratio was calculated, and the serial evaluation of M/V ratio was expressed as percent change from baseline. Hypertrophied and control hearts from separate groups of animals were rapidly excised and perfused with modified KH solution for 5 minutes. The left ventricle was weighed, frozen in liquid nitrogen, and homogenized in a buffer containing (in mmol/L): TrisHCl 20, KCl 900, MgCl2 10, EDTA 2, and glucose 10 and 0.5% Triton (Sigma). The assay was performed on the homogenate in a buffer containing (in mmol/L): TrisHCl 40, KCl 100, MgCl2 20, EDTA 4, ATP 2, NADP1 0.25, and glucose 10 and 0.03 U of glucose-6phosphate dehydrogenase (Sigma). Control assays were performed on a buffer solution in which glucose or homogenate was omitted. The rate of reduction of NADP1 with glucose-6-phosphate dehydrogenase was measured spectrophotometrically at a wavelength of 340 nm. One milliunit of hexokinase represents the amount of enzyme activity that forms in 1 nmol of glucose-6-phosphate in 1 minute.23,24 Methods Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 2-Deoxyglucose Uptake Glucose uptake rate was determined using 31P-nuclear magnetic resonance (NMR) spectroscopy. Spectra were acquired in an 8.45 Tesla vertical Bruker spectrometer operating at a proton frequency of 145 MHz. The isolated heart in its perfusion chamber was positioned within a 20-mm solenoid radiofrequency coil. During the stabilization period of 30 minutes, the magnetic field was optimized by shimming on the free-induction decay of the proton signal from the heart and the surrounding perfusate. Spectra were obtained by signal-averaging 120 scans with a 2-s delay. Each spectrum took 4 minutes. Spectral peak areas were quantified by integration after baseline correction with software provided by Bruker. The determined areas were normalized to an external standard (using 500 mmol/L of dimethylene phosphonic acid) contained in a balloon adjacent to the heart. The animals were euthanized by intravenous injection of an overdose of ketamine (50 to 100 mg/kg); heparin (500 U/kg) was also given intravenously. The hearts were rapidly excised and placed in cold Krebs-Henseleit (KH) solution. After aortic cannulation, the hearts were perfused in the nonworking, nonrecirculating Langendorff mode at a perfusion pressure of 80 mm Hg with oxygenated KH solution containing (in mmol/L): NaCl 117, KCl 4.7, MgSO4 1.2, CaCl2 1.8, NaHCO3 23.7, and glucose 10 (37°C, pH 7.4). After a 30-minute stabilization period, the perfusate was switched to a Western Immunoblotting Ventricular tissue from a separate set of hypertrophied and agematched littermates (control animals) was homogenized in ice-cold buffer containing (in mmol/L): TrisHCl 20, EDTA 2, EGTA 0.5, and PMSF 1, and 25 mg/mL leupeptin and 0.3 mol/L sucrose (pH 7.4); it was then centrifuged at 1000g for 20 minutes. The crude supernatant fraction was stored at 280°C for later analysis. Gel electrophoresis with 10% SDS-PAGE gels was performed on samples of 25 mg of protein from total homogenates in accordance with the method of Laemmli.25 Proteins were then electrophoretically transferred to nitrocellulose membranes. After transfer, the membranes were incubated in 5% nonfat dry milk in 10 mmol/L TrisHCl (pH 7.5), 100 mmol/L NaCl, and 0.1% Tween 20 for 1 hour at room temperature to block unspecific binding sites; they were then incubated with antibodies. GLUT-1 and GLUT-4 (Genzyme Diagnostics) were used as primary antibodies at a dilution of 1:1000; samples were then incubated with horseradish peroxidase-conjugated secondary antibody (Jackson Immuno Research Labs) at a dilution of 1:10000. The bound antibody was detected by the enhanced chemoluminescence method according to the manufacturer’s instructions (Amersham Life Science). This method depends on the production of light after Friehs et al Glucose Transport in Pressure-Overload Hypertrophy II-189 the oxidation of luminol by horseradish peroxidase in the presence of H2O2. After exposure on films, quantitative protein analysis was undertaken by laser densitometry. Statistical Analysis Data are expressed as mean6SEM and were analyzed using SigmaStat software (Jandel Scientific). Comparisons between groups were made with 1-way ANOVA. Probability values were corrected by Bonferroni’s post hoc correction. If normality and equal variance testing were passed, a standard t test was used. For all these tests, P#0.05 was considered statistically significant. Animal Care All animals received humane care in compliance with the Principles of Laboratory Animal Care formulated by the National Society for Medical Research and the Guide for the Care and Use of Laboratory Animals prepared by the National Academy of Sciences and published by the National Institutes of Health (NIH Publication No. 86 to 23, revised 1985). The protocol was reviewed and approved by the animal care committee at Children’s Hospital in Boston. Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Results Weekly measurements of LV M/V ratios demonstrated that after aortic banding, an initial rapid increase of LV wall thickness occurred, resulting in a rise in LV M/V ratio. This reached a plateau '30% above prebanding levels by 3 to 4 weeks of age. We termed the phase leading up to this plateau “compensated hypertrophy.” By 4 to 5 weeks of age, a gradual decline in M/V ratio occurred due to a more rapid increase in LV cavity volume relative to LV mass, indicative of LV dilatation (decompensated phase). Figure 1 shows representative M-mode echocardiographic images of a heart with compensated hypertrophy and an age-matched control heart. On the basis of the echocardiographic findings, animals with a '15% increase in M/V ratio from baseline (4 weeks of age, compensated hypertrophy) and with a '30% rise in M/V ratio (5 weeks of age, early-decompensated phase) were studied and compared with age-matched control animals. Paralleling these echocardiographic findings, the banded animals showed a significant degree of hypertrophy, as estimated by LV weight to body weight ratios, which were 3.460.4 (compensated phase) and 3.360.4 (earlydecompensated phase) in the hypertrophied groups compared with 2.360.2 in controls. Body weights were not different between the groups, and LV weight was 3.0860.26 g in hearts with compensated hypertrophy, 2.8560.06 g in hearts with early-decompensated hypertrophy, and 2.1660.29 g in control hearts (P#0.05). 31 P-NMR spectra before and after a 30-minute infusion of 2-DG are shown in Figures 2A and 2B. Figure 2C depicts a representative curve of the 2-DG-6-P peak during 2-DG infusion and wash-out, indicating that 2-DG-6-P is not further metabolized during the observation period, even after subsequent wash-out with glucose-containing buffer. Figure 3A shows the rate of 2-DG-6-P accumulation over a period of 30 minutes in the aortic-banded groups and control animals. 2-DG accumulation was significantly lower in hearts with early-decompensated hypertrophy ('30% increase of M/V ratio) than in control hearts (P#0.05), with a slower rate of rise and lower total accumulation after 30 minutes. Figure 3B shows the rate of glucose uptake mea- Figure 1. Representative M-mode echocardiographic pictures from normal rabbit hearts (A) and those with compensated hypertrophy (B). Scale is not indicative of blood-pressure curve. sured by cumulative tritiated water production from [2-3H]glucose over a period of 30 minutes. In aortic-banded animals at a '30% rise of M/V ratio, the glucose-uptake rate was significantly lower compared with age-matched control animals (P#0.05). In a separate group of hearts (n54 per group), myocardial protein was obtained from the left ventricle of rabbits with compensated, early-decompensated, and late-decompensated hypertrophy (6 weeks of age, M/V ratio beginning to fall). The GLUT-1 and GLUT-4 protein content from the myocardium of aortic-banded groups and age-matched littermates, as determined by immunoblotting, was not significantly different between any of the groups. A representative immunoblot of GLUT-4 is depicted in Figure 4A, and a summary of the densitometry results is shown in Figure 4B. In a separate group of hearts perfused with KH solution containing insulin and glucose, total hexokinase activity was the same in hypertrophied and control hearts at a M/V ratio increase of '30% (38.260.47 mU/mg protein compared with 42.861.62 mU/mg protein, respectively). II-190 Circulation November 9, 1999 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Figure 2. Glucose uptake rate and phosphorylation were measured as accumulation of 2-DG-6-P by 31P-NMR spectroscopy over 30 minutes. A, Representative NMR-spectra (PCr indicates creatine phosphate assigned to 0 ppm; standard, dimethyl phosphoric acid; Pi, inorganic phosphate; and PME, phosphomonoester). B, Representative NMRspectra with typical 2-DG-6-P peak after addition of 2-DG to the perfusate. C, Representative 2-DG uptake curve: perfusion of hearts (n53; mean6SEM) with 2-DG over 40 minutes followed by 35 minutes of wash-out with glucose- and insulin-containing buffer (change of solutions indicated by arrows). Discussion In this study, echocardiography was used to monitor the progression of LV hypertrophy and to determine the timing for the study of glucose uptake and glucose transporter protein content. The observations derived from this investigation reveal that a decrease in glucose uptake rate is evident early in the transition from compensated to decompensated pressure-overload hypertrophy, as determined by an index of LV M/V ratio. The defect in insulin-stimulated glucose uptake precedes the downregulation of sarcoplasmic reticu- lum Ca-ATPase (SERCA-2) and glucose transporter expression (GLUT-4 and GLUT-1).15,26 Under pathophysiological conditions such as hypertrophy or during ischemia and early reperfusion, a high rate of cardiac glucose metabolism may be crucial.27–29 Glucose transport is thought to be rate-limiting for glucose use. In the heart, 2 distinctive glucose transporters are responsible for glucose uptake across the plasma membrane. The GLUT-1 transporter, which is present in low levels in most tissues, is non-insulin–stimulated and is responsible for basal glucose Friehs et al Glucose Transport in Pressure-Overload Hypertrophy II-191 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Figure 3. A, Glucose uptake rate and phosphorylation were measured as accumulation of 2-DG-6-P by 31P-NMR spectroscopy over 30 minutes in aorticbanded animals showing '15% increase in M/V ratio (3 to 4 weeks of age) and '30% rise of M/V ratio (4 to 5 weeks of age) and in age-matched littermates (controls; n56/group). *P#0.05 between groups. B, Glucose uptake rate determined by measuring cumulative tritiated water production from [2-3H]glucose in aortic-banded animals showing '30% rise of M/V ratio compared with agematched littermates (n55/group). *P#0.05 versus control. use.11,12 GLUT-4 activity is regulated by insulin and is expressed in tissues in which glucose transport needs to be rapidly and markedly enhanced (adipocytes, skeletal and cardiac muscle).13,14 In the basal state, GLUT-1 is evenly distributed between the plasma membrane and low-density microsomal pools, whereas GLUT-4 is almost entirely stored in an intracellular pool.14,30,31 Insulin interacts with its receptor on the plasma membrane and stimulates the redistribution of GLUT-4 to the sarcolemma.32,33 When insulin levels fall, GLUT-4 is resequestered in intracellular vesicles.34 A decrease in GLUT-4 mRNA and protein is thought to be a mechanism for insulin resistance in various models of diabetes, and it has been associated with lower myocardial glucose uptake.14,35–38 In the present study, we did not find altered GLUT-4 protein expression, as determined by immunoblotting of LV myocardial tissue, which indicates that insulin signal transduction and/or glucose transporter activity is altered in hypertrophied hearts. In the present study, we used the distinct 31P-NMR peak of 2-DG-6-P to investigate the glucose transport capacity of hypertrophied hearts. 2-Deoxy-D-glucose, a competitive inhibitor of D-glucose, is transported into the cell via the same mechanism as glucose, is phosphorylated by hexokinase, and accumulates as 2-DG-6-P, which is metabolized very slowly. The rate of 2-DG-6-P accumulation, therefore, reflects both transport across the plasma membrane and phosphorylation of glucose, and it is a useful tracer of glucose transport and phosphorylation in the isolated perfused heart.15,39 To confirm our findings with 2-DG uptake in hypertrophied hearts, we used a radioactive tracer technique; the same results were obtained. In some models, 2-DG-6-P is further metabolized by incorporation to glycogen at low rates.40 The rate of 2-DG6-P degradation is slow with respect to the rate of uptake; degradation rates ranging from 70 to 110 minutes have been previously reported.39,41,42 In the present study, 2-DG uptake II-192 Circulation November 9, 1999 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Figure 4. A, Representative immunoblot of total homogenates from hearts with compensated ('15% rise of M/V ratio), early-decompensated ('30% increase of M/V ratio from baseline), and latedecompensated hypertrophy (decline of M/V ratio indicating dilatation) compared with age-matched controls. B, Densitometry values (arbitrary densitometry units) for total homogenates of hearts with compensated, earlydecompensated, and latedecompensated hypertrophy and agematched controls (n54/group). reached a plateau after 30 minutes of perfusion, and little, if any, 2-DG-6-P was further metabolized during a wash-out period. Similar findings have been reported when hypertrophied and normal hearts were compared in a spontaneously hypertensive rat heart model.43 Therefore, we think that the use of 2-DG is a reliable method of glucose uptake determination in our model. In the current study, in hearts with compensated hypertrophy ('15% rise in M/V ratio), glucose uptake in response to insulin was still maintained at near-normal levels; impaired glucose uptake was detected before progression from compensated to decompensated hypertrophy at the peak M/V ratio ('30% above baseline). It is conceivable that the impaired response of GLUT-4 to insulin stimulation (eg, defects in insulin receptor signaling or alterations in GLUT4-containing vesicle trafficking) could contribute to the development of decompensated cardiac hypertrophy. Similar defects in the insulin-stimulation of glucose use and transport in the heart have been demonstrated in animal models of diabetes and insulin resistance.37,44 – 46 In the absence of insulin, glucose transport is rate-limiting for glycolysis, as reported for isolated rat cardiomyocytes.47 Therefore, an important relationship may exist between the progression of hypertrophy to failure and decreased glucose uptake because a diminished rate of cardiac glucose use is thought to be detrimental to heart function.48 We previously showed that severe hypertrophy with impaired glucose transport has functional significance with regard to impaired recovery after experimental myocardial ischemia. Normalizing glucose transport with vanadate significantly improved postischemic recovery in the hypertrophied heart.15 Our data indicate that a decline of glucose uptake rate occurs in the hypertrophied heart and, concomitantly with the lack of glucose available for the myocardium, hypertrophy progresses to myocardial failure. Insulin insensitivity of the GLUT-4 transport system, a potential underlying mechanism, may play a significant role. Because GLUT-4 protein levels remain unchanged at this stage, we speculate that impaired insulin signaling is responsible for this defect. Strategies to overcome this defect by either direct bypass of insulindependent GLUT-4 activation or augmenting glucose transport to the myocytes by other means may improve myocardial function and prevent the progression of hypertrophied hearts to failure. Acknowledgements This work was supported in part by grants from the American Heart Association (to P.J.d.N.) and the National Institutes of Health (HL 46207 to P.J.d.N. and HL 52589 to F.X.M.). References 1. Ross J Jr. Afterload mismatch and preload reserve: a conceptual framework for the analysis of ventricular function. Prog Cardiovasc Dis. 1976;18:225–264. 2. Izumo S, Nadal-Ginard B, Mahdavi V. Protooncogen induction and reprogramming of cardiac gene expression produced by pressure overload. Proc Natl Acad Sci U S A. 1988;85:339 –343. 3. Litten RZ, Low BJ, Alpert NR. Altered myosin isozyme patterns from pressure overloaded and thyrotoxic hypertrophied rabbit hearts. Circ Res. 1982;50:856 – 864. Friehs et al Glucose Transport in Pressure-Overload Hypertrophy Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 4. Chevalier B, Callens F, Charlemagne D, Delcayre C, Lompre AM, Lefievre L, Mercadier JJ, Moalic JM, Mansier P, Rappaport L, Samuel J, Schwartz R, Swynghedauw B. Signal and adaptational changes in gene expression during cardiac overload. J Mol Cell Cardiol. 1989;21:71–77. 5. Allard MF, Schonekess BO, Hening SL, English DR, Lopaschuk GD. Contribution of oxidative metabolism and glycolysis to ATP production in the hypertrophied heart. Am J Physiol. 1994;267:H742–H750. 6. Kagaya T, Kanno Y, Takeyama D, Ishida N, Maruyama Y, Takahashi T, Ido T, Takishima T. Effects of long-term pressure overload on regional myocardial glucose and fatty acid uptake in rat: a quantitative autoradiographic study. Circulation. 1990;81:1353–1361. 7. Mueckler M. Family of glucose-transporter genes: implications for glucose homeostasis and diabetes. Diabetes. 1990;39:6 –11. 8. Thorens B, Charron MJ, Lodish HF. Molecular physiology of glucose transporters. Diabetes Care. 1990;13:548 –564. 9. Mueckler M. Facilitative glucose transporters. Eur J Biochem. 1994;219: 713–725. 10. Bell GI, Kayano T, Buse JB, Burant CF, Takeda J, Lin D, Fukumoto H, Seino S. Molecular biology of mammalian glucose transporters. Diabetes Care. 1990;13:198 –208. 11. Stephens J, Pilch P. The metabolic regulation and vesicular transport of Glut-4, the major insulin-responsive glucose transporter. Endocr Rev. 1995;16:529 –546. 12. Kraegen EW, Sowden JA, Halstead MB, Clark PW, Rodnick KJ, Chisholm DJ, James DE. Glucose transporters and in vivo glucose uptake in skeletal and cardiac muscle: fasting, insulin stimulation and immunoisolation studies of Glut-1 and Glut-4. Biochem J. 1993;295:287–293. 13. Kahn BB. Facilitative glucose transporters: regulatory mechanisms and dysregulation in diabetes. J Clin Invest. 1992;89:1367–1374. 14. Slot JW, Geuze HJ, Gigengack S, James DE, Lienhard GE. Translocation of the glucose transporter Glut-4 in cardiac myocytes of the rat. Proc Natl Acad Sci U S A. 1991;88:7815–7819. 15. Takeuchi K, McGowan FX, Glynn P, Moran AM, Rader CM, Cao-Danh H, del Nido PJ. Glucose transporter upregulation improves ischemic tolerance in hypertrophied failing heart. Circulation. 1998(suppl II);98: II-234 –II-241. 16. Moran AM, Takeuchi K, McGowan FX, Colan SD, del Nido PJ. Functional and molecular changes with progression to contractile failure in the hypertrophied/immature myocardium. Pediatr Res. 1998;43:24A. Abstract. 17. Thurman PA. Left ventricular and microvascular hypertrophy in essential hypertension: clinical relevance and prognostic implications. Int J Clin Pharmacol Ther. 1997;35:181–187. 18. Colan SD, Sanders SP, Borow KM. Physiologic hypertrophy: effects on left ventricular systolic mechanics in athletes. J Am Coll Cardiol. 1987; 9:776 –783. 19. Colan SD, Borow KM, Neumann A. Left ventricular end-systolic wall stress-velocity of fiber shortening relation: a load-independent index of myocardial contractility. J Am Coll Cardiol. 1984;4:715–724. 20. Colan SD, Borow KM. Effects of loading conditions and contractile state on left ventricular early diastolic function. J Am Coll Cardiol. 1985;55: 790 –796. 21. Katz J, Dunn A. Glucose-2-t as a tracer for glucose metabolism. Biochemistry. 1967;6:1–5. 22. Marshall RC, Nash WW, Shine KI, Phelps ME, Ricchiuti N. Glucose metabolism during ischemia due to excessive oxygen demand or altered coronary flow in the isolated arterially perfused rabbit septum. Circ Res. 1981;49:640 – 648. 23. Postic C, Leturque A, Printz RL, Maulard P, Loizeau M, Granner DK, Girard J. Development and regulation of glucose transporter and hexokinase expression in rat. Am J Physiol. 1994;266:E548 –E559. 24. Katzen HM, Schimke RT. Multiple forms of hexokinase in the rat: tissue distribution, age dependency and properties. Proc Natl Acad Sci U S A. 1965;54:1218 –1225. 25. Laemmli UK. Cleavage of structural proteins during the assembly of the head of bacteriophage T4. Nature. 1970;227:680 – 685. 26. Qi M, Shanon TR, Euler DE, Bers DM, Samarel AM. Downregulation of sarcoplasmic reticulum Ca21-ATPase during progression of left ventricular hypertrophy. Am J Physiol. 1997;272:H2416 –H2424. 27. Takeuchi K, Buenaventrua P, Cao-Danh H, Glynn P, Simplaceanu E, McGowan FX, del Nido PJ. Improved protection of the hypertrophied left 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. II-193 ventricle by histidine containing cardioplegia. Circulation. 1995;92(suppl II):II-395–II-399. Taegtmeyer H, Goodwin GW, Doenst T, Frazier OH. Substrate metabolism as a determinant for postischemic functional recovery of the heart. Am J Cardiol. 1997;80:3A–10A. Opie LH. Myocardial ischemia: metabolic pathways and implications of increased glycolysis. Cardiovasc Drugs Ther. 1990;4:777–790. Kahn BB, Charron MJ, Lodish HF, Cushman SW, Flier JS. Differential regulation of two glucose transporters in adipose cells from diabetic and insulin-treated diabetic rats. J Clin Invest. 1989;84:404 – 411. James DE, Strube M, Mueckler M. Molecular cloning and characterization of an insulin-regulatable glucose transporter. Nature. 1989;338: 83– 87. Cheatham B, Vlahos CJ, Cheatham L, Wang L, Blenis J, Kahn CR. Phosphatidylinositol 3-kinase activation is required for insulin stimulation of pp70 S6 kinase, DNA synthesis, and glucose transporter translocation. Mol Cell Biol. 1994;14:4902– 4911. Hausdorff SF, Bennett AM, Neel BG, Birnbaum MJ. Different signaling roles of SHPTP2 in insulin-induced GLUT 1 expression and GLUT 4 translocation. J Biol Chem. 1995;270:12965–12968. Holman GD, Cushman SW. Subcellular localization and trafficking of the GLUT 4 glucose transporter isoform in insulin-responsive cells. Bioessays. 1994;16:753–759. Garvey WT, Maianu L, Huecksteadt TP, Birnbaum MJ, Molina JM, Ciaraldi TP. Pretranslational suppression of a glucose transporter protein causes insulin resistance in adipocytes from patients with non-insulindependent diabetes mellitus and obesity. J Clin Invest. 1991;87: 1072–1081. Sinha MK, Raineri-Maldonado C, Buchanan C, Pories WJ, Carter-Su C, Pilch PF, Caro JF. Adipose tissue glucose transporters in NIDDM: decreased levels of muscle/fat isoform. Diabetes. 1991;40:472– 477. Garvey WT, Hardin D, Juhaszova M, Dominguez JH. Effects of diabetes on myocardial glucose transport system in rats: implications for diabetic cardiomyopathy. Am J Physiol. 1993;264:H837–H844. Kainulainen H, Breiner M, Schurmann A, Marttinen A, Virgo A, Joost HG. In vivo glucose uptake and glucose transporter proteins Glut-1 and Glut-4 in heart and various types of skeletal muscle from streptozotocindiabetic rats. Biochim Biophys Acta. 1994;225:275–282. Takala TES, Hassinen IE. Effect of mechanical work load on the transmural distribution of glucose uptake in the isolated perfused rat heart, studied by regional deoxyglucose trapping. Circ Res. 1981;49: 62– 69. Doenst T, Taegtmeyer H. Complexities underlying the quantitative determination of myocardial glucose uptake with 2-deoxyglucose. J Moll Cell Cardiol. 1998;30:1595–1604. Jenkins AB, Furler SM, Kraegen EW. 2-deoxy-D-glucose metabolism in individual tissues of the rat in vivo. Int J Biochem. 1986;18:311–318. Krivokapich J, Huang SE, Selin CE, Phelps ME. Fluorodeoxyglucose rate constants, lumped constant and glucose metabolic rate in rabbit heart. Am J Physiol. 1987;52:H777–H787. Paternostro P, Clarke K, Heath J, Seymour A-ML, Radda GK. Decreased Glut-4 mRNA content and insulin-sensitive deoxyglucose uptake show insulin resistance in the hypertensive rat heart. Cardiovasc Res. 1995;30: 205–211. Stroedther D, Schmidt T, Bretzel RG, Federlin K. Glucose metabolism and left ventricular dysfunction are normalized by insulin and islet transplantation in mild diabetes in the rat. Acta Diabetol. 1995;32:235–243. Eckel J, Reinauer H, Wirdeier A, Herberg L. Insulin resistance in the heart: studies on isolated cardiocytes of genetically obese Zucker rats. Endocrinology. 1985;116:1529 –1534. Zaninetti D, Assimacopoulos-Jeannet F, Jeanrenaud B, Greco-Perotto R. Dysregulation of glucose transport and transporters in perfused hearts of genetically obese (Fa/fa) rats. Diabetologia. 1989;32:56 – 60. Manchester J, Kong X, Nerbonne J, Lowry OH, Lawrence JC Jr. Glucose transport and phosphorylation in single cardiac myocytes: rat-limiting steps in glucose metabolism. Am J Physiol. 1994;266:E326 –E333. Zorzano A, Sevilla L, Camps M, Becker C, Meyer J, Kammermeier H, Munoz P, Guma A, Testar X, Palacin M, Blasi J, Fischer Y. Regulation of glucose transport, and glucose transporters expression and trafficking in the heart: studies in cardiac myocytes. Am J Cardiol. 1997;80: 65A–76A. Impaired Glucose Transporter Activity in Pressure-Overload Hypertrophy Is an Early Indicator of Progression to Failure Ingeborg Friehs, Adrian M. Moran, Christof Stamm, Steven D. Colan, Koh Takeuchi, Hung Cao-Danh, Christine M. Rader, Francis X. McGowan and Pedro J. del Nido Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Circulation. 1999;100:II-187-Ii-193 doi: 10.1161/01.CIR.100.suppl_2.II-187 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1999 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/100/suppl_2/II-187 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/