Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Globalization and disease wikipedia , lookup
Rheumatic fever wikipedia , lookup
Gastroenteritis wikipedia , lookup
Appendicitis wikipedia , lookup
Neonatal infection wikipedia , lookup
Infection control wikipedia , lookup
Hepatitis B wikipedia , lookup
Hepatitis C wikipedia , lookup
Schistosomiasis wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Kawasaki disease wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Marburg virus disease wikipedia , lookup
An Arteriosclerotic Aneurysm of the Abdominal
Aorta Secondarily Infected with Group C,
Beta-hemolytic Streptococci
Report of a Case
D E N V E R E. P E R K I N S , J R . , M.D., AND R. P A R K E R M C R A E , B.A.
Department of Pathology, Vanderbilt University School of Medicine, Nashville, Tennessee 3 7232
ABSTRACT
Perkins, Denver E., Jr., and McRae, R. Parker: An arteriosclerotic aneurysm
of the abdominal aorta secondarily infected with group C, beta-hemolytic
streptococci. Report of a case. Am. J. Clin. Pathol. 62: 646-648, 1974. A
59-year-old man was admitted to the Nashville Veterans Administration
Hospital for evaluation of fever, weight loss, and nausea and vomiting of
one month's duration. Subsequently he was found to have an aneurysm of
the abdominal aorta 8 cm. in diameter, secondarily infected with group C
beta-hemolytic streptococci. T h e aneurysm was not resected, and in spite of
theoretically adequate antibiotic therapy, the aneurysm ruptured and
exsanguination occurred. No case similar to ours was found in a review of
the literature concerning mycotic aneurysms of the abdominal aorta.
Aneurysms of the abdominal aorta which became infected with bacteria are
difficult therapeutic problems. Surgical resection of such lesions carries, at
most institutions, a mortality rate greater than 95%. There are only six
reported long-term survivors of this procedure. (Key words: Aneurysm,
myotic; Aorta; Beta-hemolytic streptococci.)
IN 1967, Bennett and Cherry reviewed
the world literature on secondarily infected arteriosclerotic abdominal aneurysms and discovered only 34 reported
cases. 2 T h e most common causative
organism was found to be Salmonella,
followed by Staphylococcus. Species of
streptococci have rarely been implicated,
and a careful review of the literature
reveals that a case of an arteriosclerotic
abdominal aneurysm secondarily infected
Received April 22, 1974, accepted for publication
May 8, 1974.
Address reprint requests to Dr. Perkins, 3808
Amhurst, Dallas, Texas 75225.
646
with group C beta-hemolytic streptococci
has not been previously reported. Group
C beta-hemolytic streptococci a r e infrequently associated with human disease;
only two cases in which death was attributed to documented infection with this
organism have been reported. 3
Report or a Case
A 59-year-old farmer was admitted to
the Nashville Veterans' Administration
Hospital for evaluation of fever, weight
\oss nausea and vomiting, and intermit.
.
,.
, , .
Singultus, of one month s duration.
Past history was not contributory.
t e n t
November 1974
GROUP C STREPTOCOCCAL MYCOTIC ANEURYSM
*%
•
':.
•
647
J
u
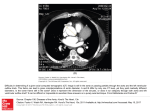
FIG. 1 (upper). This section through the aorta at a point adjacent to the site of rupture demonstrates
the marked loss of smooth muscle and elastic fiber. Verhoff-Van Gieson tain, x 12.8.
FlG. 2 {lower). Colonies of Gram-positive cocci are present in this section of the media
of the aorta. Brown and Brenn stain. x320.
Physical examination revealed only one
pertinent symptom—a diffusely tender
abdomen. T e m p e r a t u r e was 100.5 F.,
leukocyte count 13,600, and hematocrit
32%. Cultures of blood drawn on the first,
fourth, eighth, and tenth hospital days
were positive for group C beta-hemolytic
streptococci. (Identification was estab-
648
PERKINS AND McRAE
A.J.C.P.—Vol.62
lished by acid-heat precipitation.) Sub- ness of the aorta. At the point of rupture,
sequent to the first report of a positive the elastic and smooth muscle fiber of the
blood culture (tenth hospital day), the media abruptly disappeared, and the aorpatient received 20 million units of aque- tic wall became, essentially, a thin band of
ous penicillin per day, intravenously, via a fibrous tissue apposed to adventitia (Fig.
continuous-drip system for 36 days. For 1). Colonies of Gram-positive cocci were
seven days thereafter, he received 20 present both in the media and in an
million units of aqueous penicillin per organized t h r o m b u s beneath an arday, intravenously, divided into four teriosclerotic plaque adjacent to the point
equal doses. A Schlichter test, performed of rupture (Fig. 2).
with serum drawn during the thirteenth
Conclusion
day of antibiotic treatment, demonstrated
that the patient's serum was cidal to the
Infection greatly increases the likeliinfecting organism at dilutions of 1:1,024.
hood of rupture of an arteriosclerotic
An a o r t o g r a m p e r f o r m e d o n t h e
aneurysm, an event with an almost invarithirty-fourth hospital day revealed a sacably fatal outcome. 4
cular aneurysm in the infrarenal aspect of
This case demonstrates well that anthe abdominal aorta. An exploratory
tibiotics are ineffective in treating bactelaboratomy was performed, a n d the
rial infections sequestered beneath araneurysm was found to be inflamed and
teriosclerotic plaques.
surrounded by an intense fibrotic reacThe logical alternative to the use of
tion. It was judged to be infected and
antibiotics alone, the use of antibiotics
unresectable. Two weeks postoperatively,
before and after surgical resection of the
the aneurysm ruptured and the patient
aorta, carries a mortality rate greater than
died of acute hemorrhage.
95%. 4 There are only six reported cases of
long-term survival (more than a year and
Autopsy Findings (AVN-101-73)
a half) following resection of an abdomiThe peritoneal cavity was filled with nal aneurysm infected by bacteria, and
approximately 3 liters of blood. A ret- three of these cases were reported by a
,,5>6
roperitoneal hematoma extended from single group.
the inferior surface of the right leaf of the
References
diaphragm to the floor of the pelvis. A
1. Austin DJ, Thompson JE, Patman DR, et al:
saccular aneurysm 9 cm. long and 8 cm.
Infected arteriosclerotic aneurysm of the abin diameter, with a 4 cm. longitudinal rent
dominal aorta. Am J Surg 118:950-952, 1969
2. Bennet DE, Cherry JK: Bacterial infection of
along the right posterolateral aspect, was
aortic aneurysms. Am J Surg 113:321-326,
present in the infrarenal aspect of the
1967
3. Bullock JD, Cruz MG, Rabin ER, et al: A fatal
abdominal aorta. An intense inflammation
case of group C streptococcal endocarditis.
surrounded the aneurysm, and tracts of
Missouri Med 67:595-598, 1970
fibrous tissue extended superiorly as far 4. Hardy J D , Timmis H H : Abdominal aortic
aneurysms: Special problems. Ann Surg
as the inferior surface of the diaphragm.
173:945-965, 1971
The aorta showed grade VII/VII ar5. Mundt ED, Darling RC, Alvarado RH, et al:
Surgical management of mycotic aneurysms
teriosclerosis. Microscopic examination of
and the complications of infection in vascular
sections of the aneurysm revealed, as well
reconstructive surgery. Am J Surg 117:460as the usual changes of arteriosclerosis,
470, 1969
6. Reichle RH, Tyson RR, Soloff LA, et al: Salnumerous aggregates of chronic inflammonellosis and aneurysm of the distal abdommatory cells throughout the entire thickinal aorta. Ann Surg 171:219-228, 1970












![[ PDF ] - journal of evolution of medical and dental sciences](http://s1.studyres.com/store/data/007915996_1-0ee8e2544a5731bc330695136ae2f65a-150x150.png)
