Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Specific language impairment wikipedia , lookup
Auditory system wikipedia , lookup
Volta Laboratory and Bureau wikipedia , lookup
Sign language wikipedia , lookup
Telecommunications relay service wikipedia , lookup
Noise-induced hearing loss wikipedia , lookup
Video relay service wikipedia , lookup
Sensorineural hearing loss wikipedia , lookup
Deaf culture wikipedia , lookup
Hearing loss wikipedia , lookup
Audiology and hearing health professionals in developed and developing countries wikipedia , lookup
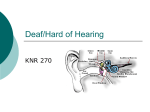
Becky Tueller Tueller 1 Nikki Mantyla English 1010-062 3 December 2011 Do You Hear What I Hear? Cochlear Implants And Children: Do They Go Hand in Hand? After uttering those legendary words, “Mr. Watson, come here…I want to see you.” I doubt Alexander Graham Bell (AG Bell) had any idea his telephone invention would play such an important role in the lives of individuals for generations to come. The idea of the telephone began many years prior to its birth. Author Harlan Lane recounts the story of AG Bell as a young boy. Alexander would sit at his dining table in preparation of his evening meal. Every night would be the same as the evening before: he would not be eating his tender morsels—at least not right away. Seated at the table with him were his mother, other relatives, and friends. Born hearing, his mother had gained a good grasp of speech, but illness had robbed her of her auditory senses; she was left without sound. She had learned to fingerspell to compensate for her hearing loss, but did not use sign language. This family of high stature often had dignitaries over for dinner. His mother did not want to be left out of any conversation and Alexander also knew how to fingerspell: so, without lifting his fork to his mouth as the others did, he proceeded to convey the conversation to his mother through fluttering fingers. As dinner concluded, the guests departed the dining area; it was only then that Alexander was finally allowed to eat his meal. The plate that once danced with color and flavor, now seems flat and lifeless; it resembles the cold resentment mounding in his heart towards his mother’s deafness. This same event continued day after day, year after year, the bitterness swelling within him. Ironically, Alexander married a woman in exactly the same situation. She was born hearing and learned to talk, but had become ill as a child and was left with very little residual hearing. AG Bell Tueller 2 was a brilliant man and very influential in society. He was able to invent a contraption his wife could wear to parties, in which she would place a small amplifier on a belt around her waist; there was one tube that came up to her ear with an earpiece attached to it, and another tube with a cone–shaped funnel end that a person could talk into; the amplifier would allow her to pick up parts of the conversation taking place. This was essentially the first modern hearing aid (Lane WTMH). The creation of hearing aids has benefitted countless individuals with hearing loss ranging anywhere from mild to severe; however, through the evolution of hearing aids comes one of the most controversial topics in Deaf culture: the use of cochlear implants. Despite the fact that in recent decades cochlear implants (CIs) have improved the quality of communication for many deaf individuals, researchers are not in total agreement on the positive outcome of their use: especially in children; children who do not have a voice to speak for themselves. These children are suspended between the Deaf and hearing worlds; but not really finding a place in either: where do they belong? Taking a closer look at the issues involving cochlear implantation in children, we will gain a better insight into the attitudes between the Deaf and hearing worlds towards deafness, the process and side-effects associated with receiving a CI, and choices parents should consider when making this life changing decision. With so much at stake, should there be laws or restrictions in place to prevent parents from imposing this irreversible procedure on young children? To allow individuals to be old enough to decide for themselves if this is the right choice for them—it is their body after all—is a basic human right. There is a tremendous gap in attitudes between the hearing and Deaf communities in regards to CIs. Having spent time as a sign language interpreter, I have been exposed to and seen first-hand Tueller 3 how these attitudes penetrate both communities. Even the very word “deaf” has different connotations. The usage of the word deaf (with a lower case d) refers to a person’s inability to hear sound. This classification is used as a medical term to describe a defect or handicap involving the ear’s function. Conversely, the usage of the word Deaf (with a capital D) refers to a sense of pride an individual feels regarding the rich culture and tight–knit community they hold so dear. They cherish their interaction with each other and share common challenging experiences; they support, encourage, and learn from one another. In essence, the word deaf tells them what they cannot do and the word Deaf tells them what they can do. It is these differences in attitudes that have created a need—on the part of the hearing community—for deaf individuals to be cured or made “normal.” Many researchers have performed studies on children who have been embedded with CIs as young as twelve–months–old. Much of the data supporting the claims that children gain more complete language skills if a child acquires an implant at an early age is very impressive. According to one research report performed by the Indiana University School of Medicine, 54 percent of the deaf children in their study claimed that, with a great deal of therapy, a five-year-old can have language learning levels that are almost equivalent to a hearing child of the same age (Svirsky). Similar data was backed up by a study by the International Journal of Pediatric Otorhinolaryngology studying children embedded with two implants (Scherf, et.al.). However, other research suggests that the evidence may not be as conclusive as it appears and the numbers may be slightly skewed. New research indicates that children with CIs are not learning at the same rate or equivalent to their hearing counterparts. In fact, by the time deaf children with CIs graduate from mainstream (public) high school, research has found that most students have a reading comprehension level of a fourth grader—not exactly equivalent. In evaluating the studies supporting the use of CIs, it has been found Tueller 4 that they were selective with the candidates utilized in the testing process and the test scores only seemed to improve in two out of the seven areas being tested. (Lane MOB). Recognizing the value of CIs, I have been fortunate to teach sign language in mainstream high schools for the past five years. Almost all of my students are hearing. Last year, I had a wonderful sixteen year old student named Josh. Josh is deaf. He is one of the only deaf individuals that I personally know that has chosen to have two CIs. In talking to him, I discovered that he did not get them both at the same time. His parents chose to have the first surgery when he was two-years-old. During his preschool and early elementary years, he was enrolled in special programs and began to learn American Sign Language (ASL) as well as speech therapy. By the time he was in second grade, he was able to use his new found language skills, by connecting English through signing and speech. He progressed and adjusted very well, but felt like he was still missing out on some things, so when Josh was twelve, he decided for himself to have his second CI. For him, this decision has been very successful. He is grateful to hear what he can, and thankful his parents made this choice for him (Josh): Josh is the exception, not the rule; most are not as successful; most do not use ASL in their education. Regrettably, AG Bell’s adverse attitude towards deafness influences hearing society still today. About two hundred years ago, ASL was introduced in the United States. For the first time deaf children were finally able to communicate their thoughts and desires. ASL flourished and hearing people realized that deafness didn’t mean a lack of intelligence: these children could be taught. Many Deaf students grew to become teachers; they positively influenced younger students to believe they could achieve anything they worked for. AG Bell did not approve of the direction this explosion of ASL was heading. His father was a great teacher of oralism and, he too, felt this was the only pure Tueller 5 form of speech. Because of his connections with people in high political positions, he was able to influence many people to accept and pass the banning of ASL in educating deaf children; the only form of teaching deaf children would be oralism and speech training (Gannon). ASL was no longer allowed in schools, children were punished and their hands were tied together if they were caught signing. Hearing society has been persuaded to accept that the only way deaf children can learn English and be fully integrated into the hearing world, is to learn to speak. This is the same attitude many medical professionals (and much of hearing society) still hold true today. On the flip side, members of the Deaf community accept and embrace their deafness. Most do not view their deafness as a disability. They view themselves as an individual that can do anything a hearing person is capable of doing: except hear. They are bright, competent individuals that have a strong desire to be self-reliant. An interpreter may be needed in some circumstances for equal opportunities to acquire information. If the interpreter is skilled, the deaf person is just as knowledgeable as any hearing person. It was working as an interpreter that I gained my perspective of the frustrations and oppression deaf individuals experience on a daily basis living in a hearing world. Furthermore, I have a close family friend who is Deaf, his name is Greg. Recently, he was involved in a conversation with my sister-in-law. She was questioning Greg to see if he would ever pursue receiving a CI. Without hesitation came an emphatic NO! She could not understand that he would prefer to remain in silence when technology has created something so wonderful to make him more “normal” (or acceptable) and allow him to “get over” his handicap. He tried to explain that the Deaf community is proud of their culture and heritage. They do not necessarily support the use of CIs and that those who have them are denying the fact that they are Deaf and missing out on that rich heritage. His feelings are [much the same as most Deaf people] that God created him the way he is Tueller 6 and that is something to be celebrated. He has been given some challenges to face in life, but so has everyone . . . some people need glasses, does that make them less of a person? In his mind, there is nothing wrong with him; hearing people are the ones reminding him he is not whole. He said, “You wouldn’t tell an African American with a family history of slavery to “just get over it.” The Deaf community has very much the same deep ties to culture through shared oppressive experiences.” This was something my sister-in-law could not fathom, and the conversation came to an abrupt end (Greg). This is a common example of the frustration Deaf people experience when trying to educate hearing people about deafness (and CIs). Prior to 1990, CIs were only approved for adult use. In the summer of 1990, the U.S. Food and Drug Administration (FDA) approved the use of CIs in children ages 2-17. Today they are approved for babies as young as six–months–old. Since 9 out of 10 deaf children are born to hearing parents, my student Josh is representative of what most deaf children experienced when the decision to receive a CI becomes an option. As a baby, the parents suspect there is something “not quite right” with their child. They go to the doctor were their greatest fears are confirmed. The doctor will stand behind the child and clap or create loud noises: the child does not respond. The parents are then referred to an audiologist that performs a series of hearing tests. If the child is a good candidate for a CI—and even if they are not—, the parents are bombarded with information and statistics of the benefits of cochlear implantation and how their children will have a more “normal” life. Bear in mind, “the CI industry has mounted a successful marketing campaign, playing on the hopes and fears of parents” (Moore). Parents want to make choices that will bring happiness to their children, and deep down they want their children to have a “normal” life, so the decision is made to surgically embed the CI: rarely are these parents encouraged to contact or seek out anyone involved in the Deaf Tueller 7 community to get a different perspective. Medical professionals focus more on fixing the defect than they do the emotional effects on a child—who is constantly reminded by hearing society they are not “normal.” The process of embedding a CI is painful, evasive and irreversible. Externally, the deaf individual wears a device on their ear that looks very much like a hearing aid, but does not work exactly like one. The ear piece has a microphone that receives and passes information along to an external transmitter that is held magnetically in place just behind the ear; an internal receiver is surgically drilled and implanted in the skull beneath the transmitter and receives the information; a wire containing several electrodes are run from the receiver to the inner ear called the cochlea, where the electrodes stimulate the auditory nerve with the new information. It is during this implantation process that the great controversy is verified. As the electrodes are being inserted and wound through the “snail” shaped cochlea, sensitive tissue is destroyed: tissue that can never be repaired. From that moment on, all residual hearing is lost. In addition to the painful surgery, the patient requires one month of healing before any external hardware can be tested: for one month there is complete silence in that ear. When the healing is complete, the real test begins. Most children know immediately if their hearing is improved; however, they will spend several months or even years learning to interpret the electronically processed sounds they hear into meaningful speech. Parents are informed that if they learn and use ASL, their children will never learn to speak properly (Lane MOB ). They are required to commit to a grueling oral/speech program—there is no room for sign language. Some children will thrive in this environment; others will struggle and fail. My student Josh went through years of training and therapy to know how to use his CIs and understand what he was listening to. He mentioned to me, “While all the other [hearing] kids were outside Tueller 8 playing during the summer or sleeping in, I wasn’t, I was at speech therapy” (Josh). This is a common occurrence; many tedious hours of training are required to interpret the new information they receive, while the world seems to be passing them by—without ASL they will never catch up. Besides extensive speech training, there are other side-effects associated with receiving CIs: the body could painfully reject the new device; the equipment may get damaged or malfunction; there is a total loss of residual hearing in the implanted ear; the sounds transmitted are mechanical and raspy, almost robotic, compared to true acoustic sound; the process produces vibrations in the brain that can cause severe headaches and nausea; there is a loss of pitch perception leaving sounds monotone; very limited “surround sound”, inaccurate sound perception in speech and background noises; lower levels of self-esteem compared to hearing children; and high risk of bacterial meningitis and other recurring infections. In a report by the New England Journal of Medicine addressing bacterial meningitis, it is claimed that children six years and younger with CIs are 30 times more likely than the general population to contract bacterial meningitis. Parents and health-care providers are encouraged to ensure that all children with CIs are appropriately vaccinated and monitored so they can be treated promptly for any bacterial infection to reduce risks involved (Reefhuis). With so much at risk, parents need to do their homework when making this life changing decision for their child. Besides medical advice, parents should research multiple viewpoints to weight the costs and benefits. Talking to other parents who have made this choice for their children and contacting Deaf individuals for feedback will be of the greatest benefit to parents. They should also seriously consider the use of ASL to provide immediate communication to the child; ASL could very well be a missing link between the two worlds (Hintermair). If you think about it, a hearing child at the age of three is just beginning to express clearly his needs and wants through a spoken Tueller 9 language; deaf children are often five before they can express the same desires (Christiansen). Years of frustration could be eliminated if a deaf child were able to use his first language: ASL. It is critical to get language to a child immediately from birth. Hearing babies start to receive spoken language the moment they are born, but speech does not give them a language overnight. Even hearing babies recognize and respond to gestures long before they are able to communicate using speech (Moore). A clear example of this was demonstrated to me when my first grandchild was born. Although he is hearing, we began signing to him regularly when he was a month old. When he was eight months, he was able to use twelve signs to express his wants, and by the time he was one year, he was using twenty-five signs on a regular basis. The advantage to this method of language was; he never cried. He could indicate exactly what he needed in a meaningful way we could understand with very little frustration for everyone involved. The downside to this method was the other grandparents were not aware of all the signs he was using, as a result, at times they were frustrated; they knew he was trying to communicate with them, but they did not know his system well enough. This is one of the pitfalls deaf children face. Often parents and family members are unwilling to commit to the time it takes to learn this form of communication, it’s just too much trouble; instead they desire the children to be like them: hearing—they want to undo deafness. Many deaf adult express some resentment towards their parents for putting them through years of speech training instead of their parents learning to sign; they complain about speech training, but rarely complain about ASL training. Interestingly, Josh told me that even though he has better hearing due to his CIs, he still considers himself very much a visual learner and is grateful he was taught ASL (Josh). In addition to exploring the idea of teaching their children ASL, parents should also take a closer look at other questions before this permanent decision is made: Does this surgery benefit all Tueller 10 deaf people the same? How do I know for sure if my child has any residual hearing before we destroy the cochlea? What special needs will my child have after implantation? Will there be self-esteem issues that the use of ASL could lessen? Where will my child fit—hearing or Deaf world? What is truly best for my child—not me? Should I be the one to make this decision for my child? Although many hearing people are under the assumption that early implantation can provide normal hearing advantages in deaf children, and that they will learn language equivalent to their hearing counterparts: CIs will not make these children hearing. In fact, research suggests that if a very young, profoundly deaf child, without a language base is implanted too early, there is no sound recognition and the child would be better suited with the use of a regular hearing aid (Christiansen). The evasive surgery and powerful hearing aids hold the same benefit, so why would parents choose a risky surgery for their child? Many people, both hearing and Deaf, believe that the consequences of this irreversible procedure should not be performed on children that cannot voice their own opinion about what they may want for themselves. Laws are established for parents to make life-threatening choices in behalf of their children, but this is not a life-threatening situation. Who will be an advocate for these children, if not the parents? I would have to place my voice with those who believe that there should be at least restrictions placed on the age of children receiving CIs: these children should be allowed to be part of the process of deciding what happens to their bodies. There is just not enough evidence to prove early implantation provides the best answer for deaf children. We as a hearing community need to step away from the narrow-minded attitude in which AG Bell viewed deaf individuals and truly accept them the way they are, as valued human beings—not a broken ear with a body attached to it. Only then will deaf people be allowed to be Deaf. Works Cited Christiansen, John B. and Irene Leigh. Cochlear Implants in Children: Ethics and CHoices. Washington, DC 20002: Gallaudet University Press, n.d. 2002 Gannon, Jack R. Deaf Heritage: A Narrative History of Deaf America. Silver Springs: National Association of the Deaf, 1981. Greg. Would You Get A Cochlear Implant? Becky Tueller. 4 July 2011. Hintermair, M. &J. Abertini. "Ethics, Deafness, and The New Medical Technologies." Journal of Deaf Studies and Deaf Education (2005): 10, 184-192. Josh. Your Experience With Cochlear Implants Becky Tueller. 15 November 2011. Lane, Harlan. The Mask of Benevolence: Disabling the Deaf Community. 1992; rpt. San Diego: DawnSign Press, 2000. Lane, Harlan. When the Mind Hears: A History of the Deaf. 1984; rpt. New York: Pelican, 1999. Moore, Matthew S. and Linda Levitan. For Hearing People Only. Rochester: MSM Productions, Ltd., 2009. Reefhuis, Jennita, Ph.D., et al. "Risk of Bacterial Meningitis in Children with Cochlear Implants." New England Journal of Medicine (2003): 349:435-445. Scherf, Fanny, et al. "Hearing Benefits of Second-side Cochlear Implantation in Two Groups of Children." International Journal of Pediatric Otorhinolaryngology (Aug 2007): 71, 1855-1863. Svirsky, Mario A, Amy M Robbins, Karen Iler Kirk, David B Pisoni, and Richard T Miyamoto. "Language Developement in Profoundly Deaf Children with Cochlear Implants." Psychological Science (2000): Volume 11, Number 2.